
Abstract
Bowel habits affect the quality of life (QOL) of patients with functional gastrointestinal disorders. This study evaluated the effects of reduced form coenzyme Q 10 (ubiquinol) intake on defecation frequency and stool form in patients with daily abdominal symptoms. This was a single-center, prospective, double-blind, randomized control study. Forty-one patients who had the daily symptom of constipation or diarrhea were randomly assigned at a 1:1 ratio to receive either ubiquinol (150 mg/day) or placebo for 12 weeks. Patients completed a daily diary to collect information regarding their numbers of defecations and stool forms according to the Bristol Stool Form (BSF) Scale for 7 days at baseline and 12 weeks. QOL was assessed using the 36-item short-form (SF-36) at baseline and 12 weeks. Twenty-one patients were assigned to the ubiquinol group, and 20 were assigned to the placebo group. At 12 weeks, the mean defecation frequency, compared to baseline, significantly decreased in the ubiquinol group (−0.1 times/day, P = .034) and increased in the placebo group (+0.3 times/day, P = .004). There was no significant change in the 12-week BSF Scale score of the ubiquinol group (+0.2, P = .123), whereas that of the placebo group was increased (+0.5, P < .001). The 12-week general health perception SF-36 score was significantly increased in the ubiquinol group (+3.5, P = .045), whereas there was no significant difference in that score in the placebo group (+1.2, P = .178). In conclusion, taking ubiquinol for 12 weeks decreased defecation frequencies and increased the QOL score, suggesting that ubiquinol may change the bowel habits and improve QOL in patients with abdominal distress.
Introduction
Functional bowel disorder (FBD), including irritable bowel syndrome (IBS), and functional dyspepsia are chronic conditions that negatively affect the quality of life (QOL) of patients and contribute significant socioeconomic burden. FBD is now highly prevalent worldwide. 1 Bowel habits and abdominal symptoms, including abdominal pain, bloating, and distention, markedly affect the QOL of patients with FBD. Because the overall mechanism of FBD is still unknown, the treatment of FBD focuses on managing symptoms with various strategies available, including pharmacotherapy, psychological therapies, and dietary medications, such as a low fermentable oligo-di-mono-saccharides and polyols diet, probiotics, and prebiotics. 2,3
Coenzyme Q 10 (CoQ10) is a vitamin-like antioxidant and an integral component of the mitochondrial respiratory chain for energy production and for preventing oxidative stress injury. 4,5 It has been reported that CoQ10 increases cyclic adenosine monophosphate and can improve mitochondrial function and inhibit oxidative stress. 6 In addition, several studies on the bioavailability of reduced form CoQ10 (ubiquinol) and oxidant form CoQ10 (ubiquinone) found that ubiquinol reached higher concentrations in the plasma, pancreas, and liver than ubiquinone. 7,8
The effect of CoQ10 supplementation on cardiovascular function, metabolic disease, neurodegenerative disorder, and rheumatoid arthritis has been investigated. 9 –13 However, no studies have investigated the effect of CoQ10 for gastrointestinal function. Regarding the gastrointestinal tract, recent experimental studies have revealed the anti-inflammatory effect of CoQ10 in the prevention of mucosal injuries in gastritis and colitis animal models. 14 –16 Furthermore, another study reported that CoQ10 improves QOL. 17 Therefore, we hypothesized that ubiquinol has an effect on bowel habits and abdominal symptoms because it has anti-inflammatory and antioxidative effects on gastrointestinal tissue and improves QOL. The aim of this exploratory study was to evaluate the effect of ubiquinol on bowel habits and abdominal symptoms in patients with daily symptom of constipation or diarrhea.
