
Abstract
Crohn's disease (CD) is a well-known subset of inflammatory bowel disease (IBD) that results in patchy inflammation through the entire thickness of the bowel wall, with the ability to target virtually any part of the gastrointestinal tract, but most commonly affecting the area between the ileum and the cecum. While a bacterial origin of Crohn's is well speculated, it is difficult to pinpoint what drives inflammation in these subjects, particularly the flare-ups or the sudden symptomatic intensification or recurrence. This review aims at tracing the etiology of CD back to diet, particularly fried foods, a known aggravator of symptoms. Based on the reactions that frying entails, the chemical composition of the food is altered in ways that can lead to maldigestion and inflammation. Current evidence suggests a direct dietary role in the inflammation underlying CD or the flare-ups. The presented review focuses on an underresearched, yet, very applicable topic. We suggest that emphasis should be put on dietary alteration as a means of treatment for patients with CD to supplement current therapy for optimal results. With the widespread popularity of fried foods, it is important to raise awareness about the potential negative outcomes that are prevalent worldwide.
Introduction
Fried foods, in some form or another, have become dietary staples all around the world due to the proliferation and popularity of restaurants and fast food chains that attract customers with their appetizing, convenient, and relatively inexpensive menus. Frying simply involves submerging a food item in hot oil until it reaches a safe minimum internal temperature. Frying is not solely attributed to fast food restaurants, however. Such food, in the form of chips is also widely available in grocery stores. In addition, at home, we often substitute deep frying with sautéing, stir frying, pan frying, shallow frying, and par frying with the notion that these are safer alternatives. 1,2 The newest addition is air frying, which may involve much lesser quantity of oil. While these alternatives could affect the amount of oil that might be associated with the processed food, they do not in any way influence the chemical processes taking place. In fact, there might be greater levels of toxic products associated with larger pans and shallow oil as opposed to deeper pans with limited exposure to outside air. The frying process sounds simple, but the chemical composition of both the food and oil undergoes changes due to complex reactions. 3
