
Abstract
The aim of this study was to analyze the efficacy of berberine taken alone or in other formulations (with silymarin or other mixtures) on dyslipidemia through a systematic review of the literature and a meta-analysis. A systematic investigation was conducted on 19 studies that were selected based on inclusion and exclusion criteria. Both controlled trials (n = 12) and cross-sectional trials (n = 7) were included. The following formulations were examined: berberine used alone (n = 5), berberine combined with silymarin (n = 8), and other mixture containing berberine (n = 6). A meta-analysis was performed using a fixed-effects model and meta-regression. Total cholesterol (TC), low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and triglycerides were considered. Moreover, possible associations of each parameter with age and the dose and duration of the treatment were analyzed. The data obtained showed a significant reduction in TC and LDL cholesterol for each formulation. A reduction in triglycerides was also observed for both TC and LDL but with a smaller impact. As regards HDL, a slight increase was observed, but it was not statistically significant. The formulation of berberine in association with silymarin was found to have the greatest impact on TC, LDL, HDL, and triglycerides. The greater efficacy of the formulation consisting of berberine associated with silymarin can probably be accounted for by the fact that the latter increases the bioavailability of berberine. However, it is necessary to carry out further clinical studies to better define the efficacy of the treatment and which patients show the best response.
Introduction
Dyslipidemia refers to an alteration of plasma lipid levels compared with the norm, in particular, an increase in cholesterol and/or triglycerides, or low-density lipoprotein (LDL). 1 Dyslipidemia represents an important risk factor for the development of atherosclerosis and cardiovascular diseases, 2 the main cause of mortality in western countries. 3 In this regard, it is reported that dyslipidemia causes four million deaths every year. 4
Hypercholesterolemia, hypertriglyceridemia, and low levels of high-density lipoproteins (HDLs) are the alterations that contribute the most to an increased risk of cardiovascular diseases and can be also present in combination. Moreover, in some cases, such alterations can be the consequence of genetic mutations or secondary to other pathological conditions or lifestyle. 2 In particular, the Framingham Study and Multiple Risk Factor Intervention Trial demonstrated that mortality from cardiovascular disease increases progressively with increasing levels of LDL cholesterol. 2
At present, the most common therapy used to reduce LDL cholesterol is statin. However, it is not always well tolerated. 5 Indeed, many patients are reportedly unable to reach LDL cholesterol target values because of their inability to tolerate statin or a full dose of the drug because of adverse effects. This intolerance could also be associated with polymorphisms of numerous genes. 6 Various side effects have been reported in association with statin therapy, including increased transaminase, increased risk of diabetes mellitus and in some cases, correlations with renal and neurological dysfunctions. 7 Moreover, other side effects have been observed such as dyspepsia, nausea, and headache, although clinical studies show that these symptoms also occur with the same incidence in patients treated with a placebo. 8 Furthermore, use of statins is contraindicated during pregnancy and breastfeeding because of general safety concerns, and the fact that several studies have suggested that statins are teratogenic and could accumulate in milk. 9 In addition, statin therapy has been reported not to achieve clinical results in 10–15% of patients. 10
At present, other treatments are available, including berberine. Berberine is extracted from several plants of the Berberidaceae family, namely Berberis aristata (tree turmeric), Berberis vulgaris (barberry), and Berberis aquifolium (the Oregon grape). It can also be found in plant species such as Argemone mexicana, Thalictrum flavum, Hydrastis canadensis (goldenseal), Coptis japonica, Coptis chinensis (Coptis or goldthread), and Phellodendron amurense. 11,12 Berberine is used in traditional Chinese and Indian medicine, thanks to its antimicrobial properties against various microorganisms, including bacteria, viruses, fungi, protozoa, and helminths. Hence, it is used in the treatment of diarrhea and intestinal infections. Recently, studies have highlighted new potential applications for berberine based on pharmacological mechanisms related to metabolism, in particular, in the treatment of hypercholesterolemia. 13
