
Abstract
Compound K (CK) is a metabolite of a saponin in Panax ginseng, formed from ginsenoside, a triterpenoid glycoside, by human intestinal bacteria. Lactobacillus paracasei A221 isolated from fermented food can hydrolyze (deglycosylate) the main ginsenoside, ginsenoside Rb1, and generate CK. However, the pharmacokinetics of L. paracasei A221 fermented ginseng (FG) and nonfermented ginseng (NFG) have not been investigated so far. The aim of this study was to investigate the pharmacokinetics of CK after oral administration of single doses of FG and NFG in healthy Japanese adults. An open-label, randomized, single-dose, two-period, crossover study was conducted in 12 Japanese healthy volunteers (five men and seven women, aged 40–60 years). All subjects were equally allocated into two groups and administered tablets containing FG or NFG. Until 24 h after the administration, blood samples were sequentially collected, plasma concentrations of CK were measured, and the pharmacokinetic parameters were calculated. We also expected restoration of decreased testosterone level as one of the beneficial effects of FG and measured plasma total testosterone concentrations in male volunteers. The means of Tmax, Cmax, and area under the concentration–time curve (AUC) were significantly different between the two groups. In the FG group, AUC0–12h (ng h/mL) and AUC0–24h (ng h/mL) were, respectively, 58.3- and 17.5-fold higher than those in the NFG group. Moreover, mean testosterone concentration in the FG group significantly increased 24 h after administration. These results showed that the main ginsenoside metabolite of ginseng, CK, produced by L. paracasei
Introduction
G
Intestinal bacteria have been suggested to play a role in the production of ginsenoside metabolites, in which bacterial enzymes cleave the oligosaccharide connected to the aglycone stepwise from the terminal sugar, to generate the major metabolites, such as 20S-protopanaxadiol 20-O-β-
Therefore, the individual differences in metabolite-producing potential are intrinsically related to intestinal microbiota that is suspected to affect ginseng efficacy. Differences in the genetic background and the dietary habits of the population may also be related to the microbiota and the efficiency. 9
Lactobacillus paracasei A221 isolated from fermented food can hydrolyze (deglycosylate) the main ginsenoside, ginsenoside Rb1, and generate CK. 3 CK is reported to be absorbed into systemic circulation and to have diverse intriguing biological properties. 7,8 However, there are no reported investigations of the pharmacokinetics of L. paracasei A221-fermented ginseng (FG) in Japanese subjects.
Therefore, the aim of this study was to investigate the pharmacokinetics of CK after the oral administration of single dose of ginseng fermented with L. paracasei A221 (FG) and nonfermented ginseng (NFG) in healthy Japanese adults.
We also expected CK to restore testosterone level that decreases with age in men by ingesting FG. It may be one of the beneficial effects of ginseng. Therefore, we examined the effect of FG on plasma testosterone levels along with the pharmacokinetics of CK.
Materials and Methods
Ethics and safety management
The experimental protocol was approved by the Ethics Committee of Nihonbashi Egawa Clinic (IRB No.16000016, Chuo-ku, Tokyo) and conformed to the ethical principles set forth in the Declaration of Helsinki. Voluntary written informed consent was obtained from all participants. The experiment was conducted under the management of medical doctors at Tokyo Skytree Station Medical Clinic (Director Toshiyuki Kaneko; Mukojima, Sumida-ku, Tokyo). This clinical trial is registered as UMIN-CTR as ID number UMIN000036260 and reception number R000034556.
Subjects
The demography of the participants of this clinical study is given in Table 1. The subjects were 12 healthy adults, between 43 and 59 years of age, who had not contracted past or present diseases related to the liver, kidney, endocrine, cardiovascular system, gastrointestinal system, lungs, blood, metabolism, mental health, and anemia; no subject had participated in other clinical trials within the past 3 months or took other drugs or supplements during the trial period.
Characteristics of Study Participants Before the First Administration
SD, standard deviation.
Materials
FG and NFG were provided by Nagase Beauty Care Co., Ltd. 10 Fibrous root powder, with an abundance of ginsenoside Rb1, was used as the raw material for FG and NFG. The supplement tablet (274.4 mg) consisted of FG or NFG (40.8 wt%) and edible excipients. This study intervention consisted of a single administration of six tablets. CK, ginsenoside Rb1, Rb2, Rc, Rg1, and Re contents were analyzed in the extract of FG or NFG by using high-performance liquid chromatography (HPLC) and detected at a wavelength of 203 nm. 11 HPLC chromatograms that quantify CK of FG and NFG are given in Figure 1. The ginsenoside compositions of FG and NFG are given in Table 2. The CK content of FG and NFG was 0.75 mg/tablet and 0.00 mg (not-detected)/tablet, respectively.
