
Abstract
Prostatism and erectile dysfunction (ED) are highly prevalent and closely comorbid. Prescription treatments are limitingly expensive but robust in mechanisms of action (MoA). Nutritional supplements (NS) are low-cost but inadequately supported by evidence. Do any NS use robust MoA? Could their efficacy be amplified via dosing, concentration of active principles, and/or use in combination? The goal is to develop an effective NS for prostatism and ED using the MoA of prescription treatments. Literature reviews were conducted on dietary supplements for prostatism or ED and MoA of relevant drugs. The most promising NS employing these MoA were chosen. A pilot study of a prototype combination was conducted. A protocol was created for an adequate dose-response trial to test the NS combination in men with ED and prostatism. The main measures were response rates, International Prostate Symptom Score, and International Index of Erectile Function. For drugs, the MoAs best proven for prostatism and ED were nitric oxide augmentation, mild androgen inhibition, and anti-inflammatory effects. The following NS best simulate these MoA and are best supported for efficacy; for prostatism: beta sitosterol; for ED: panax ginseng, arginine, and citrulline. Pilot clinical data provided support. A plan for a formal dose-response clinical trial was approved by a central institutional review board. NS using effective MoA might suffice for prostatism and ED. Pilot testing of a combination NS with the best-supported MoA supported further development. A dose-response trial should be conducted using adequate doses of L-citrulline, beta-sitosterol, ginseng, and vitamin D3.
Introduction
Prostatism, i.e., symptomatic benign prostatic hyperplasia (BPH), is severe enough to require treatment in one-fourth of older men. BPH makes urination slow, difficult, urgent, and excessively frequent (Lower Urinary Tract Symptoms [LUTS]). Worse, by obstructing the bladder neck, it leads to bladder detrusor muscle hypertrophy then decompensation, poor bladder tone, and eventually hydronephrosis, injury to the ureters and renal pelvis, and renal insufficiency. 1
Professional care for prostatism is expensive; the total yearly costs in the United States were $4 billion 20 years ago, when fewer men were affected. 2 In 2016, 12 months of treatment with either of two representative drugs for LUTS, one generic (finasteride) and one newer (dutasteride) each cost in excess of 6000 euros. 3
The vast majority of older men with prostatism also have erectile dysfunction (ED). 4,5 Large multinational studies have established a clear, strong, independent link between LUTS and ED. 4,6
Like drugs for prostatism, drugs for ED cost billions of dollars annually, even though less than 10% of affected men get treated. 7,8 Shame, stigma, and embarrassment may limit help-seeking. Worse, many U.S. insurers have recently stopped paying for phosphodiesterase-5 (PDE5) inhibitors, sharply cutting the proportion of men seeking care. 9
One way to provide accessible treatment for prostatism and ED might be to deliver benign therapies without serial clinic visits or prescription drugs, via nutritional supplements (NS). In many countries, NS are virtually unrestricted. The lack of regulatory oversight intensifies competition, driving costs down. Low margins, however, limit budgeting for research. This in turn limits developing an evidence-based approach to treatment with NS. Low-cost internet-based trials to test NS could be a promising approach to solve this problem and will be discussed later in this article.
First, however, selection of promising NS is required. Drugs for LUTS and ED have helped open paths to rational treatment with NS by establishing biochemical bases for treatment—relevant mechanisms of action (MoA). This article pursues whether such pharmacology can be exploited for NS combinations.
Materials and Methods
Reviews of drugs and NS for LUTS and/or for ED and research on mechanism(s) of action relevant to such problems were gleaned from PubMed, dose response in men was determined if possible, strengths of evidence were assigned, and the most promising agents were chosen for a combination NS. Priority was assigned to NS with known positive effects on nitric oxide levels, mild antiandrogenic effects on prostate tissue, and/or anti-inflammatory effects. An open-label dose-finding pilot study of a prototype combination was conducted, measuring change via standard measures of LUTS and erectile function. Results were used to modify the formulation. A scale-up proposal was adopted for an adequate dose-response study to determine efficacy and safety via an internet-driven protocol.