The mechanism of action of berberine is different from that of statins because it does not involve the activity of 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase. Indeed, berberine is able to upregulate the expression of the receptor for LDLs independently of sterol regulatory element-binding proteins (SREBPs). However, it is dependent on the activation of kinases regulated by extracellular signaling and by “c-Jun N-terminal kinase” (JNK). Specifically, the upmodulation of LDL is caused by a post-transcriptional mechanism capable of stabilizing the mRNA. 14 Furthermore, researchers have reported observing a synergistic interaction between berberine and simvastatin, which could be explained by the role of the proprotein convertase subtilisin/kexin type 9 (PCSK9). 5
Recently, it was discovered that PSCK9 binds to the LDL receptor on the cell surface determining the distribution of receptors from the surface to lysosomes, where they will be degraded, thus preventing the receptors from being recycled on the cell surface 15 and resulting in the removal of LDL cholesterol from circulation. 5
However, there could be other mechanisms related to the action of berberine. For example, berberine may be able to reduce levels of cholesterol by inhibiting its absorption and promoting its excretion. On a molecular level, this may be explained by a decreased capacity in molecular up-taking of cholesterol from the enterocyte and/or to an increased ability in releasing on the hepatic site. 5 The reduction of the cholesterol absorbing ability of enterocytes was confirmed by a study involving the coadministration of berberine and phytosterols, which was found to result in an important synergistic interaction leading to a reduction in the absorption of intestinal cholesterol. 16 An increase in the cholesterol released by the liver and subsequent increased cholesterol levels in bile were demonstrated by a study conducted on hyperlipidemic rats treated with berberine. 17
A crucial characteristic of berberine is related to its absorption and its consequent low bioavailability. Indeed, absorption is <1% in humans. 18 A number of different approaches are used to increase its bioavailability such as the coadministration of berberine with substances that can increase its absorption or the use of analogues or derivatives of berberine with the same pharmacological properties. 19 Regarding the coadministration of berberine with other substances, the validity of Silybum marianum extract (an inhibitor of P-19 glycoprotein) has been recognized. 19 S. marianum is a complex of flavoneolignans, mainly silybin, silidianin, and silicristina, which constitute silymarin. 20 In addition to silymarin, plant derivatives have been observed to antagonize P-glycoprotein, including ginsenosides, catechins gallate, and naringenin. However, silymarin is preferred because of its low oral availability, which allows it to carry out its actions almost completely at the intestinal level. 5
Several studies claim that berberine is able to reduce total cholesterol (TC) and LDL by 30% and 25%, respectively, and triacylglycerols by ∼35%. Such claims are based on both animal and human models. 14,21 Studies concerning the use of pure berberine, multicomponent mixtures containing berberine and formulations that enhance the activity are present in literature. In this regard, the main aim of this study was to investigate which of the various berberine-containing neutraceuticals are most effective in reducing TC and LDL cholesterol. Moreover, its impact on other variables, in particular HDL and triglycerides, was also assessed. Possible correlations between each parameter and the daily dose, age of the participants, and the duration of the treatment were also examined.
Meta-analyses of berberine have already been performed such as the study by Lan et al 22 in which clinical studies were selected from Chinese databases, and meta-analyses were conducted to study the effects of berberine on type 2 diabetes, hyperlipidemia, and hypertension and also examining the action of berberine when used with lipid-lowering drugs and alone. Another recent meta-analysis on the effects of berberine focused on berberine used in combination with silymarin in randomized, double-blind placebo-controlled clinical trials. 23
In this investigation, clinical studies in which berberine was administered without other treatment combinations were selected together with investigations in which different formulations containing berberine were compared to evaluate their efficacy in the treatment of dyslipidemia and their possible specific clinical use. Moreover, both controlled trial and cross-sectional trials were assessed. To the authors' knowledge, this is a novel approach, which could provide useful information for clinicians.
Materials and Methods
Search strategy
A meta-analysis was carried according to PRISMA guidelines. A systematic computerized literature search was performed using the online database MEDLINE®/PubMed.
