
Abstract
Federal guidelines recommend that food with hormone content fall below 1% of endogenous production in the subset of the population with the lowest daily production. The majority of dairy products are obtained from pregnant cows, which increase the level of hormones present. The purpose of this article was to perform theoretical evaluation of the quantity of progesterone in cow's milk based on fat percentages and to assess whether this was within the recommended range. Daily recommended dairy product intake from various countries worldwide was researched. This was compared to the concentration of progesterone previously identified in varying fat contents of cow origin milk to assess the amount of progesterone (mg/day) that would be consumed if the guidelines were followed. The maximum daily progesterone consumption suggested will be met by ingestion of 2.7 L, 1.42 L, 1.13 L, 940 mL, 810 mL, 650 mL of 0% (skim), 1%, 2%, 3.25%, 10% (cream), and 35% (whipping cream) fat liquid cow origin dairy product, respectively. Therefore, ingestion of the highest amount of recommended daily dairy intake fell below 1% of the daily endogenous quantity produced, except in the unlikely case of consumption of 650 mL of 35% fat. Studies demonstrating an effect of cow's liquid dairy product intake may need to be revisited, since levels of progesterone consumption remain within the recommended levels. However, it should be considered that ingestion of cow's milk might have a potential effect on the hormonal profile in patients; however, this seems unlikely.
Introduction
Guidelines exist for the consumption of foods and beverages with hormone content. 1 –4 These recommendations are based on maximum consumption of at most 1% of endogenous production, in the subset of the population with lowest daily secretion. 5 Compared to cow's origin liquid dairy products (CDPs) in traditional farming, commercial CDP contains greater amounts of estrone, 17β-estradiol, and progesterone. 6 To maximize dairy production, cows are maintained pregnant for the majority of their lactating lives, 6 and the level of these hormones is positively correlated to the trimester of pregnancy. 2 Gilman et al. reported that progesterone concentration in CDPs ranges from 4.9 to 20.4 nM based on percentage of fat in the product obtained in Quebec, Canada. 7
This practice of maintaining cows pregnant occurs in much of the world, including North America and Europe, 6,8,9 while it does not occur in certain parts of Asia. 6 However, it should also be noted that these hormones are also present at all other times as well in cows at similar levels, such as during the estrous cycle. Milk progesterone concentrations during diestrus are similar to those during a first trimester pregnancy in cows. Therefore, nonpregnant cows also contribute somewhat to hormone levels in milk based on their position in the estrous cycle.
Previous studies have shown that increased consumption of cow's milk may lead to lower semen parameters in males, particularly sperm morphology and motility. 10 Another study showed that an oral bolus of about 1000 mL of cow's milk with 3.5% milk fat (600 mL/m2) was demonstrated to reduce pituitary follicle-stimulating hormone (FSH) and luteinizing hormone (LH) production, after 30–60 min. 11 These two studies suggest that first pass hepatic metabolism of these consumed steroids can be overcome with large volume of commercial milk consumption.
Progesterone and estrone sulfate are fat-soluble hormones. In a previous study, a significant linear correlation of commercial cow's milk progesterone levels and fat content was noted (r = 0.8251, P = .04). 7 However, a study by Macrina et al. stated that the levels of estrone and estrone sulfate in cow's milk are well under 1% of the daily endogenous hormone production 5 and as such are likely safe. Given that serum concentrations of progesterone could hypothetically have effects on a patient population with conditions such as breast cancer, prostate cancer, fibroids, endometriosis, infertility, and recurrent pregnancy loss, evaluating the actual amount consumed is important.
The objective of this study was to perform a prospective theoretical evaluation of the quantity of progesterone in CDP based on varying fat percentages and government recommendations for consumption in various countries worldwide.
Material and Methods
CDPs of varying fat percentages: 0%, 1%, 2%, 3.25% and 10%, 35% had been previously prospectively analyzed for progesterone concentrations. 7 Two samples of each specific fat concentration and different commercial facility were analyzed and averaged. Milk products were obtained from a variety of different commercially available producers in Quebec, Canada (Agropur, Inc., Saputo, Inc., and Parmalat, Inc., all three cases located in Canada). Competitive enzyme-linked immunosorbent assay were run in duplicate with intra-assay and interassay coefficients of variation <6%. These obtained progesterone concentrations, as previously published, 7 were then used to calculate intake levels (for further information on these levels, review this article). The recommended CDP consumption from various countries worldwide (Canada, United States, France, and Germany) was researched (Table 1). 1,4,12,13 It should be noted that most countries do not have recommendations for CDP daily consumption. Instead these countries refer to these cited levels recommended by the authorities listed above. We attempted to gain knowledge of all countries' recommended CDP consumption levels and include any and all recommendations in our study.
Recommended Daily Dairy Product Intake by Country and Intake of Progesterone (mg/Day) in Varying Fat Concentrations of Milk Based on Specific Country's Recommended Daily Intake of Dairy Products
Based on our review, these values include the minimum (Germany) and maximum (United States and France) recommended intake of dairy products in developed countries worldwide. Other countries refer to these recommendations.