Frying is a multifaceted cooking procedure that requires more attention than it receives in terms of the various chemical changes occurring. Heat is one factor that singularly requires much consideration. 1,3 Different types of oils used for cooking are represented in Figure 1. The U.S. Department of Agriculture (USDA) recommends different frying temperatures for different oils, but seldom are the users aware of this. If the oil is heated for too long, is exposed to a large surface area, is repeatedly used for frying, is predominantly polyunsaturated, or the food contains high carbohydrates or proteins, the oil can differentially modify the food chemically with cooking. Upon heating, it is also important to choose oil that is stable enough to prevent its reaction with oxygen.
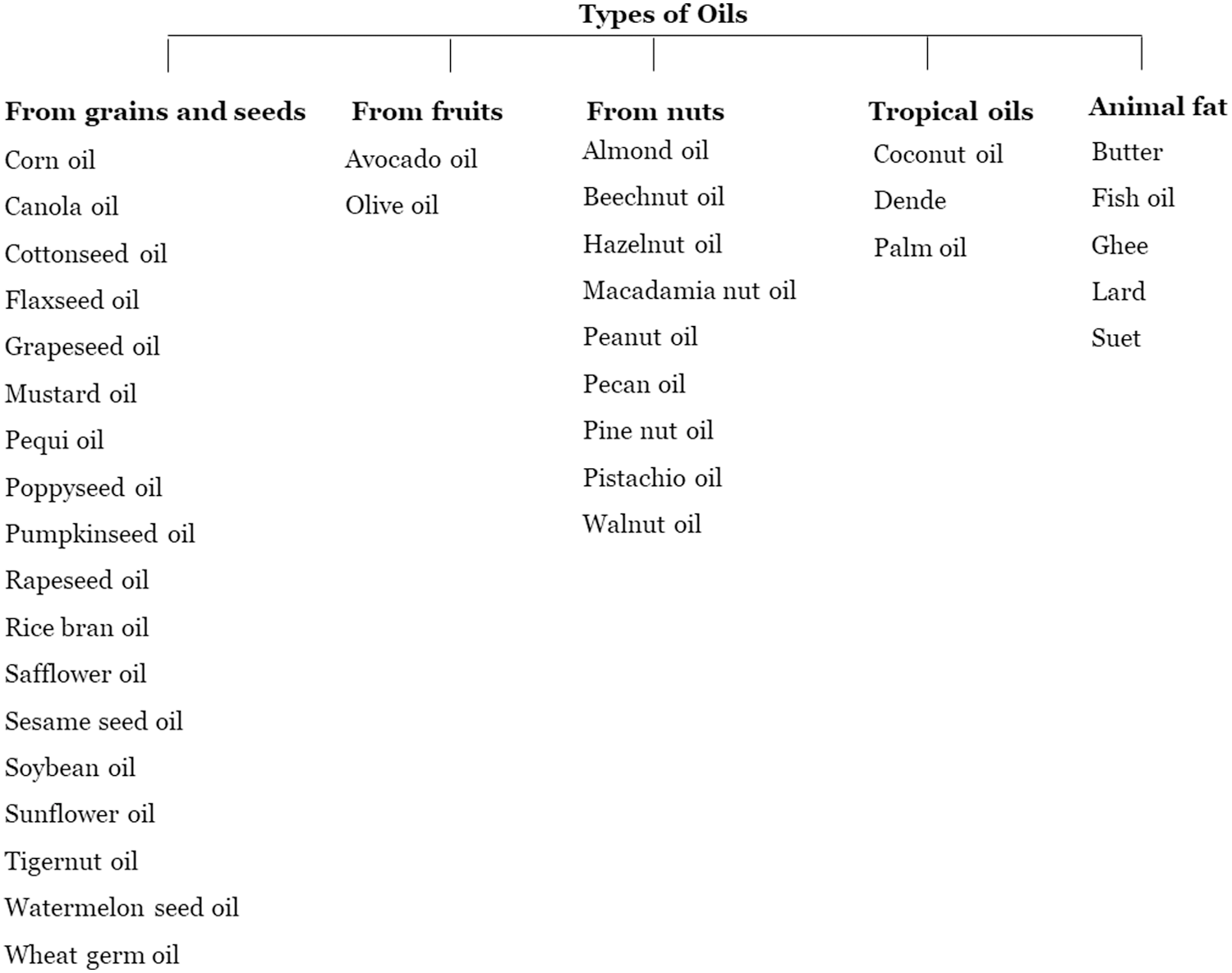
Various types of oils used in cooking.
Frying Reactions
The major reactions (Fig. 2) that occur during the frying process are oxidation, hydrolysis, polymerization, fission, and browning. 1 –3 Oxidation proceeds through free-radical chain reactions that lead to oil rancidity and eventual food deterioration upon auto-oxidative reactions accompanied by secondary reactions with oxidative and nonoxidative character. In contrast to the stability, the rate of fatty acid oxidation is positively correlated with the degree of unsaturation. The double bonds, characteristic of unsaturated fats, react with oxygen and subsequently produce harmful by-products upon heating. Recent studies have shown that heating unsaturated oils such as sunflower and soybean oils generate genotoxic and cytotoxic aldehydes such as 4-hydroxy-(E)-2-alkenals and 4,5-epoxy-2-alkenals. 1 It has to be emphasized that while polyunsaturated fatty acids (PUFA), particularly, fish oil-derived polyunsaturated fat, are preferable oils for healthy cooking, they are uniquely prone to oxidation-induced decomposition. Hydroperoxides, derived from the oxygenation of PUFA, and their degradation products are responsible for the malodorous scent and rancidity resulting from the reaction of fatty acids with oxygen. While some of the products derived from peroxidation are foul smelling, alerting the user of rancidity, others can enhance the flavor of the food material and give the user a false sense of a “good” cooking process.