A combination of keywords including “effect” AND “berberine,” “effect” AND “berberine” AND “dyslipidemia” were used.
Inclusion and exclusion criteria
Controlled trials and cross-sectional trials were considered. The studies that were selected were on the use of berberine alone, berberine in formulations with silymarin, or any mixtures containing berberine.
Moreover, the subjects under study had dyslipidemia, type 2 diabetes, polycystic ovary syndrome (PCOS), metabolic syndrome, hypercholesterolemia, and high-dose statin intolerance.
Only studies that reported specific blood parameters (TC, LDL, HDL, and triglycerides), which were evaluated both before and after the intervention, were selected. Studies conducted on animal models and those that did not meet all the inclusion criteria were excluded.
Data extraction and statistical analysis
The first search with “effect” and “berberine” as keywords led to the selection of 5545 articles. These were reduced to 598 by applying the keywords “effect” and “berberine” and “dyslipidemia.” Of these, 292 were clinical studies. Finally, applying the inclusion and exclusion criteria, 19 studies were considered for the meta-analysis.
Data extracted from each eligible study were analyzed and are summarized in Tables 1 (controlled trials) and 2 (cross-sectional trials). In particular, the number of subjects, their age, the daily dose of berberine, treatment durations, formulations used, and blood parameters (TC, LDL, HDL, and triglycerides) were reported. Data were analyzed using ProMeta 3 software© (2015; Internovi). Data related to selected blood parameters were expressed as mg/dL, in the case of mM, a conversion to mg/dL was performed to analyze the data using the software.
Controlled Studies Baseline Characteristics
Data reported as mean ± SD (except otherwise specified).
Values represented in median (range).
HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC, total cholesterol; TG, triglycerides; SD, standard deviation.
The meta-analysis was carried out using a fixed-effects model by obtaining the forest plot with effect size (ES) and confidence interval (CI) fixed at 95%. The significance of ES was calculated using the Cohen scale (1988; Cohen), in which 0.0–0.2 was considered a small effect close to zero, 0.2–0.5, a small effect, 0.5–0.7, a medium effect, and >0.8, a large effect. For each variable (TC, LDL, HDL, and triglycerides), forest plots were analyzed for the efficacy of berberine and different formulations. Statistical heterogeneity was evaluated using Higgins index (I 2 ), where 0–40% represents almost no heterogeneity, 30–60%, mild heterogeneity, 50–90%, considerable heterogeneity, and 75–100%, strong heterogeneity. When considerable or marked/strong heterogeneity was found, the age, daily dose, and duration of treatment variables were analyzed individually by meta-regression techniques, thus revealing how significant those variables were in response to treatment.
Results
The initial 5545 publications that were retrieved (Fig. 1) were reduced to 598 articles after applying the restriction concerning the association between berberine and dyslipidemia, and of those articles, only 292 were clinical studies. Among clinical studies, 220 were full-text articles, of which 201 were excluded because they did not meet the inclusion criteria, finally leaving 19 studies that were selected for the meta-analysis.

Prisma flow diagram.
Data from clinical trials included in the meta-analysis are given in Tables 1 and 2.
Cross-Sectional Studies Baseline Characteristics
Data reported are as mean ± SD (except otherwise specified).
Values are represented as median (range).
Of the 19 studies, 12 were controlled trials, whereas 7 were cross-sectional trials. The subjects of the studies ranged in age from 21 to 77 years, the daily dose of berberine ranged from 200 to 1500 mg, and the duration of treatment ranged from 30 to 365 days.
An important consideration was the type of formulation that was administered. Five studies regarded berberine taken alone, eight studies were concerned with a combination of berberine and silymarin, and six studies focused on mixtures containing berberine.
Regarding the subjects of the investigations, 3 studies involved women with PCOS, 6 involved patients with type 2 diabetes (in 2 of those studies, subjects were both diabetic and dyslipidemic), 11 studies involved dyslipidemic patients (2 of those studies involved patients with both dyslipidemia and diabetes) and 1 study examined patients with metabolic syndrome.