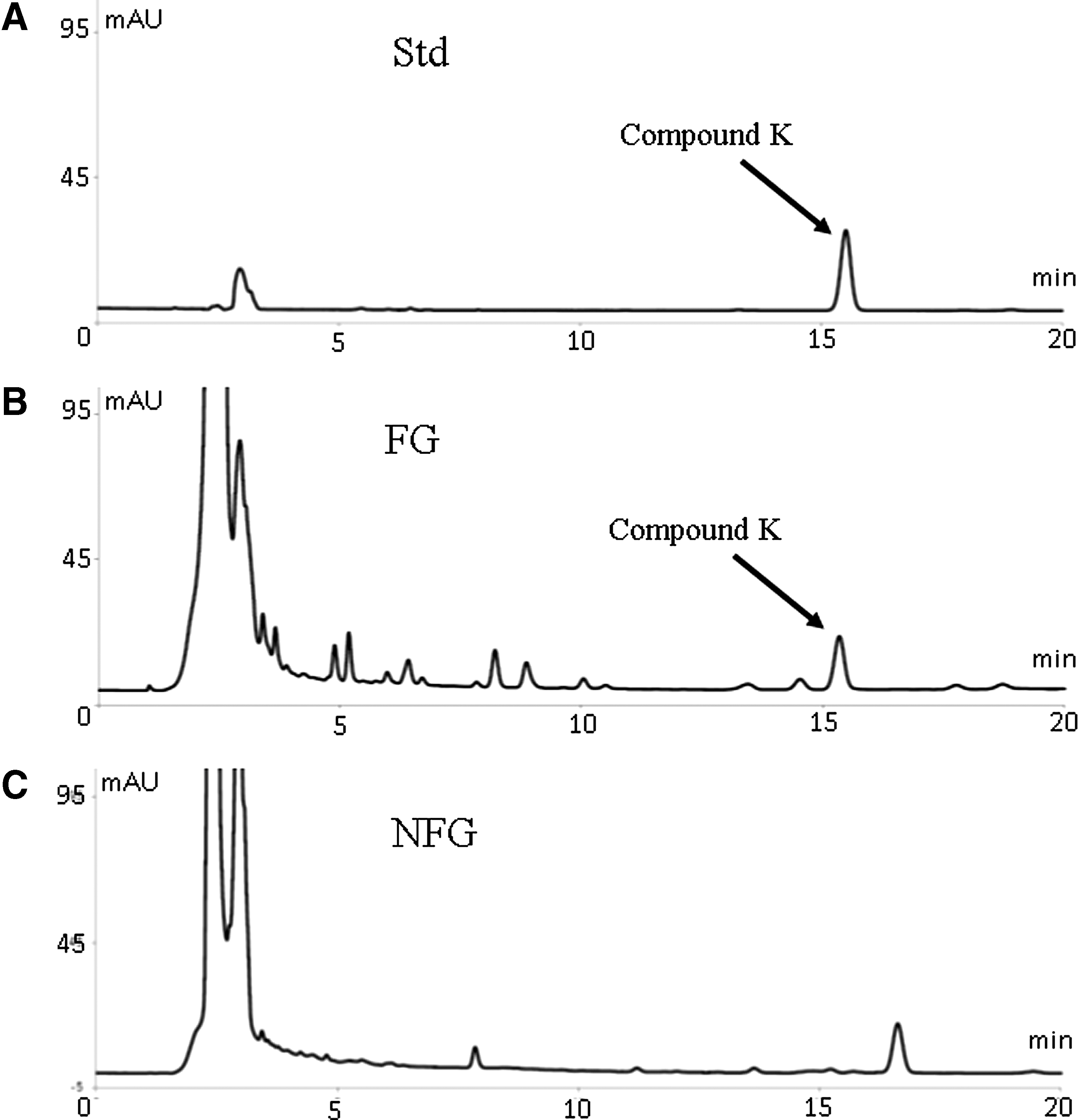
High-performance liquid chromatography chromatogram for CK quantitation.