Results
MoA of drugs for prostatism and ED
One MoA used for controlling prostatism, that of finasteride, dutasteride, and newer selective androgen receptor modifiers, is inhibiting prostate hyperplasia by blocking the effects of endogenous androgens, whether directly or via 5-alpha-reductase to minimize conversion of testosterone to the more potent dihydrotestosterone. 10
Two other MoA, for prostatism and for ED alike, are properties of the PDE5 inhibitors: relaxing lower urinary tract smooth muscle hypertonicity via the nitric oxide pathway 11 —and possibly anti-inflammatory effects. 12 Moreover, applying multiple MoA simultaneously—alpha blockade and PDE5 inhibition, or PDE5 inhibition and 5-alpha reductase inhibition—has been shown to have greater effects for prostatism and for ED. 13,14 (Some newer drugs use antimuscarinic effects for prostatism, 15 but no natural antimuscarinics for prostatism are notable. 16 ) Employing multiple, complementary MoA may be important for response because not even the approved drugs have large effects on prostatism 15 –19 ; the usual response criterion on the standard scale for prostatism, the International Prostate Symptom Score (IPSS), is a mere 25% reduction in symptoms. 19
Mechanisms and efficacy of supplements as therapies for prostatism
NS for prostatism supported by scientific reviews include beta-sitosterol, pygeum africanum (African prune or African cherry), serenoa repens (saw palmetto), and cernilton (rye grass pollen extract). 20 The first three may all rely on mild antiandrogenic effects. 21 The main effect of cernilton may be anti-inflammatory. 22
Pygeum africanum improved overall symptoms twice as likely as placebo did, though quantitative change was minor: nocturia was reduced by 19%, residual urine volume by 24%, and peak urine flow was increased by 23%. 23
Saw palmetto is not supported by most clinical trials. 24 However, the content of the putative active components, fatty acids and beta sitosterol, varies too much between saw palmetto products to rely on; content of these components was found to vary by a factor of 20 between various commercial preparations of saw palmetto. 25
Cernilton was tested in only two studies with quality issues. Available evidence suggests modest improvement in symptoms including nocturia. 26
Beta sitosterol, the best-known plant sterol in saw palmetto and pygeum africanum, is associated with significant improvement compared to placebo; see meta-analysis data, Figure 1A. The meta-analysis showed a mean superiority on the IPSS of less than five points (1/7 of the 35-point scale) over placebo, but there was an apparent dose response; see Figure 1B. About 135 mg/day (in divided doses) appeared more beneficial than 30 mg/day, and, across 2 trials, bested placebo by about 10 points on the IPSS. 27

Thus, the best-proven MoA for NS to treat prostatism seem to be mild antiandrogenic effects and possibly anti-inflammatory effects.
Mechanisms and efficacy of supplements for ED
Various NS are provided for ED, but convincing efficacy has not been demonstrated in controlled trials according to a recent review. 31 Another recent review focused on 10 top-selling NS for ED. 32 The reviewers' conclusions about efficacy and safety are shown below in italics. The current author's comments follow.
(1) Dehydroepiandrosterone (DHEA) given once a day was of benefit in one controlled study but not in another, in which DHEA was given twice a day. DHEA seems relatively safe as the data does not show a significant impact on hormone levels. The data are weak to suggest a benefit. DHEA is mildly androgenic and acts as a precursor of sex hormones, particularly testosterone.
While this MoA, androgen augmentation, might be of benefit for ED in hypogonadal men, it would not be expected to benefit eugonadal men. This MoA is the opposite of the mild antiandrogenic activity of proven pharmaceutical agents for LUTS/BPH (see previous section). The same issues also apply to fenugreek (immediately below).
(2) Fenugreek was beneficial in one study, in improving sexual arousal and orgasm. No adverse events (AE) were reported. Other studies also show this to be a safe supplement.
Safety is not necessarily assured; fenugreek is a teratogen and abortifacient. 33,34 Since this review was published, two studies have shown conclusively that the herb increases testosterone levels significantly. 35,36
(3) Ginseng was found effective for ED in two meta-analyses but trials were of low quality. Ginseng appears to be well tolerated but was infrequently associated with mild headache, upset stomach, constipation, rash, and insomnia and can lower blood sugar (caution in diabetics).