Effects on TC
Figure 2 provides the effect of berberine on TC with an ES of −1.17 (−1.28 to −1.06), which is of great significance according to the Cohen scale; therefore, regardless of the type of formulation, berberine was found to be effective in the reduction of TC.
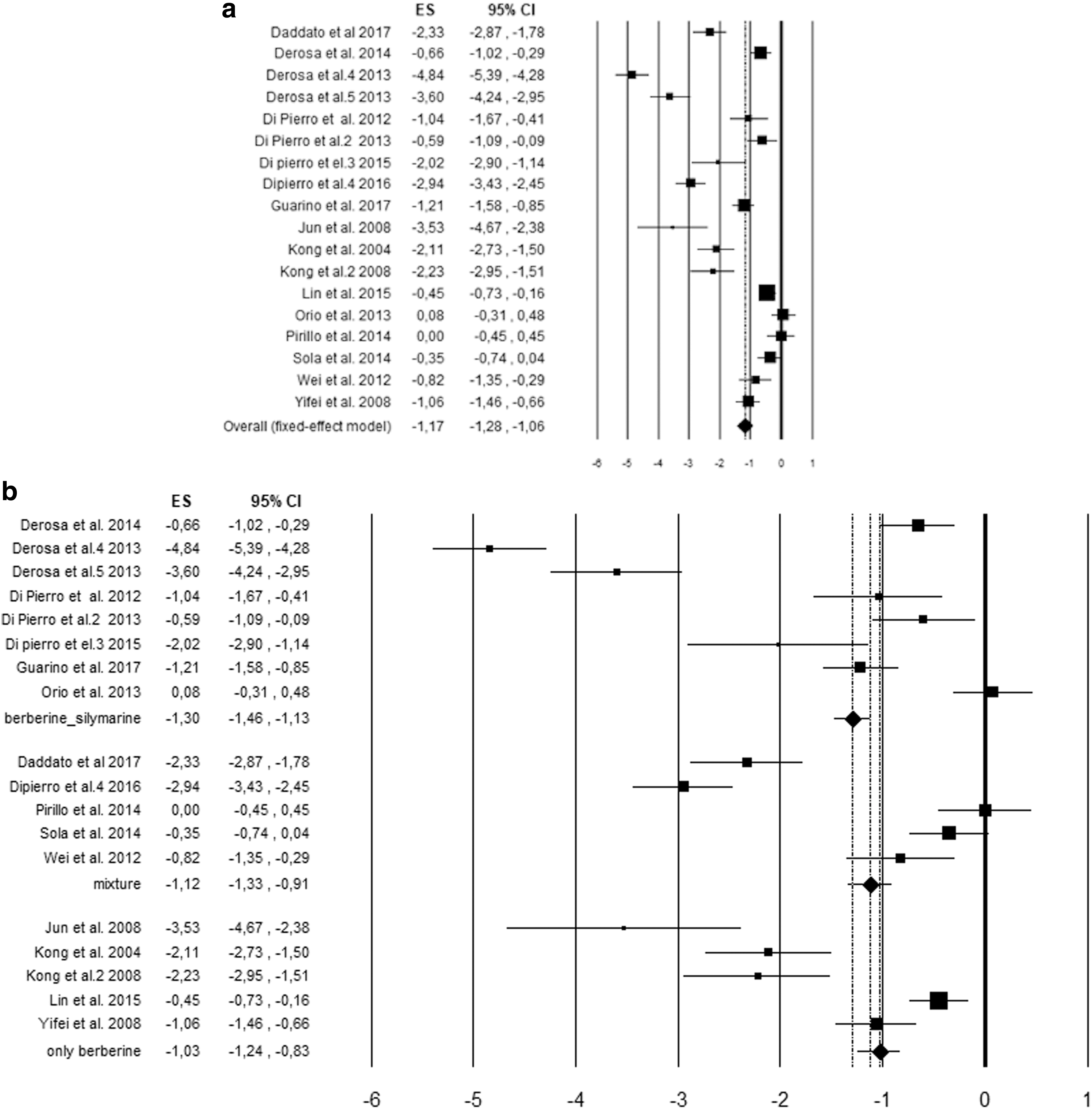
Effects of berberine on total cholesterol overall
None of the studies seem to be favorable to controls, but from the forest plot it can be noted that of the 19 analyzed studies, three do not reach the threshold of statistical significance: Orio et al. 24 with ES 0.08 (−0.31 to −0.48), Pirillo et al. 38 with ES 0.00 (−0.45 to 0.45), and Solà et al. 40 with ES −0.35 (−0.74 to 0.04).