Based on the amount of progesterone in each fat level of CDP, calculations were performed to assess the daily amount of progesterone (mg/day) that would be consumed if current dietary recommendations were met. Calculations were based on the recommendation per day (mL) multiplied by the concentration of progesterone per mL based on fat content of the CDP. We indexed the molecular weight of progesterone to convert molar concentrations into milligrams. We used our previously determined progesterone concentration in CDP as a function of its fat percentage. Maximal recommended daily progesterone intake is 0.00416 mg/day (based on The European Agency for the Evaluation of Medicinal Products which state that men produce 0.416 mg of progesterone per day
2
and on the U.S. Food and Drug Administration (FDA) guidelines which state that no physiological effects occur when consumption is ≤1% of the endogenous quantities produced by the segment of the population with the lowest daily production
14
which is equivalent to 13.22 nmol/day). We subsequently used the aforementioned values to calculate the thresholds of consumption above which the progesterone ingestion in milk would be in excess of recommendations. The maximum level of progesterone daily consumption was calculated based on the progesterone in different fat CDPs. The progesterone molecular weight (3179.9 mg/nmol) was multiplied by the maximal daily progesterone intake recommended (0.00416 mg/day = 13.22 nmol/day) and then calculated progesterone concentration in CDP by fat percentage:
Volsafe—the recommended safety threshold of CDP volume consumption (mL/day); P safe—calculated recommended safety threshold of progesterone consumption per day (nmol/day); MWprog—progesterone molecular weight; and P conc—progesterone concentration in CDP as a function of fat content (%).
This study did not require ethical or IRB approval since it is a theoretical study and it did not use any patient data.
Results
In adults, the segment of the population with the lowest daily production of progesterone is males. At the lower end of the normal range, adult males produce 0.416 mg of progesterone daily. 2 This means that 1% of the quantity produced would be 0.00416 mg/day (13.22 nmol/day). Daily recommended CDP consumption levels and levels of daily consumption of progesterone based on dietary recommendations are listed in Table 1. With consumption of the highest fat (35%) CDP (cream), that is, whipping cream, and the highest recommended daily intake (710 mL/day), 1,4 the daily intake of progesterone reaches 0.004544 mg, only 0.0004 mg/day higher than recommended (Table 1). Consumption of 710 mL of 35% whipping cream on a daily basis is highly unlikely. By ingesting the recommended consumption of 3.25% (full fat) milk, the amount of progesterone consumed is under 1% of the daily quantity produced in the lowest producers in the adult population (0.001 mg/day lower than recommended). We subsequently determined how much of each fat concentration of cow's milk could be safely consumed based on progesterone levels (Fig. 1). It should be noted that 1% fat milk consumption exposed the drinker to elevated progesterone levels at <1.5 L/day, a large but not impossible to consume quantity. Clearly, this is a level which could be consumed particularly when you factor in cheese and other sources of milk consumption. Importantly, 0.95 L of whole milk (3.25% fat) consumption is required before you reach levels which may have biologic implications.
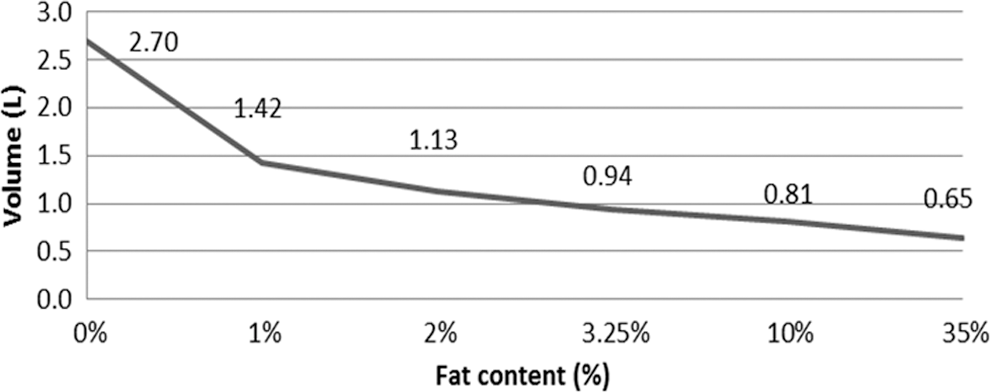
Estimated safe maximal liquid commercial cows' origin dairy product daily volume consumption as a function of fat content.
Discussion
This study shows that the recommended intake of CDP generally falls below what is the recommended hormonal consumption in adults. The exception is the unlikely situation in which only 35% fat CDP is being consumed in very high levels. As mentioned, previous studies in the literature have reported various effects of milk intake on physiologic processes, including sperm parameters and suppression of pituitary hormones.