Panax ginseng is a traditional tonic for sexual function. Figure 2 shows a review of placebo-controlled clinical studies of P ginseng extract for ED. Consistently, positive effects were found on response rate across the 6 small trials (n given ginseng per trial, 19–45, median, 30; see Fig. 2). In the meta-analysis, P-value for the difference between ginseng and placebo was P < .0001. In the three trials using the International Index of Erectile Function (IIEF), 37 the unweighted average of the mean change was moderate with ginseng (6.6) and small with placebo (0.9; P < .00001). The trials used 600–1000 mg three times a day. No dose response is evident (Fig. 2). 38
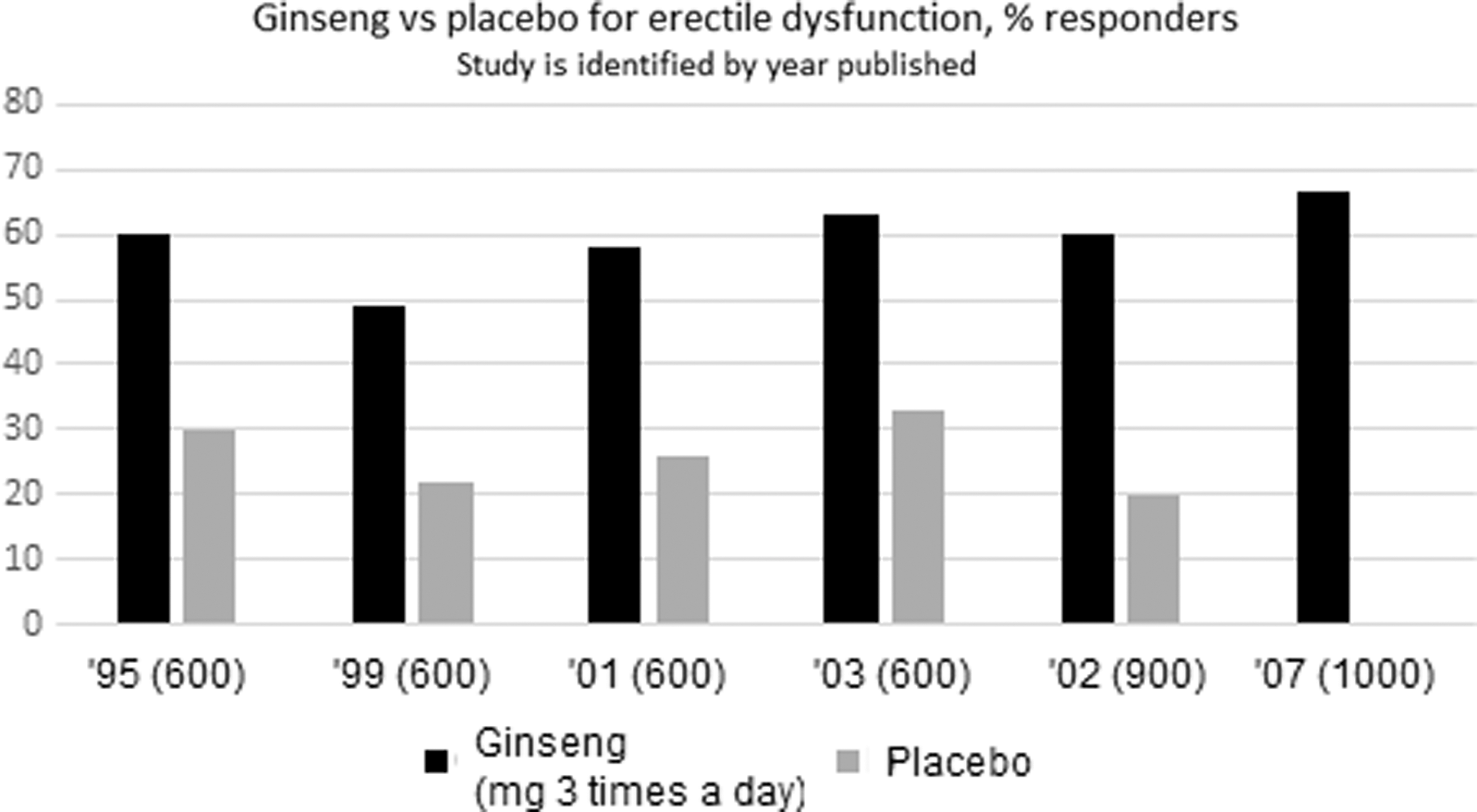
Response rate to P ginseng or placebo in men with erectile dysfunction. Studies are identified by year published and dose (given thrice daily) in mg. In the 2007 study, the % responders to placebo was 0.38.