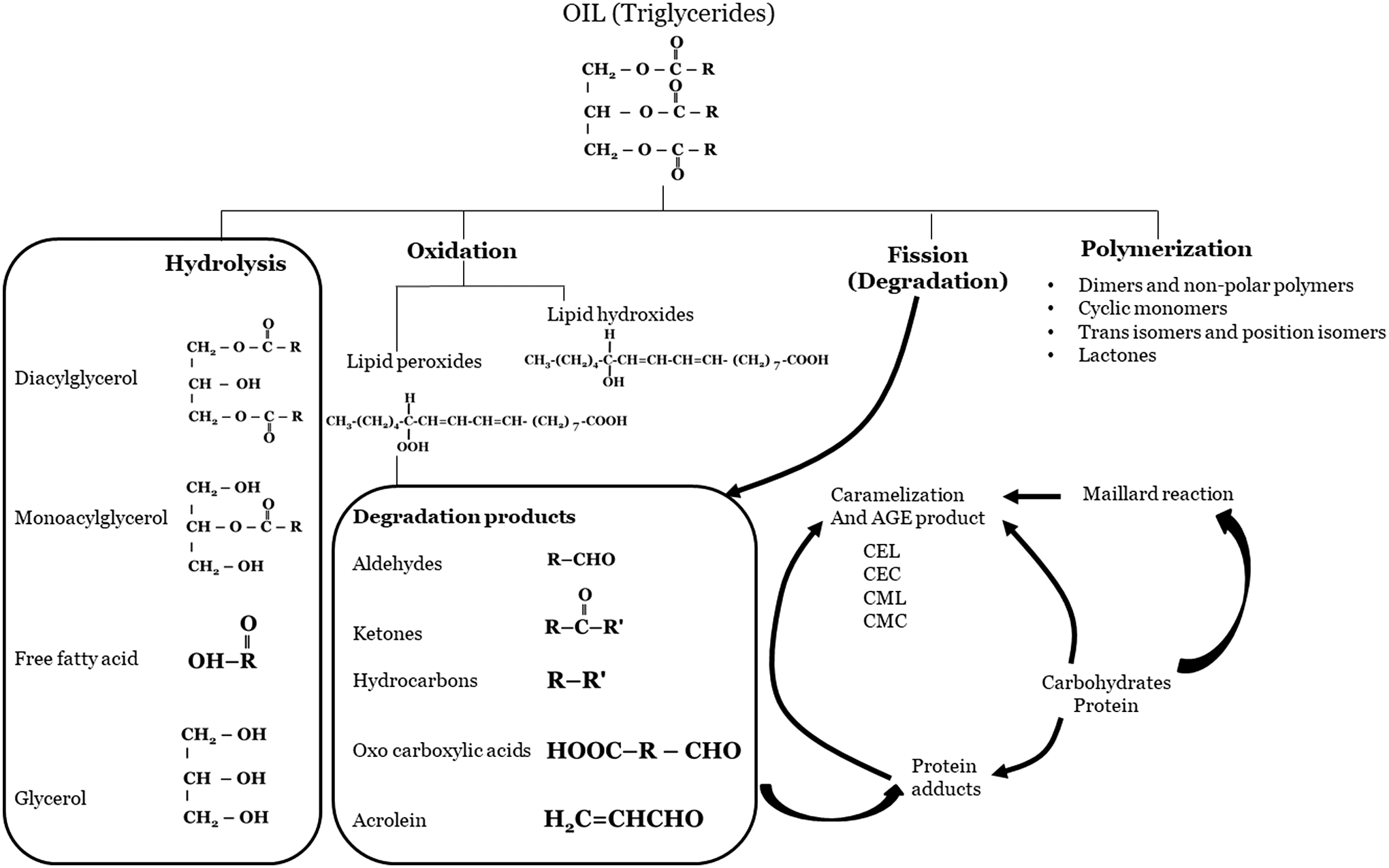
Major reactions during frying process of oil. CEL; carboxyethyl lysine; CEC, carboxyethyl cysteine; CML, carboxymethyl lysine; CMC, carboxymethyl cysteine.
Not only can oxidation change the taste of food but it can also aid in the development of further reactions that deplete the nutritional value of the food, including the depletion of antioxidants. Hydrolysis is one such reaction, in which the free fatty acid content contributes to an off-flavor. The resulting flavor makes the oil less acceptable for frying. 2 Moreover, a myriad of changes in carbohydrates, e.g., Maillard reaction, generates countless other oxidation products, derived from the food materials.
Overall, as the number of frying using the same oil increases, the free fatty acid content increases as well. 4 In addition, polymerization of oil produces several changes that affect oil composition as well as physical properties. 5,6 Polymerization causes accelerated oil degradation, increased oil viscosity, decreased heat transfer, foam production, increased oil absorption of food, and undesirable food coloration. 7,8 Nonenzymatic browning can either lead to pyrolysis of sugar or the Maillard reaction. In particular, the Maillard reaction is related to fried foods popularized by fast food chains that in most cases forego safety guidelines. While this reaction occurs around 284–329°F, if temperatures rise above 356°F, toxic or carcinogenic byproducts such as acrylamide can be released. 3 The reaction products include low molecular weight chemicals such as aldehydes, ketones, dicarbonyls, acrylamide, heterocyclic amines, advanced glycation end products (AGEs), and so on. Even though AGEs are low molecular weight compounds, AGEs mostly interact with macromolecules in foods as well as in biological systems. In recent years, biological AGEs were thought to be harmful for health and were considered to be causative factors for various kinds of diseases. Sato et al. 9 classified these AGEs into six groups. According to these studies, AGE-1 group are generated from glucose through Schiff bases and Amadori products, AGE-2 are from glyceraldehyde, AGE-3 are from glycoaldehyde, AGE-4 and carboxy ethyl lysine are from methylglyoxal, AGE-5 and carboxy methyl lysine are from glyoxal, and AGE-6 are from 3-deoxy`glucosone. The final step of the reaction produces flavor compounds and melanoidins, which work to brown high molecular weight compounds. List of toxic products released during repeated heating of oil has been represented in Table 1.