Materials and Methods
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board at Yuri Kumiai General Hospital approved the study protocol on September 11, 2015 before patient recruitment. Informed consent was obtained from all patients before they were enrolled. This study was registered with the University Hospital Medical Information Network Clinical Trials Registry (
Patients and study design
We conducted a prospective, placebo-controlled, double-blinded, randomized control study at the Yuri Kumiai General Hospital in Akita, Japan between September 2016 and April 2017. Advertisements for study recruitment were posted in the Yuri Kumiai General Hospital using posters between January 2016 and January 2017, and they targeted participants of the hospital's elderly health checkup program. Forty-one patients who fulfilled the inclusion and exclusion criteria were enrolled in the study. Inclusion criteria were as follows: (1) men and women over 60 years of age with stable disease and (2) those who had the daily symptom of constipation or diarrhea in a self-assessment. The exclusion criteria were as follows: (1) those with inflammatory bowel disease, (2) abdominal surgery, (3) mental illness or an addiction to drug or alcohol, (4) pregnancy, (5) breast feeding, and (6) the absence of informed consent.
Eligible patients were randomly assigned at a 1:1 ratio to receive either ubiquinol (150 mg/day) or placebo for 12 weeks. Randomization was performed using a permuted block method, with stratification by age and sex, using computer-generated random numbers. The ubiquinol and placebo capsules were specially produced by the same company (Kaneka Corporation, Tokyo, Japan). The placebo capsule has the same shape, color, and weight as the ubiquinol capsule. Ubiquinol and the placebo were sealed in identical aluminum bags. The patients were instructed to take three capsules of ubiquinol or the placebo with any meal.
Patients visited the Yuri Kumiai General Hospital at baseline and 12 weeks. When the patients visited (at baseline and 12 weeks), we assessed their vital signs and performed a physical examination and laboratory tests. All side effects were reported to the investigator.
Study outcomes
The outcomes of interest in this study were the changes in numbers of defecations, stool forms, abdominal pain, abdominal discomfort, abdominal bloating, and global assessment of the abdominal condition at 12 weeks from baseline. All outcomes were evaluated by daily diary entries. Patients were instructed to record a daily diary to collect information regarding their numbers of defecations, stool forms according to the Bristol Stool Form (BSF) Scale, 18,19 abdominal pain, abdominal discomfort, abdominal bloating, and global assessment of the abdominal condition for 7 days at baseline and 12 weeks. To assess the magnitude of changes in the abdominal pain, discomfort, bloating, and global assessment of the abdominal condition, validated self-administration scales were used. Abdominal pain, discomfort, and bloating were assessed by the visual analog scale (VAS), for which the score ranges from 0 to 100 mm (0 = no symptoms, 100 = the most severe symptom; a higher score means the worst abdominal symptom). Global assessment of the abdominal condition was also assessed by the VAS, for which the score range of 0–100 mm was a reverse scale of that for abdominal symptoms described above (0 = poor condition, 100 = excellent condition; a higher score means a better global abdominal condition). The VAS has been shown to be a valid and reliable tool for IBS. 20,21 In addition, the general health-related QOL was assessed using the 36-item short-form (SF-36). Patients received the SF-36 at their visits (at baseline and 12 weeks).
Statistical analysis
Because there was no previous data on the efficacy of CoQ10 for the change of numbers of defecations, stool forms, and abdominal symptoms at the time this study was designed, we were unable to estimate the sample size. However, we estimated that the number of eligible patients within the 12-month advertisement period would be 40. Hence, we planned to enroll 20 patients per group.
To evaluate the efficacy of the study, an intent-to-treat (ITT) analysis was performed. The ITT analysis was conducted for all patients who evaluated these outcomes at baseline. The changes in study outcomes from baseline to 12 weeks were analyzed using descriptive statistics. Baseline data of this study were based on patient data collected before randomization.
The Fisher exact test was used to compare categorical variables. The Mann–Whitney U-test was used to compare continuous variables. The Wilcoxon signed-rank test was used to compare continuous variables from baseline to 12 weeks. A P value <.05 was considered statistically significant. All analyses were performed using JMP 12.1 software (SAS Institute, Cary, NC).
Results
Demographic characteristics at baseline and 12 weeks
The demographic characteristics of patients at baseline and 12 weeks are shown in Table 1. Twenty-one patients were assigned to the ubiquinol group, and 20 were assigned to the placebo group. Baseline characteristics, including age, sex, and body mass index (BMI), were well balanced between the two groups.