In particular, the 2013 study by Orio et al. 24 was conducted on obese women with PCOS, that of Pirillo et al., 38 on patients with metabolic syndrome, and that of Solà et al. 40 on patients with moderate hypercholesterolemia.
Significance was found in particularly in two studies: De Rosa et al. 29,31 with ES values of −4.84 (−5.39 to −4.28) and −3.60 (−4.24 to −2.95), respectively.
The subjects in these studies were male and female, Caucasian, dyslipidemic patients, older than 18 years. In particular, in the first study, the age ranged from 21 to 27 years, whereas in the second study, it ranged from 50 to 60 years. In both studies the daily dose was 1176 mg of berberine associated with silymarin for a duration of 90 days. Concerning formulation types, it was found that berberine taken alone has an ES of −1.03, which is of great effect according to the Cohen scale, berberine associated with silymarin had an ES of −1.30, also of great effect, whereas the mixtures showed an ES of −1.12, representing a great effect compared with overall ES values. Overall ES values showed that the formulations were effective, regardless of their type. However, berberine associated with silymarin showed a value higher than the other two formulation types; hence, we can deduce that it has a more significant effect.
Considerable statistical heterogeneity was found (I 2 = 96%). Using meta-regression, age, daily dose, and duration of treatment variables were analyzed individually to study their correlation with the efficacy of the treatment. Age-related meta-regression showed that the effects of berberine on TC were not significant (P = .15).
Regarding the daily dose, a value of P = .58 was reported, which was not significant either. As regards the duration of the treatment, a nonsignificant value of 0.69 was obtained. Therefore, neither the age, nor the daily dose, nor the duration of treatment was able to account for the variability of the results of the studies.
Effects on LDL cholesterol