Different Processes That Occur During Repeated Heating of Oil
The Maillard reaction occurs readily in foods and biological systems. Since the Maillard reaction products exist abundantly in many foods, the effects of these products on consumers of such foods are of concern.
Diet's Contribution to Health
Diet is a multifaceted component of life that plays a large role in health determination. 10 Fried foods that are exceptionally high in saturated fats (as a result of depletion of PUFA) and high peroxidized fats' decomposition products are of particular concern as they are a source of possible inflammation. Many studies have reported the proinflammatory nature of peroxidized fat and their decomposition products (e.g., aldehydes) in addition to the anti-inflammatory nature of polyunsaturated fat. 11 –14 For example, the breakdown of peroxidized lipids into aldehydes, which chemically modify proteins and other cellular components, has been well documented. 15 –17 Although the mechanism(s) by which aldehydes are generated from peroxidized lipids are still unclear, both free-radical dependent and independent mechanisms have been suggested. 16 –19 Although PUFA intake may be beneficial to health, such benefits may not translate into potential physiological effect if they are oxidized. Raw PUFAs may differently affect health compared with their oxidation-exposed counterparts, which form substantial amount of peroxides and other deleterious by-products. The various biological effects of peroxidized fat decomposition products have been represented in Table 2. 11 –19
Biological Effects of Peroxidized Lipids
HODE, hydroxyoctadecadienoic acid; HPODE, hydroperoxyoctadecadienoic acid; ONA, oxonanoic acid; OVA, oxovaleric acid.
The gut is the major tissue in the body that receives the ingested fat. As a result of lipolysis and digestion, most of the fat is presented to the gut as free fatty acid, monoacyl glycerol, and alcohols, such as cholesterol and retinol. The presence of peroxidized fat or their degradation products are likely to affect both the mucosal cells as well as inflammatory cells associated with the Peyer's patch or lymphatic follicles. Inflammation in turn can lead to several complications such as inflammatory bowel disease (IBD), including Crohn's disease (CD) and ulcerative colitis (UC). In both cases, there is dense infiltration of inflammatory cells at the site of disease activity. 20 Increased inflammatory stress also might lead to metabolic syndrome and obesity. Obesity and IBD similarly show moderately elevated concentration of inflammatory mediators both locally and systemically. 21 Recent studies also have pointed out increased development of atherosclerosis in mice fed a peroxidized fat diet compared with mice with similar levels of blood cholesterol, 22 –27 presumably attributable to inflammatory stress.
The possibility that diet more than just aggravates gut inflammatory diseases cannot be ignored. Studies show that the traditional clinical presentation of CD in underweight patients is now shifting to 1% more in those who are overweight or obese. 28 –30 Interestingly, higher obesity rates are seen in less developed and smaller nations as they move toward unhealthy fast food options such as fried foods in lieu of food scarcity and rising prices. The different prevalence rates of Crohn's in different parts of the world can be, in part, attributed to differences in diets overall.
Statistically, based on total population and IBD estimates, about 0.32% of the U.S. population and about 0.34% of the European population is living with IBD. 31,32 While traditionally Asian and European countries adhere to healthier diets than Americans, westernization is quickly shifting this trend as these countries and many others adopt western-style eating habits. The growth and spread of unhealthy fast food chains have provided a stimulus for such change. 33
While CD is commonly treated pharmacologically, diet alteration also plays a significant role in controlling flare-ups and symptoms. The Mayo Clinic suggests avoiding fatty fried foods due to their intestinal processing. 34 Intestinal inflammation resulting from CD leads to malabsorption and maldigestion; thus, eating fried foods can aggravate symptoms and lead to flare-up. In addition, fried foods are typically high in cholesterol, which is poorly absorbed compared with phospholipids and triacylglycerols. Cholesterol absorption is aided by the presence of dietary fat, particularly by fried fat, 35 and hindered by high fiber content as fiber binds bile salts and cholesterol, preventing proper absorption and premature transit into the colon. 36 In addition, high-fat dietary content can eventually lead to steatorrhea that can result from malabsorption diseases such as CD. 37 Frying food alters the composition of the food and leaves it in a completely different state. For example, the frying potatoes results in enhanced starch and fiber content due to the formation of resistant starch. 37,38 Thus, if the increased fiber content hinders cholesterol absorption that can lead to or be characteristic of disease such as Crohn's, then the increased fiber content of fried foods, resulting from the frying process, can be attributed as a possible cause of developing the disease.