Compositional Analysis of Fermented Ginseng and Nonfermented Ginseng by High-Performance Liquid Chromatography
FG, fermented ginseng; ND, not-detected; NFG, nonfermented ginseng.
Study design
An open-label, randomized, single-dose, two-period, crossover study was conducted to assess the pharmacokinetics of CK after the oral ingestion of FG or NFG. The subjects were allocated into two equal groups and orally administered six tablets containing FG or NFG with 200 mL water. Blood samples (2 mL each) were sequentially collected up to 24 h after administration (predose and at 1, 2, 3, 4, 5, 6, 8, 10, 12, and 24 h after ingestion) and plasma samples were prepared for the analyses. The subjects were fasted from 21:00 hours on the day before FG or NFG administration, which occurred at 08:00 hours; subsequently, the subjects were given a meal after blood sampling at 4 and 12 h. The washout period in the crossover condition was set as 1 week.
Analysis of CK in the plasma
The plasma concentrations of CK were measured by a validated liquid chromatography–tandem mass spectrometry (LC-MS/MS) assay. 12 In brief, 10 μL of 50 vol% acetonitrile, 10 μL of 500 ng/mL prednisolone, and 150 μL of methanol were added to 50 μL plasma. The sample was centrifuged (1900 g, 5 min, 4°C) and the filtered supernatant was analyzed. The LC-30AD system (Shimadzu) and QTRAP 6500 (AB Sciex) were used for the LC and MS/MS systems, respectively. The analytical column used was a Capcell Pak C18 MGIII, 5 μm, 2.0 mm I.D. × 50 mm (Shiseido) and the mobile phase consisted of gradient of 30% acetonitrile and 0.1% formic acid at 0–0.5 min and 95% acetonitrile at 2.5–3.5 min. The flow rate was 0.2 mL/min. The abundant product ions were at m/z 425.2 from the parent m/z 623.3 ion of CK. The desolvation temperature was 200°C and the ion capillary voltage was 5500 V.
Pharmacokinetic analysis
The plasma concentrations of CK were computed by Analyst 1.6.2 (AB Sciex) using simultaneously prepared calibration curves and the pharmacokinetic parameters were computed by Phoenix WinNonlin ver 6.3 (Certara) using a noncompartmental model.
Analysis of testosterone in the plasma
Plasma total testosterone concentrations in five male volunteers were measured using a validated LC-MS/MS assay similar to the method used for measuring CK. In brief, 10 μL of 50 vol% acetonitrile, 10 μL of 100 nmol/L phenacetin, and 150 μL of methanol were added to 50 μL plasma. The sample was centrifuged (1900 g, 5 min, 4°C), and the filtered supernatant was analyzed. The same LC-MS/MS system and analytical column that were used for analyzing CK was used for testosterone analysis. The mobile phase consisted of acetonitrile and 0.1% formic acid under the following gradient elution program: 25% acetonitrile at 0–1.0 min, 50% acetonitrile at 1.0–2.5 min, and 90% acetonitrile at 2.5–3.5 min. The flow rate was 0.4 mL/min. The abundant product ions were at m/z 96.90 from the parent m/z 289.21 ion of testosterone. The desolvation temperature was 600°C and the ion capillary voltage was 5000 V.
Results
In this study, no adverse events were observed and no clinically morbid manifestations or obvious contributions by the supplements were identified for all variations in the individual subjects.
Figure 2 provides LC-MS/MS chromatograms of CK in the plasma of a typical volunteer. The time course of the plasma concentration of CK after the administration of FG and NFG tablets (each n = 12) is given in Figure 3. At all time points between 1 and 24 h, there were significant differences in the CK concentrations between the FG and the NFG groups. The pharmacokinetic parameters of CK in plasma of the FG group and NFG group are given in Table 3. The mean values of the observed time of maximum concentration (Tmax), maximum concentration (Cmax), and the area under the concentration–time curve (AUC) were significantly different between the two groups. In the FG group, the mean Tmax was 2.2 h, which was indicative of very fast absorption. It should be noted that half-life (t1/2) and mean residence time (MRT0-∞) in the NFG group could not be calculated because the Tmax was late (16 h). The mean AUC0-12 h (ng h/mL) and mean AUC0–24h (ng h/mL) were 58.3-fold and 17.5-fold higher, respectively, than those in the NFG group.