Commercial extracts vary widely in the proportion of the active components, saponins called ginsenosides. 39 Variation between 4% and 5% ginsenosides is common. 40 Though 10% was claimed by one maker, independent analysis showed 4% ginsenosides. If the extracts used in the efficacy studies reviewed above contained 5% ginsenosides, the minimum effective dose may be as high as 30 mg of ginsenosides three times a day (90 mg/day). The MoA supported for ginsenosides for ED is dose-dependent relaxation of the corpus cavernosal smooth muscle triggered by increasing release of nitric oxide. Androgenic effects are disproven. 38
P ginseng has not been studied clinically for LUTS but is supported for prostatism by various animal studies. In the prostate, it prevented enlargement and suppressed expression of epidermal growth factor and alpha-1D receptor formation. In specific micturition-associated areas of the brain where nerve growth factor was overexpressed in BPH-induced rats, it reduced expression of nerve growth factor. 41,42 Also, ginsenosides are anti-inflammatory and thus are used to treat coronary artery disease. 43
(4) L-arginine (ARG) has the potential to improve erectile function by raising nitric oxide levels but 1500, 3000, and 5000 mg per day have been tested without consistent benefit. The supplement seems relatively safe but has been associated with a 10% drop in blood pressure. First pass hepatic metabolism inactivates orally administered ARG. L-citrulline (CIT) is an alternative, because it escapes first pass metabolism. One study showed CIT effective for erectile function and frequency of sexual intercourse.
CIT is readily interconverted in the body with ARG via the urea cycle. Both aid formation of nitric oxide via the enzyme nitric oxide synthase to relax the smooth muscle coat of bodily vessels (including the corpora cavernosa). This lowers blood pressure mildly, facilitates penile erection, and relaxes the male urethra to aid urine flow. 44 ARG improved erections in a creditable proportion of men with ED at daily doses of 2.8–6 g but not at 1.5–1.7 g; see Figure 3. 45 –48

Dose response to L-arginine, given as % responders. Three of five trials were open-label; placebo-controlled trials are noted by statistical conclusions (NS or *). The banded bar shows results from a clinical trial in which other herbs and vitamins were added; labeling recommends q.d. use but this clinical trial used 3 g twice a day.
A dose of 3 g or more may be needed to increase tissue [ARG] substantially because the usual diet provides about 5 g a day. ARG loses about 40% bioavailability in first-pass metabolism. CIT provides higher ARG levels and lasts a few hours longer in the body. 49
(5) Yohimbine has shown promise for improving male sexual function in some studies. It can cause hypertension, headache, agitation, insomnia, and sweating.
Two factors severely restrict the utility of yohimbine. The effective dose for ED, about 10 mg, may be inseparable from the dose precipitating significant hypertension in hypertensive patients, and the human half-life is only 0.6 h. 50,51
(6) Magnesium was discounted as plentiful in the Western diet. 32
However, the largest published study of magnesium intake found that a Western diet fails to provide enough magnesium. Men need about 400 mg per day, whereas a large (4257-participant) nationally representative sample of the USA found that the average intake was 326 for Caucasian men, 237 for African American men, and 297 for Mexican American men, a shortfall of about 20–40%. 52 Magnesium deficiency promotes atherosclerosis, endothelial dysfunction, and chronic inflammation, 53,54 and is a large risk factor for cardiovascular disease and diabetes, both of which are strongly associated with vascular ED. 55,56 However, no available studies have investigated the relationship between magnesium intake and ED or BPH/LUTS.
(7) Folic acid (FA) is popular in NS for ED, but no efficacy data were cited.
However, a strong relationship has been found between serum FA levels and ED, possibly due to an effect of FA on the metabolism of nitric oxide, homocysteine, and 5-hydroxytryptamine. In men with ED, FA levels were about half those in controls. 57
The reviewers also found the following popular NS ineffective for ED: maca, epimedium (Horny Goat weed), and ginkgo biloba.
Finally, Vitamin D is unmentioned by reviews of NS for ED, but it may be relevant. Up to half of the population worldwide may be deficient in vitamin D3. 58 Vitamin D deficiency mediates endothelial dysfunction. 59 Men with ED in the United States and China were found to have levels about half those in age-matched men without ED. The difference was highly statistically significant. 60 Like magnesium, vitamin D3 deficiency is strongly linked to chronic inflammation and atherosclerosis. 61 A recent uncontrolled study of erectile and metabolic parameters in 102 vitamin D-deficient men, mean age 53.2, found monthly high-dose ergocalciferol (vitamin D2) 600,000 IU for 12 months associated with improvement in mean (SD) IIEF-5 score from 13.88 (3.96) at baseline to 20.25 (3.24) (P < .01). 62
The Vitamin D3 receptor is also recognized as a target for development of drugs for BPH; receptor analogs exert beneficial effects on LUTS/BPH. 63 –65 Increased intake of vitamin D from diet and supplements is related to decreased prevalence of BPH. 66
See Table 1 for a summary of the more positive results with NS applicable to prostatism and ED.