In addition to peroxidized fat/fried food, the oxidation of dietary proteins during food processing, storage, and digestion also increases the oxidative stress in the intestine lumen, which might induce direct or indirect oxidative damage to the intestine mucosa. Several studies support the adverse effects of dietary oxidized proteins on intestine and other internal organs. For example, Zhu-qing et al. studies reported an increased levels of oxidative damage markers in blood in oxidized protein-fed mice. 39 Studies also reveal on association between in vivo protein oxidation and aging and disease, 40 which shed light on the role of dietary oxidized proteins as external sources of oxidative stress and disease. This can be explained by incorporation of oxidized amino acids into cellular proteins, which lead to cell dysfunction, apoptosis, and potentially disease. 41 Keshavarzian et al. 42 reported increased oxidant levels in IBD along with oxidation of tissue cytoskeletal proteins (carbonylation and nitration of actin and tubulin). Marked actin oxidation (>50%) was shown only in inflamed mucosa of active IBD, suggesting that the cumulative oxidative damage in the mucosa may be related to luminal prooxidant factors, such as dietary oxidized proteins.
Based on in vivo and in vitro evidence Xie et al., 43 proposed advanced oxidation protein products (AOPPs) as a novel pathogenic factor that influences IBD progression. Administration of AOPPs to normal mice resulted in AOPP deposition within the intestinal epithelial and inflammatory cells of the lamina propria, linking to intestinal injury. Similarly, Xie et al. 43 reported AOPPs deposition in intestinal epithelial and inflammatory cells in the lamina propria of CD subjects. These results confirm the ability of protein oxidation products to induce and facilitate IBD progression. 44
It has been identified that proinflammatory cytokines such as interleukin-2 (IL-2) or tumor necrosis factor-α (TNF-α) is also associated with the initiation and progression of UC and CD. 45 In contrast, cytokines with anti-inflammatory effects, such as IL-4, IL-10, and partly IL-13, also contribute to the pathogenesis of IBD. 44 IL-2 is produced by activated T-lymphocytes and potently stimulates lymphocytes, macrophages, and natural killer cells to produce variety of cytokines. The enhanced production of these cytokines might facilitate recruitment of immune cells to the lesion, whereby they become activated leading to mucosal damage by release of oxygen radicals, proteases, and cytokines. 45 –47 Impaired reactive oxygen species (ROS) detoxification has been associated with UC and CD, which might lead to upregulation of oxidases or altered mitochondrial function. Recent studies implied that cyclosporin, a potent inhibitor of IL-2 production by T cells, 48 has a beneficial therapeutic effect on chronic active CD. 39 In addition, these studies also suggested that IL-2 ligand effect is mediated by IL-2R, which was also found to be increased in subjects with active CD than UC.
Van Kampen et al., 49 showed IL-4 alone has the ability to act as a proinflammatory cytokine in the mucosa of the colon and could lead to colitis. Other studies 50 have also shown the involvement of IL-4 in colitis development. According to these studies, the development of colitis was of significantly lower in IL-4/IL-10 double deficient mice compared with IL-10 knockout mice, which developed severe colitis. These findings suggested that IL-4 might be directly involved in causing gut inflammation.
Our studies (unpublished) suggest that dietary peroxidized lipids might be involved in monocytes recruitment and their differentiation into macrophages by the induction of IL-4 and MCP-1 in intestinal tissues. This in turn might lead to increased TNF-α release by macrophages and correlates with granulomas formation found specifically in CD patients (Fig. 3). This process is also seen in chronic granulomatous disease (CGD). CGD is due to the inherited absence of one of the nicotinamide adenine dinucleotide phosphate (NADPH) subunits, which results in repeated infections and formation of granulomas in multiple organs, including gut. 51 –54 Thus, peroxidized lipids could be acting as an inflammatory agent and can induce gut granuloma formation in CD.