Demographic Characteristics at Baseline and 12 Weeks
P < .05.
BMI, body mass index; CoQ10, coenzyme Q 10; SD, standard deviation.
Regarding adverse events within the 12-week study period, one patient developed constipation in the ubiquinol group, while one patient developed a skin rash in the placebo group; the patients were terminated from the study. In addition, two other patients dropped out of the study and could not be followed. Consequently, after 12 weeks, 19 patients in the ubiquinol group and 18 in the placebo group completed the study and were evaluated at 12 weeks. There was a significant difference in the plasma CoQ10 level between the groups at 12 weeks. Although there was no significant difference in systolic blood pressure between the two groups at baseline and 12 weeks, it was significantly decreased from 154 to 144 mmHg in the ubiquinol group (P = .006) for 12 weeks, while it changed from 151 to 148 mmHg in the placebo group (P = .399). There was no significant change in body weight and BMI after 12 weeks in either group.
Change in defecations and stool forms
The mean numbers of defecations per day at baseline and 12 weeks are shown in Figure 1. The frequency of defecation significantly decreased from 1.2 to 1.1 times/day (P = .034) in the ubiquinol group; in contrast, it significantly increased from 1.0 to 1.3 times/day in the placebo group. The BSF Scale scores at baseline and 12 weeks are