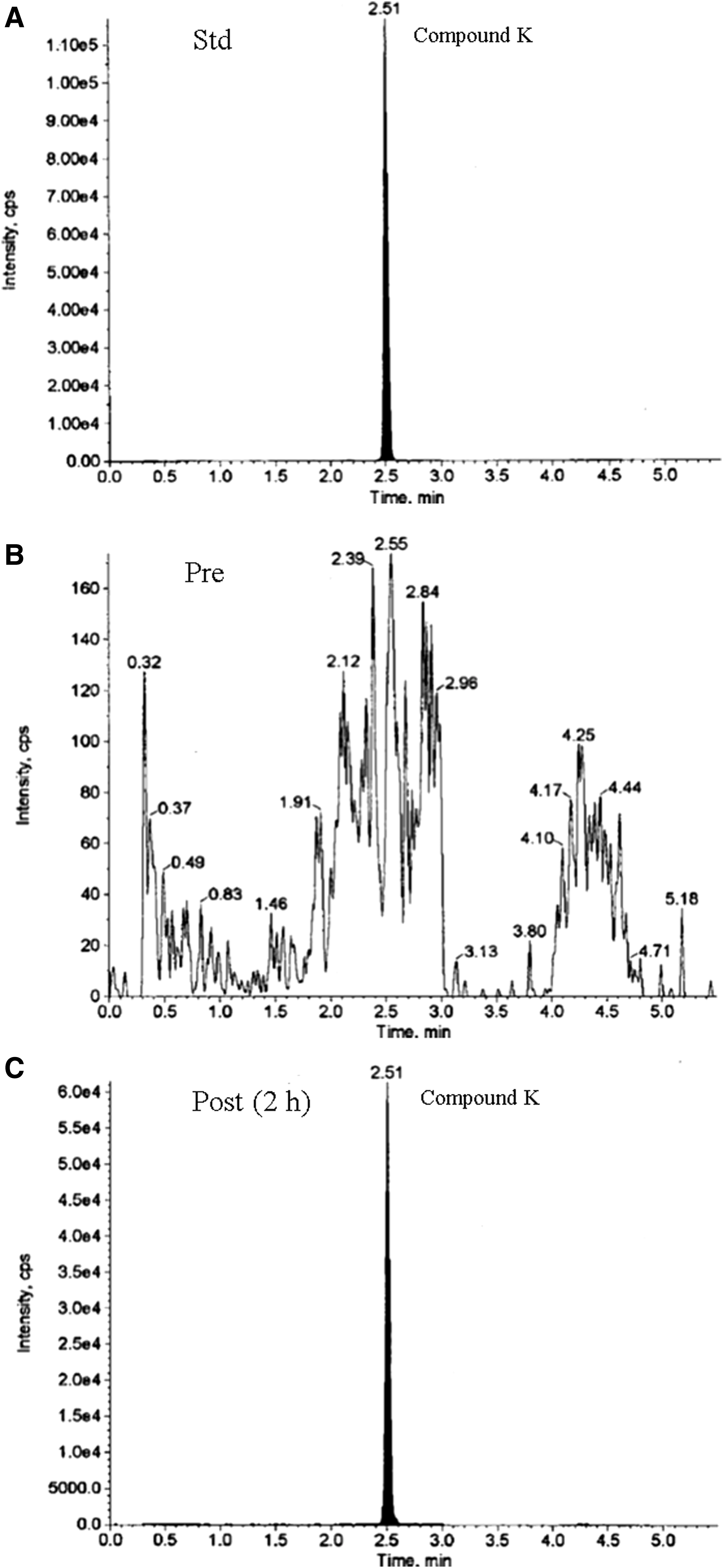
Liquid chromatography–tandem mass spectrometry (LC-MS/MS) chromatogram of CK analysis in the plasma of a typical volunteer.