Supplements, Dose Response, and Level of Evidence
Supplements for prostatism supported by meta-analysis of comparative clinical trials are limited to beta sitosterol and pygeum africanum. Supplements for ED supported by comparative clinical trials are limited to L-arginine (metabolically interconvertible with
ED, erectile dysfunction; BPH, benign prostatic hyperplasia; FA, folic acid; LUTS, lower urinary tract symptoms; BPH, benign prostatic hypertrophy; ED, erectile dysfunction.
A very recent review and meta-analysis of clinical trials of herbal supplements for ED also found positive results with ginseng, and mixed results with Tribulus (and saffron), but added one small study each on Pinus pinaster [n = 21] and Lepidium meyenii [n = 50] with what the authors considered very preliminary positive results. 69
Ingredients of an NS combination for male urinary and erectile function
Table 1 summarizes the NS that are backed for prostatism and/or ED by the preponderance of efficacy and safety results in comparator trials and by sharing the effective MoA of drugs: (1) Beta-sitosterol or p africanum to block prostatic androgen receptors; (2) Arginine or citrulline to raise nitric oxide levels; and (3) Panax ginseng to raise nitric oxide levels and exert anti-inflammatory effects.
Micronutrients with MoA similar to the above and probably needing repletion in men with prostatism also include vitamin D3, FA, and magnesium, but prospective trials of relevance are unavailable. Vitamin D3 deficiency stands out in linkage to ED and prostatism.
Formulation and testing of a combination
An initial formulation, and a pilot study using it in four men with LUTS, were done before the current review of supplements for ED and BPH/LUTS was completed. P ginseng and urea cycle amino acids (AAs) (ARG and ornithine) were included in the formulation, but not beta sitosterol. The protocol called for baseline and on-treatment IPSS, IIEF (five-item version plus two items on sexual desire),
37
and Patient's Global Impression of Improvement (PGII) self-ratings while testing the following supplements open-label in sequential periods of 1–4 weeks each, q.d. then b.i.d.: P ginseng extract 240 mg; rhodiola rosea extract 250 + 100 mg rhodiola rosea root in capsules (for putative adrenergic/arousing properties); tableted AA mixture of L-arginine 1800 mg and
IPSS results on the first subject tested, a 72-year-old man with moderately severe BPH/LUTS and ED, showed a reduction in score with the AA mixture or ginkgo plus the AA mixture, from baseline values of 22–25 to 12 after the NS combination was given twice daily, but no response with once daily administration (IPSS scores of 1–7 = Mild; 8–19 = Moderate; 20–35 = Severe. 70 ). Only the two b.i.d. regimens with the AA mixture improved the IIEF-5 by two points or more. Two subjects aged 49 and 51 with mild prostatism were not monitored as intensively but showed improvement in PGII with the AA/ginseng mixture. A 69-year-old subject with neurogenic LUTS did not benefit. Successfully treated subjects found that beneficial effects dissipated within a day after the last dose. Sexual desire item scores were unaffected by treatment.
In light of the above, the formulation was modified to provide per serving: 400 mg beta sitosterol (extract of phytosterols from soy or canola oil); 45 mg ginsenosides (P ginseng extract with 30% ginsenosides); 3 g
Plan for a developmental trial of the formulation
The next study is planned as an open-label randomized crossover dose-finding study of urinary and erectile function in older men using the modified NS combination. Two dose regimens will be compared: daily (q.d.) and twice daily (b.i.d.). The primary test population will be men with at least moderately impaired urinary function and ED. Secondary objectives are to test efficacy and tolerability in men with any severity of urinary and erectile symptoms but who seek improvement.
Efficacy measures will include the co-primary endpoints of IIEF-5 and IPSS; secondary endpoints are IPSS Quality of Life due to urinary symptoms and Volunteer's Global Impression of Change in erectile function. Safety measures include the primary endpoint of AE and the secondary endpoint of AE dropouts. The population to be studied is 228 men: 128 meeting severity criteria and randomized to take the NS once-daily or twice-daily first, and the first 100 other men who meet the minimal entry criteria. The sample size of 64 per treatment assigned first was chosen using a moderate effect size of 0.5 and an alpha of 0.05. 71 This effect size is conservative in reference to the data on beta sitosterol and panax ginseng reviewed above.