shown in Figure 2. The ubiquinol group showed no significant change after 12 weeks in the BSF Scale score (from mean 3.6 to 3.8 points; P = .123), whereas the placebo group showed a significant increase in it from 3.3 to 3.8 points (P < .001).
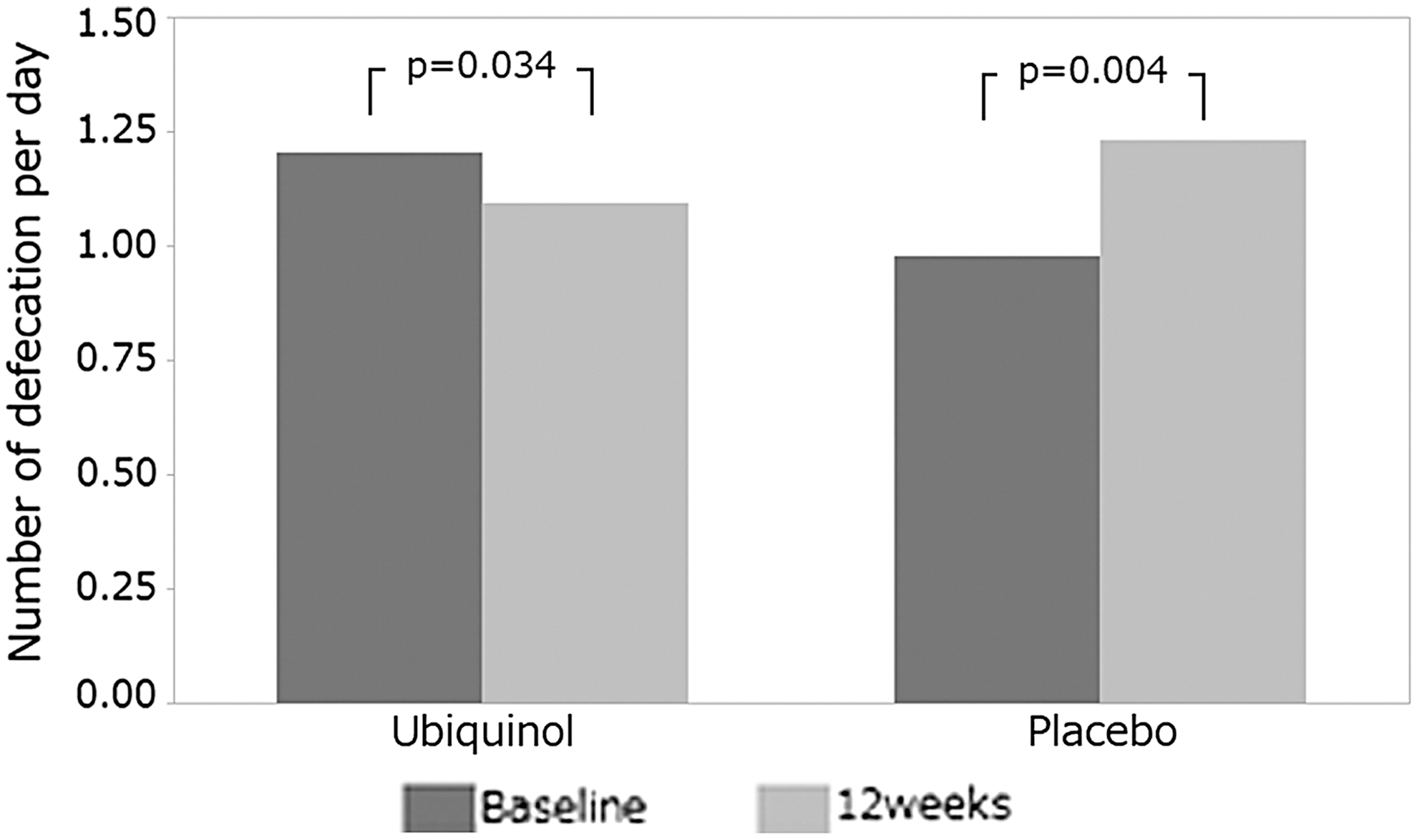
Mean numbers of defecations per day between baseline and 12 weeks in the ubiquinol and placebo groups. The mean numbers of defecations are significantly decreased from 1.2 to 1.1 times/day in the ubiquinol group; in contrast, those are significantly increased from 1.0 to 1.3 times/day in the placebo group.
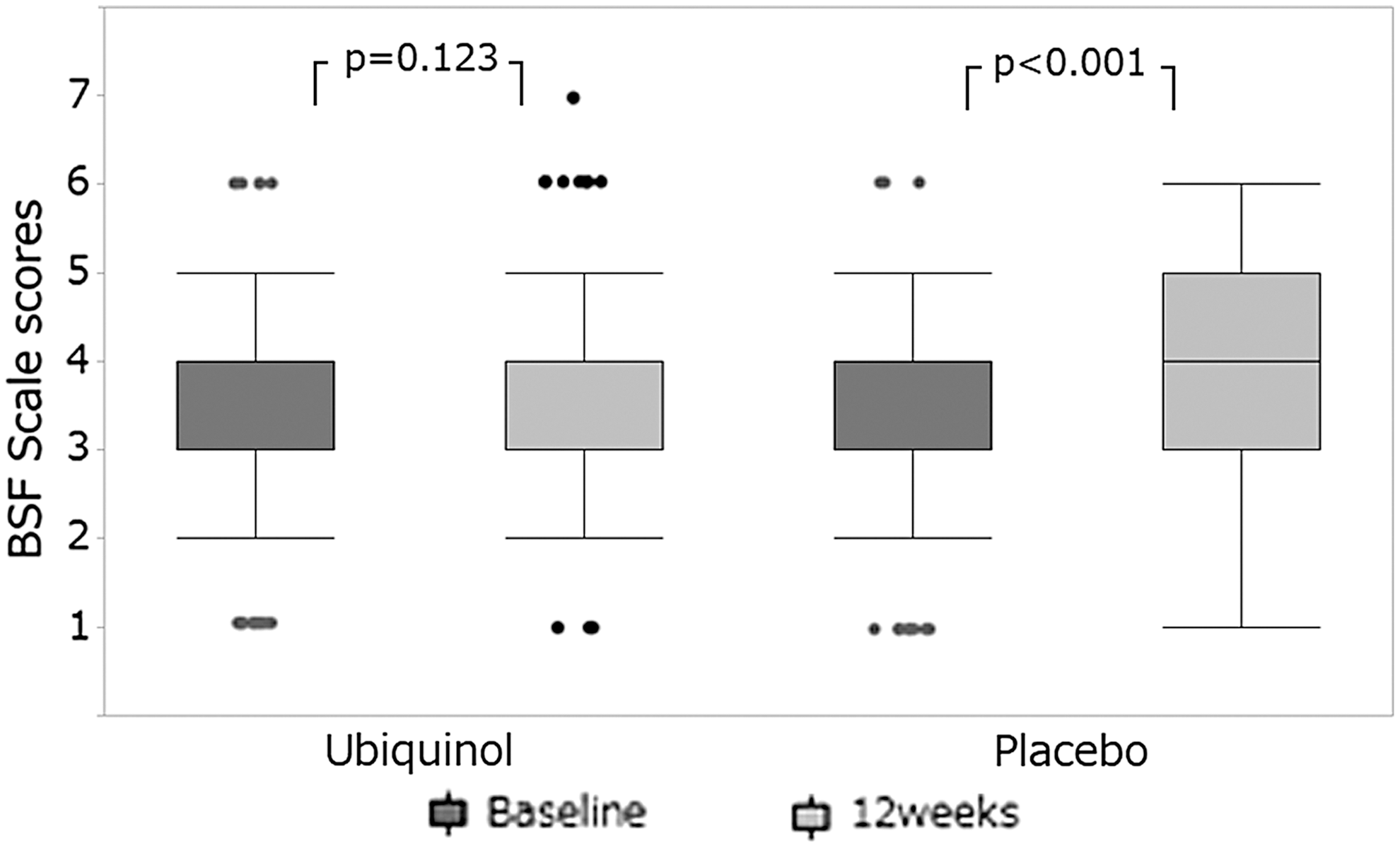
Scores of the BSF Scale between baseline and 12 weeks in the ubiquinol and placebo groups. There is no significant difference in BSF Scale scores in the ubiquinol group (from mean 3.6 to 3.8 points), whereas there is a significant increase of those scores in the placebo group (from mean 3.3 to 3.8 points). BSF, Bristol Stool Form.
In the subgroup analysis of patients who had daily symptom of constipation, which was defined as less than 1 time/day of defecation frequency, the mean number of defecations was not decreased in the ubiquinol group (from 0.7 to 0.8 times/day; P = .491); in contrast, this value was significantly increased in the placebo group (from 0.7 to 1.0 times/day; P = .004). In the subgroup analysis of the patients who had the daily symptom of diarrhea, which was defined