Schematic representation of peroxidized lipid-induced gut inflammation and its progression to granuloma. The red dotted line represents the separation of intestinal lumen and the blood. POL, peroxidized lipid; IE, Intestinal epithelial tissue; PP, Peyers patches; IL, interleukin; TNF, tumor necrosis factor; MCP-1, monocyte chemoattractant protein 1.
Oxidative stress has been considered a potential pathogenic factor in the initiation, progression, and severity of IBD, rather than the propagation of chronic inflammation in the intestinal mucosa. However, the underlying mechanisms are not yet known. Based on the existing literature, various types of antioxidants, such as ROS inhibitors, functional foods, micronutrients, herbal plant extracts, hormones, polyphenols, synthetic substances, and probiotics, are potential therapeutic substances that target IBD. Although further research is needed to confirm the efficacy of these capable drugs for their appropriate doses and administration routes, focusing on conventional medications and a combination of new antioxidant-enhancing therapies may attain better therapeutic effects in IBD and would shed light on beneficial clinical outcomes. Recommended and nonrecommended diet for Crohn's or IBD subjects is represented in Table 3.
Recommended and Nonrecommended Diet for Crohn's Disease Subjects
This review is focused on an area of research that requires much attention, but is overlooked. While clinical treatment of CD predominantly focuses on pharmacologic therapy, changes in diet should be made in conjunction for optimal results. Physicians must work to educate patients more about the causes of CD and potential dietary components that are linked to inflammation.
The conclusions based on this study present data that are conducive not only to the primarily focused CD but are also very applicable to other diseases that manifest themselves secondarily or caused directly by inflammation. Inflammation accounts for several illnesses such as asthma, arthritis, diabetes, cardiovascular diseases, Alzheimer's disease, Parkinson's disease, hypertension, hypercholesterolemia, and possibly even cancer. Thus, while often overlooked, inflammation is ultimately the root for much more than we commonly associate. Inflammation can directly cause the aforementioned issues, and CD can lead to further complication as a natural side effect. 55
The nutritional value of peroxidized fatty acid is currently unknown and thus one should be cautious of excess and chronic consumption. Nutritional value of food is enhanced by the nature of vitamins present, especially antioxidant ones such as vitamin C, E, and carotenoids. In food, peroxidation of fat can be enhanced by the loss of such antioxidant vitamins and minerals. These antioxidants are key players in reducing the risk of atherosclerosis, cancer, and ischemic heart disease, controlling blood sugar, retarding the development of Parkinson's as well as Alzheimer's disease, and protecting the body from environmental pollution. 56 Furthermore, these antioxidants also protect fatty compounds against oxidation of blood-borne components and cell membranes, and play a significant role in the homeostasis of cellular redox environment. 57,58
Evidence suggests an association between chronic intake of western-style foods (high fat, high carbohydrate, and low fiber) and the incidence of IBD. 59 The interaction of peroxidized fat with other common nutrients and drugs, especially those taken by patients with IBD patients, has not been studied. The ability of gut microbes to generate toxic aldehydes and other products from peroxidized fats has also not been studied. Our previous studies have shown that peroxidized fat could mimic bile acids in their ability to solubilize cholesterol. 35 Taken together with increased serum cholesterol found in peroxidized fat-supplemented animals 14,22 –27 and the ability of free cholesterol to induce inflammation, 60 it is likely that peroxidized fat could contribute to inflammation via multiple pathways. These pathways include (1) acting as a peroxide, (2) generation of inflammatory aldehydes, (3) generation of oxygen radicals upon further oxidation of aldehydes, (4) mononuclear cell recruitment that generate vast quantities of superoxide radicals, and (5) excess membrane cholesterol deposition.
Whether antioxidants could provide complete benefit to Crohn's subjects have not been well studied. Some studies have reported that antioxidants such as resveratrol and green tea polyphenols are beneficial for IBD; however, these have properties beyond antioxidant effects, and it is premature to conclude that the observed effects could be solely attributed to their antioxidant effects. 61,62 However, the vast quantity of oil used in deep frying as opposed to miniscule levels of antioxidants present in the oil during frying would not have any discernable effect on the oxidation process. Besides, our previous studies have documented that antioxidants do not affect the degradation of existing peroxides 63 ; thus, additional supplement of antioxidants may have little to no effect. Overall, subjects with IBD might be better advised to refrain from deep-fried food.
Footnotes
Author Disclosure Statement
No competing financial interests exist.