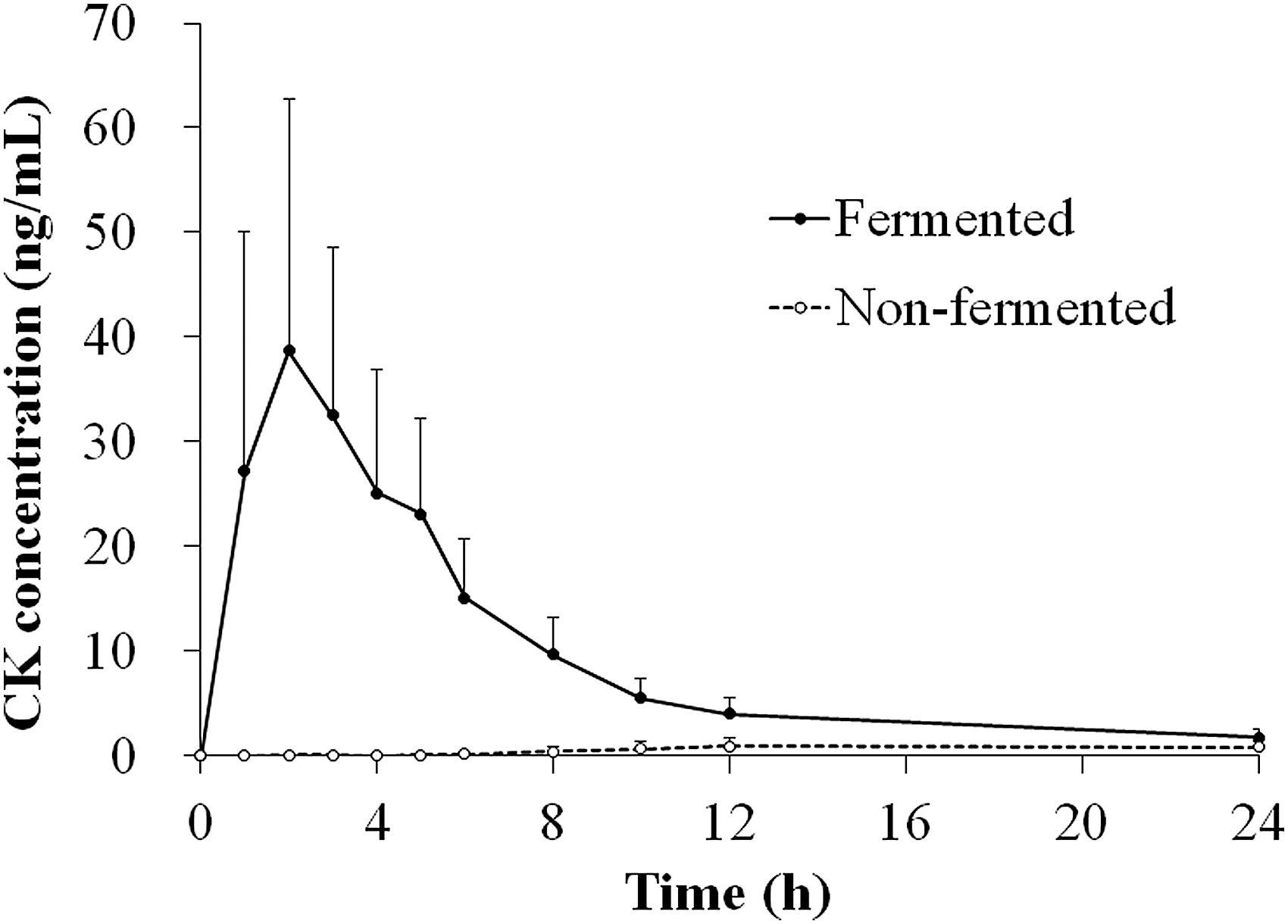
Plasma concentration–time profile of CK after the administration of fermented and NFG in healthy Japanese subjects (n = 12 for each). The data are shown as the mean values with the standard deviation.
Pharmacokinetic Parameters of Compound K in Plasma from Healthy Japanese Subjects
PK parameters include half-life (t1/2), time of the maximum concentration observed (Tmax), maximum concentration observed (Cmax), area under the concentration–time curve from 0 to 12 h (AUC0–12h), AUC from 0 to 24 h (AUC0–24h), AUC from 0 to infinite time (AUC0-∞), and mean residence time (MRT0-∞).
AUC, area under the concentration–time curve; PK, pharmacokinetic; MRT0-∞, mean residence time; NC, not-calculated.
Figure 4 provides LC-MS/MS chromatograms of testosterone analysis in the plasma of a typical male volunteer. Moreover, the mean total testosterone concentration in plasma of men in the FG group (n = 5) was significantly increased at 24 h after administration compared with the value before administration and the mean change ratio of the concentration at 24 h after administration in the FG group was significantly higher than that in the NFG group when preadministered concentrations were assumed 100% (Table 4). However, the mean total testosterone concentration in the NFG group was not significantly increased at 24 h.