as more than 1.5 times/day of defecation frequency, the frequency of defecation decreased from 2.2 to 2.0 times/day, but not significantly (P = .615), in the ubiquinol group; this value increased from 1.6 to 2.3 times/day, but not significantly (P = .313), in the placebo group.
Effect on abdominal symptoms and QOL
Concerning the VAS scores of abdominal pain, discomfort, and bloating at 12 weeks, there was no significant change from the baseline in both groups. In the ubiquinol group, the mean VAS score of abdominal pain changed from 3.3 to 7.8 (P = .182), that of abdominal discomfort changed from 13.9 to 12.0 (P = .136), and that of abdominal bloating changed from 10.8 to 16.6 (P = .207). In the placebo group, the mean VAS score of abdominal pain changed from 8.0 to 10.0 (P = .654), that of abdominal discomfort changed from 18.3 to 16.2 (P = .166), and that of abdominal bloating changed from 17.7 to 17.6 (P = .722). Regarding the VAS scores of global assessment of the abdominal condition at 12 weeks, there was significant change in the ubiquinol (from 70.7 to 78.6; P = .025) and placebo groups (from 67.1 to 81.3; P < .001). The general health perception SF-36 scores are shown in Figure 3. The general health perception SF-36 score at 12 weeks significantly increased from 47.2 to 50.7 (P = .045) in the ubiquinol group, whereas there was no significant change in the placebo group (from 46.9 to 48.2; P = .178).