Worsening sperm morphology and motility were noted with increased full-fat dairy intake. 10 However, the study does not include specific values on how much milk intake there was in these subjects; the subjects are divided into quartiles based on self-reported dairy product intake. The upper quartile of total dairy intake ranges from 4.33–13.26 servings/day; however, it is likely that the majority of the 47 subjects in this quartile were on the lower end of this range, given the narrow ranges of dairy intake in Quartiles 1–3. 10 That said, intake of 4.33 servings of dairy per day would be equivalent to 1082.5 mL per day (i.e., more than the recommended 710 mL), assuming that each serving size was 250 mL. It would be helpful to better understand CDP intake as related to sperm parameters had the article included the distribution of subjects across the quartiles. This article also failed to define the volume consumed as a serving of milk or dairy products. It is possible that whenever a dairy product was consumed this was considered a serving, including a 100 mL container of yogurt or a single slice of processed American cheese. Both would potentially represent less than 250 mL of milk. This study also failed to contemplate the fat concentration of the milk product consumed. All these factors could greatly alter the steroid amounts within that dairy product.
In a second article, there was both increased serum estrone and progesterone and decreased serum LH, FSH and testosterone, as well as increased urinary excretion of estrone, estradiol, estriol, and pregnanediol, after an oral bolus of full fat (3.5%) cow's milk. 11 In this study, the bolus in subjects amounted to ∼1000 mL of cow's milk, an unrealistic amount more than most people will drink at one time. Consuming 1000 mL of 3.25% milk leads to 0.004387 mg/day of progesterone, which is only slightly over the recommended 0.00416 mg/day, and thus most probably is an insignificant deviation. This study also examined ovulation timing in women. It found that in 80% of women, ovulation timing was unaffected, regardless of intake of successive boluses of milk (500 mL per night) starting on cycle day 2 for a total of 21 days. 11 There are also several issues with this article. Maruyama et al. present serum and urine hormone concentrations after a bolus intake of milk. A number of participants could not consume the entire quantity, yet their data were still used. The data for men, women, and children are combined, and the concentration values for the hormones measured fall within the normal physiological range. As well, these authors did not measure the hormone concentrations in the milk they used.
The amounts of cow's milk taken in with additional consumption by women are likely well below what is required to obtain pituitary suppression with the oral contraceptive pill. In contraceptive pills, the estradiol doses are in the 10–35 mcg range. Concurrently, the progestin dose in oral contraceptives is in the milligram range, which is about 300–900 times higher than we calculated as is ingested, with the highest recommended daily intake of 3.25% fat milk. It is possible that the combination of estrone, estradiol, and progesterone may exert agonistic effect on the pituitary gland; however, at these doses it is unlikely. It seems unlikely that these steroid doses seen with CDP ingestion would have pituitary effects, given the required quantities in combined oral contraceptive pills to obtain FSH and LH suppression. We previously attempted to reach pituitary suppression with 4 mg daily of estradiol valerate delivered orally at the start of menses and this failed. 15 Pituitary suppression was ultimately seen with a dose of 6 mg daily intake. 15 It should also be considered that the doses of hormones required to achieve pituitary suppression of 24 h duration are likely significantly higher than what may be needed to temporarily alter serum hormone levels without affecting ovulation. Therefore, intake of CDP products in lower levels may increase serum steroid levels temporarily and for short duration, but should not ultimately alter ovulation.
Given the relatively low levels of steroid intake, the study describing an association between milk consumption and semen parameters and the study demonstrating pituitary function effects should be repeated, to confirm the results. However, if these results are confirmed, further studies would be needed to determine the lower threshold of milk consumption at which temporary alterations in serum steroid levels can be achieved. It seems intuitive that if results are confirmed this level would be less than 1% of male daily production. In addition, should the effect be only brief, it would remain important to know if this brief effect modifies the disease course of any hormonally dependent conditions.
One weakness of this study is that progesterone levels could vary based on the country of origin of the milk consumed or in one local different time period. As such, Canadian milk may not be representative of milk in other countries. It is difficult to determine if these levels are consistent at different times and different locations since no other studies have evaluated the effect of fat concentration on progesterone levels in commercial CDPs. Most countries' commercial cow's milk demonstrates estrone and estrone-sulfate levels consistent with the second trimester of bovine gestation. 5,8,9 This level intuitively makes sense since companies combine first, second, and third trimester collected milk, in approximately similar volumes likely resulting in a mean level of second trimester. Second, it is unlikely that internationally (except in Asia) these hormone levels vary much in cows per trimester. Therefore, minimal variation in levels would be expected over time.
In conclusion, studies demonstrating effects of cow's milk intake may need to be revisited, since levels of intake achieved should remain in the safety margin of recommended intake levels and should not have likely caused what was demonstrated in those studies. It should be considered that ingestion of cow's milk might have a potential effect on the hormonal profile in patients; however, given the calculated levels across fat distribution in this study this is unlikely. Further studies are required to assess what physiologic role, if any, the intake of cow's milk in varying fat concentrations has in women, men, and children. Likely, consumption of cow's milk at levels currently consumed in our society is safe and probably do not exert hormonal effect on the human body.
Footnotes
Author Disclosure Statement
No competing financial interests exist.