Subjects will be involved for 3 weeks: a day for informed consent and screening, 2–5 days for baseline/shipping of treatment, 1 week for treatment twice daily, and 1 week for treatment once daily, with the treatment sequence assigned randomly.
Subjects will be recruited, consented, and monitored via the internet. The feasibility of such trials for treating sexual dysfunction has recently been reviewed. 72 The same work also described the internet-driven informed consent process negotiated with a central institutional review board for this study.
Discussion
This article uses five working hypotheses: (1) that the pharmacology of drugs effective for prostatism and/or ED should apply to NS; (2) that the high correlation of prostatism with ED is a result of similar or the same pathogeneses, so natural supplements helpful for one of these disorders should benefit the other; (3) that employing multiple MoA should be more helpful than any single MoA; (4) that natural supplements can exert pharmacologic effects to an effective degree, that they are not simply placebos; and (5) conversely, that natural supplements are not well recognized as effective for prostatism and/or ED because they have been consumed at doses insufficient for pharmacologic effects or because the effects of single agents are too small.
This work shows that several natural supplements may possess the same three MoA as drugs known to relieve prostatism and/or ED: (1) raising nitric oxide levels with urea cycle AAs or ginseng, like the augmentation of nitric oxide levels by PDE5 inhibitors; (2) mild antiandrogenic effects from beta-sitosterol and possibly other phytosterols may simulate those of the pharmacologic alpha-2 reductase inhibitors; and (3) anti-inflammatory effects of ginseng may simulate those of the drugs known primarily as PDE5 inhibitors.
PDE5 inhibitors for ED also help prostatism. The converse is not so for apha2 reductase inhibitors for prostatism; they are associated with ED. 73 However, a PDE5 inhibitor (tadalafil) was shown effective to relieve ED in men already taking a reductase inhibitor (finasteride) and having ED. 74
We noted that combining multiple MoA augments the efficacy of drugs for prostatism. For ED, however, the high efficacy of the PDE5 inhibitors disfavors a need for augmentation. But, no NS has shown effects nearly as large as for PDE5 inhibitors; for ginseng, the mean increase in IIEF was 6.6 (vs. 0.9 for placebo) across controlled trials, whereas for sildenafil, mean response in one large controlled flexible-dose trial was 19.3 (vs. 3.7 with placebo). 75 Therefore, a rational combination of NS may be required to relieve ED satisfactorily.
The importance of dose sufficiency and clinically relevant effect size cannot be overemphasized. Very recently, a small crossover trial of men with ED tested the effects of one of the urea cycle AAs, CIT, at 800 mg per day, about ¼ of the minimum effective dose 32,45 –48,76 (plus resveratrol, another putative natural nitric oxide enhancer). 77 Efficacy was declared statistically significant versus placebo, but the mean change was only a 32% increase. In contrast, the known mean effect of sildenafil is a 94% increase, an improvement approaching the standard remission criterion of 25. 78 The rationale given for the low dose of CIT plus resveratrol was synergy expected from rat cavernosal data, but synergy requires an effective dose of each component. This exemplifies a broad, negative conclusion about extant natural supplement combinations for ED or BPH: that subtherapeutic doses of multiple components are usually used in an unsupported “shotgun” approach to synergy.
A limitation of this article is how tentative the conclusions must be due to the paucity of relevant clinical trials of substantial size with adequate (or any) control, both in the reviewed work and in the pilot study of a proposed nutritional combination that relied on an earlier, incomplete version of this literature review. Thus, this article is primarily for hypothesis-building. It deviates from prior reviews in concentrating on dose response and effect size, stressing quantitative findings over qualitative conclusions about the efficacy of NS for prostatism or ED. Perhaps such an emphasis, and low-cost but scientifically valid human developmental studies, can lead the field out of traditionalism and subjectivity into evidence-based alternative medicine for sexual health.
Conclusions
Rationally designed and adequately dosed NS combinations might help men with the linked, underserved problems of prostatism and ED. The best-known MoA of drugs for these conditions are nitric oxide augmentation for smooth muscle relaxation; mild antiandrogenic effects for inhibition of prostate cell multiplication; and possibly anti-inflammatory effects for inhibition of prostate growth. Among NS, the best evidence for simulating these MoA favors urea cycle AAs arginine and citrulline; beta sitosterol; and ginseng. Pilot testing of similar combinations supports further development. The utility of combining these MoA for additive effects will be tested in an open-label, dose-controlled exo-clinical trial. The doses will follow available dose-response data.
Footnotes
Author Disclosure Statement
No competing financial interests exist.