The effect of berberine on LDL cholesterol is given in Figure 3. All the clinical trials showed favorable results for the experimental group. Of the 19 studies, 3 were not significant: Di Pierro et al. 25 with ES −0.59 (−1.19 to 0.02), Orio et al. 24 with ES −0.33 (−0.72 to 0.07), and Solà et al. 40 with ES −0.31 (−0.70 to 0.08).
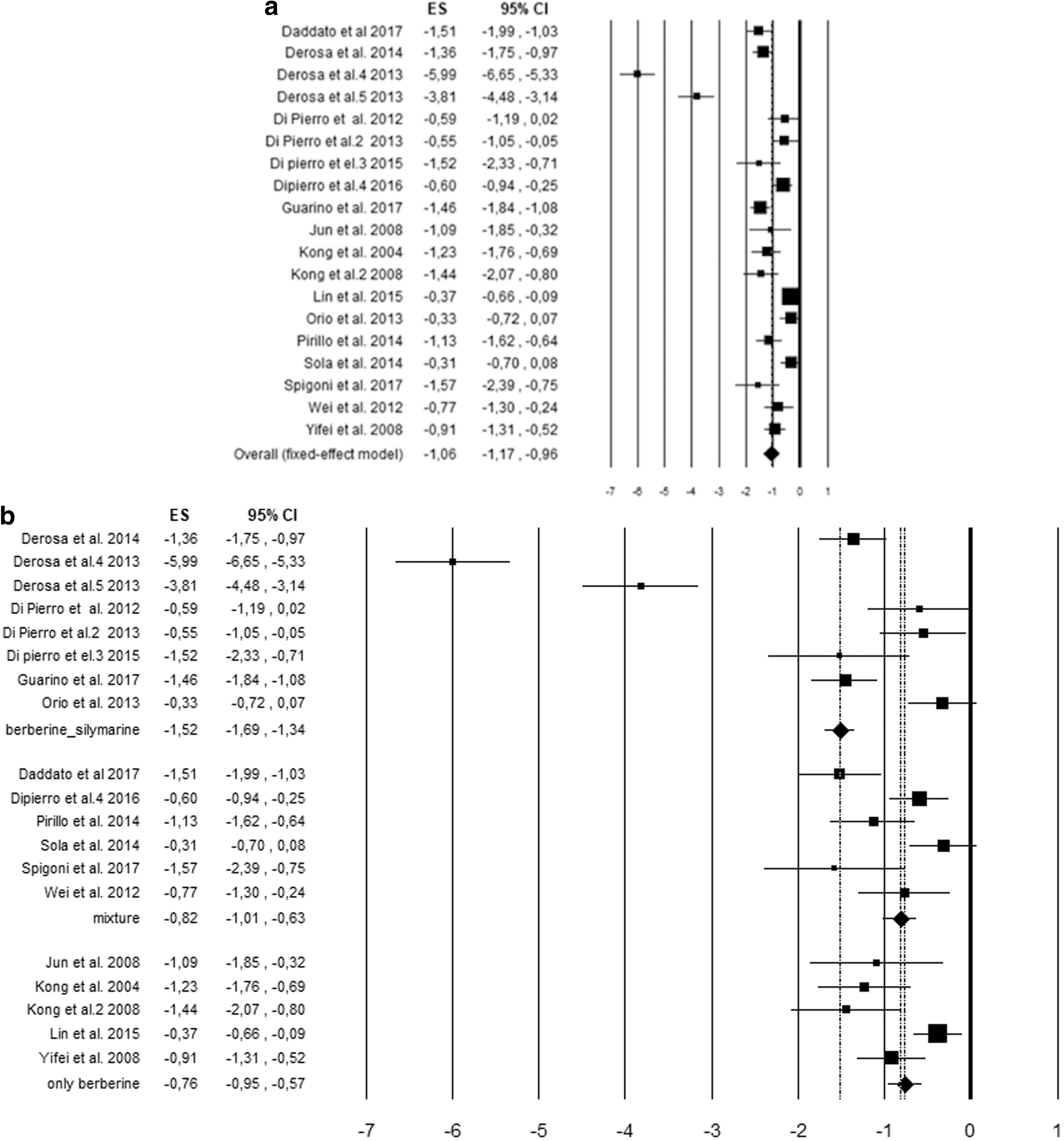
Effects of berberine on low-density lipoprotein cholesterol; overall
Di Pierro et al. 25 carried out their study on 22 subjects with type 2 diabetes. The small sample size could account for the nonsignificance; the study by Orio et al. 24 was conducted on obese women with PCOS; Solà et al. 40 investigated patients with moderate hypercholesterolemia.
The studies by De Rosa et al. 29,31 were of particular interest showing an ES of −4.84 (−5.39 to −4.28) and −3.60 (−4.24 to −2.95), respectively. These studies were conducted on male and female, Caucasian, dyslipidemic patients older than 18 years. In particular, in the first study the subjects ranged in age from 21 to 27 years, whereas in the second study, they ranged from 50 to 60 years. In both studies the daily dose was 1176 mg of berberine associated with silymarin administered for 90 days.
Evaluating the overall results, the ES value was found to be −1.06 (−1.17 to −0.96), which shows great effect according to the Cohen scale. Therefore, berberine is effective in the reduction of LDL.
Comparing the three overall ES values in relation to formulation type, the formulation of berberine with silymarin had a value of −1.52, which corresponded to a great effect according to the Cohen scale. Mixtures had a value of −0.82, corresponding to a great effect, whereas berberine taken alone had a value of −0.76, which corresponded to a moderate effect.
These values show the effectiveness of berberine, regardless of the type of formulation. However, berberine associated with silymarin had a value that was greater than the other two typologies suggesting that it had a more significant effect.