LC-MS/male chromatogram of testosterone analysis in the plasma of a typical volunteer.
Plasma concentrations of the total testosterone 24 h after the administration of fermented and NFG and the change ratio in 24 h in healthy male Japanese subjects (n = 5). The change ratio after 24 h was calculated assuming a 100% preadministered concentration of total testosterone.
P < .05 (vs. preadministration using paired t-test).
P < .05 (vs. NFG using Student's t-test).
Discussion
Orally ingested ginsenoside is activated by intestinal bacterial deglycosylation and the process is crucial for its pharmacological actions. NFG contained ∼2% by weight ginsenoside Rb1. In the pilot study of three healthy men in their 50 sec, using the same conditions as this study, ginsenoside Rb1 was not detectable by LC-MS/MS in the plasma samples. CK metabolized from ginsenoside Rb1 in the intestine is one of the main absorbed forms and must be the active form, as reported. 7,8 However, intestinal bacteria vary vastly depending on the host conditions, such as diet, health, and stress. 5 Therefore, ginseng food products in which ginsenoside Rb1 is preconverted into CK with fermentation technology is considered to be useful because it avoids individual variations in activity. This study could therefore strengthen the idea that the fermented product is remarkably effective for the practical absorption of the active ingredient.
At present, most clinical studies that evaluated the efficacy or pharmacology of P. ginseng as a health food were performed with Chinese or Korean volunteers. 1 This study provides the first report of the pharmacokinetics of CK in Japanese subjects administered ginseng fermented with L. paracasei A221 or NFG. Our results in Table 3 and Figure 3 show that Tmax in the FG group was shorter and the absorbed amount was greater than those reported in a similar study from Korea that used ginseng extract treated with enzyme, although the intake of CK in this study was lower. 13 The reasons for this may include differences in the population, dosage form, materials, and fermentation/processing methods. Alternatively, because the gut microbial composition varies depending on different dietary habits in humans, 9 the intestinal microflora of the Japanese population may differ from that of the Korean population, and may tend to have lower metabolizing activity of ginsenoside Rb1.
We also expected restoration of the decreased testosterone level to be one of the beneficial effects of ginseng, and we found FG to have a higher efficacy than NFG. 14 –16 It is said that plasma testosterone level decreases with age in men, especially in middle-aged and older men, which leads to the disturbance of physical and mental homeostasis. 17 Our recent in vitro study examined the secretion of testosterone in primary-cultured mice testicular cells after the addition of FG, NFG, CK, and ginsenoside Rb1, and found that the concentration of testosterone in the cells treated with FG was much higher than that treated with NFG and CK, and also had secretory activity, whereas ginsenoside Rb1 had no activity (data not given). We confirmed that the decrease in total testosterone in the blood of the male stress mouse model was restored to a level close to that of normal mice by FG administration (data not shown).
The results in Table 3 indicate that male testosterone production or secretion by ginseng was significantly higher in FG than in NFG. Although further study is warranted to better understand the molecular mechanisms through which CK stimulates the production of testosterone, it is tempting to speculate that the increased absorption of ginsenoside metabolites induced by FG treatment in humans, particularly elderly men, could exert beneficial effects through the augmentation of testosterone signaling.
The results of this study showed that the main active ginsenoside metabolite of P. ginseng was absorbed after the administration of FG, but not NFG, and led to significantly higher plasma testosterone levels, which suggest the potential efficacy of ginseng fermented with L. paracasei A221 for the maintenance of health in healthy middle-aged and old Japanese adults.
Footnotes
Acknowledgments
The authors thank Kentaro Igami of Nagase Beauty Care Co., Ltd. for providing the FG. Tazuru Kikkawa was responsible for the production of the tablets. The authors are grateful to Toshiyuki Kaneko of Tokyo Skytree Station Medical Clinic, D.O., A.Y. of HUMA R&D CORP, and J.N., M.T., T.H., and K.A. for the preliminary study of the experimental design, recruiting volunteers, and performing the clinical tests. The authors also thank Tazuru Kikkawa of Kamakura Techno-Science, Inc. for performing the pharmacokinetic analysis and Kazuaki Iguchi for reviewing the article. The authors report no conflict of interest in the preparation of this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.