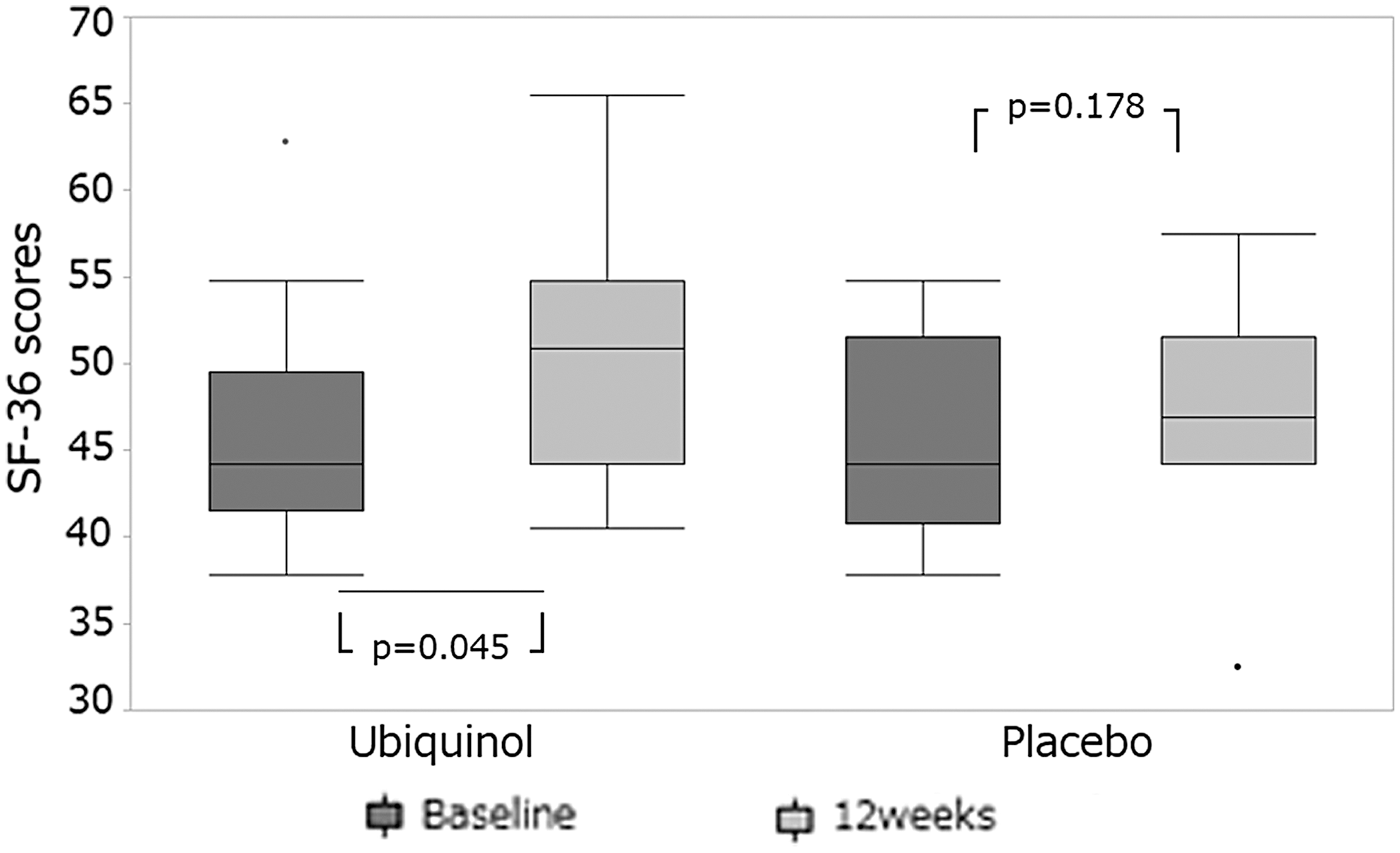
The general health perception 36-item short-form (SF-36) scores between baseline and 12 weeks in ubiquinol and placebo groups. The score is significantly increased from mean 47.2 to 50.7 in the ubiquinol group, whereas there is no significant difference in the placebo group (from mean 46.9 to 48.2) for 12 weeks.
Discussion
To the best of our knowledge, this is the first study to investigate the effects of ubiquinol on bowel habits, including the frequency of defecation and stool form, and abdominal symptoms. In this study, with the intake of ubiquinol for 12 weeks, the frequency of defecation significantly decreased without change of stool form in patients with the daily symptom of constipation or diarrhea. In addition, general health perception SF-36 scores were significantly improved for 12 weeks with the intake of ubiquinol.
There are a few studies on the effects of CoQ10 on the gastrointestinal tract. Karakaya et al. and El-Abhar reported a gastroprotective effect of CoQ10. 22,23 Possible mechanisms of gastroprotection attributed to the administration of CoQ10 might be as follows: it can act as an antioxidant directly by protecting biological membranes against oxidation, 24 CoQ10 may counteract vasoconstriction resulting from impaired endothelial nitric oxide (NO) production, 25 and CoQ10 might maintain gastric mucus thickness. Several other studies had proven the ability of CoQ10 to hamper the infiltration of neutrophils, as well as myeloperoxidase activity 26,27 ; thus, its effect may extend to suppress gastric mucosal neutrophil invasion. Regarding colonic mucosa, it has been reported that CoQ10 protects against ulcerative colitis in rats through antioxidant and anti-inflammatory potentials. 14 In this study, the ubiquinol and placebo capsules contained rapeseed oil, beeswax, and polyglycerol fatty acid ester. The frequency of defecation and BSF Scale score in the placebo group might have increased because of these lipid solutions. In the ubiquinol group, it was inferred that the effect of ubiquinol on gastrointestinal mucosal protection and anti-inflammatory potentials decrease the frequency of defecation and maintain stool form. Although the frequency of defecation decreased for 12 weeks with the intake of ubiquinol, this finding was not shown in patients with daily symptoms of constipation. That may be reason why the general health perception of SF-36 scores increased in the ubiquinol group in this study.
CoQ10 also decreased the expression of inflammatory mediators, including interleukin (IL)-6, IL-7, and tumor necrosis factor (TNF)-α in the colon tissue, and in contrast, increased the expression of anti-inflammatory mediators such as IL-10 and transforming growth factor-β. 15 Other studies have shown that inflammatory cytokines, including IL-6, IL-8, and TNF-α levels, increased in patients with IBS. 28,29 In addition, a strict correlation has been observed between NO production and gastrointestinal disease. 30 It has been suggested that elevation of inflammatory cytokines and NO plays an important role in the pathogenesis of IBS. Thus, a decrease in inflammatory mediators and NO production by ubiquinol might have reduced the frequency of defecation in this study.
Recently, the contribution of the gastrointestinal microbiota has begun to be explored for FBD. Subjects with IBS have a demonstrable alteration in their intestinal microbiota compared to healthy controls. 31 As some gastrointestinal microbiota are eukaryotes, they have mitochondria that produce adenosine triphosphate. The intake of ubiquinol possibly affects the energy metabolic pathway of some gastrointestinal microbiota through their mitochondrial respiratory chain. Because the gastrointestinal microbiota were not examined in this study, the effect of ubiquinol intake on gastrointestinal microbiota needs to be studied in the future.
Although this was a prospective randomized study, several limitations must be mentioned. First, this was a single-institution study that only included a small sample size of elderly patients older than 60 years of age. Thus, these findings may not be generalized to younger patients. Second, the patients' compliance with taking the ubiquinol or placebo capsule was not checked. In addition, although all patients enrolled in this study had the daily symptom of constipation or diarrhea, they were not diagnosed based on definite criteria such as Roma IV. 32 Large-scale multicenter studies of patients with IBS diagnosed based on definite criteria in which the sample size is calculated based on the data of this study are needed.
In conclusion, this prospective, double-blinded, randomized control study showed that taking ubiquinol (150 mg/day) for 12 weeks significantly decreased the frequency of defecation without changing the stool form in patients with the daily symptom of constipation or diarrhea. In addition, it improved general health perception SF-36 scores. The use of ubiquinol may be effective for improving the conditions and symptoms of patients with constipation or diarrhea.
Footnotes
Acknowledgment
This study was supported in funding sources, technical assistance, and provision of reagents by Kaneka Corporation.
Author Disclosure Statement
S.S., T.G., C.K., and H.I. have nothing to declare; Y.M. and K.F. are employees of Kaneka Corporation, Tokyo, Japan.