With respect to statistical heterogeneity, the software yielded a result of I 2 = 95%, which showed considerable heterogeneity. Age, daily dose, and duration variables were examined by meta-regression analyses to evaluate correlations with the efficacy of the treatment.
The effects of berberine on LDL in relation to age were found not to be significant (value of significance = 0.18). Regarding the daily dose, the software yielded a value of P = .48, which was not significant. As regards the duration of the treatment it showed P = .45.
Effects on HDL
With respect to the effect of berberine on HDL, an ES value of 0.24 (0.14–0.34) was reported, which corresponded to slight but insignificant increase in HDL (Fig. 4).

Effects of berberine on high-density lipoprotein; overall
Of 19 studies, 10 were in favor of controls, of which 5 were significant. Of these, three were of great significance: Guarino et al., 30 Pirillo et al., 38 and Wei et al. 32 with ES values of 1.70 (1.31–2.09), 1.12 (0.63–1.60), and 1.10 (0.55–1.65), respectively, indicating great effect according to the Cohen scale.
The investigation by Guarino et al. 30 was conducted on subjects with type 2 diabetes ranging in age from 55 to 65 years. Subjects took a daily dose of 1000 mg for 365 days. The study by Pirillo et al. 38 focused on subjects with metabolic syndrome ranging in age from 53 to 60 years. They took a daily dose of 400 mg for 56 days. Wei et al. 32 focused on PCOS patients, age 25–28 years, who took a daily dose of 1500 mg for 90 days.
One study was found to be exactly on the significance line, whereas the other eight studies were in favor of the experimental groups but only one study by Jun et al. 35 was found to be statistically significant with an ES of −1.44 but a wide CI (−2.25 to −0.64), possibly because of the small sample size (n = 15).
Regarding ES in terms of formulation typology, berberine alone showed a value of −0.19 (−0.38 to −0.00), corresponding to a small effect. In a formulation with silymarin, the ES was 0.46 (0.30–0.61), corresponding to a moderate effect. A small effect was found for berberine mixtures, which showed an ES of 0.34 (0.16–0.52).
Taken together these data suggest that berberine taken alone seemed to have no effect on HDL, whereas berberine taken with silymarin and mixtures of berberine had a small effect on HDL, which showed a slight but statistically insignificant increase.
Heterogeneity was found to be consistent (I 2 = 85%). Age, daily dose, and duration variables were investigated by meta-regression analyses to evaluate correlations with the efficacy of the treatment. No significance was found for age (value of 0.49), daily dose (value of 0.95), or treatment duration (value of 0.33).
In conclusion, age, daily dose, and treatment duration did not correlate with the effect of berberine on HDL.
Effects on triglycerides
The effect of berberine on triglycerides resulted in an overall ES of −0.60 (−0.71 to −0.50), which corresponded to a moderate effect according to the Cohen scale (Fig. 5). Of 19 studies, only 1 was in favor of controls, 36 whereas of the other 18 (favor experiment), 12 were statistically significant.

Effects of berberine on triglycerides; overall
Di Pierro et al. 36 reported an ES of 0.40 (0.05–0.74). Their investigation involved overweight/obese and hypercholesterolemic subjects ranging in age from 51 to 65 years and taking a daily dose of 500 mg for 180 days of treatment.
Among the 12 significant studies (favor experimental), 3 were of particular interest: Guarino et al., 30 Jun et al., 35 and Pirillo et al. 38 with ES = −2.64 (−3.10 to −2.18), −2.54 (−3.51 to −1.58), and −1.87 (−2.42 to −1.33), respectively.
The study by Guarino et al. 30 was conducted on type 2 diabetic subjects with altered lipid profiles ranging in age from 55 to 65 years and taking a daily dose of 1000 mg for 365 days of treatment.
The study by Jun et al. 35 was considered to have low statistical power because it was conducted on a small sample size (n = 15) with type 2 diabetes. Pirillo et al. 38 focused on subjects with metabolic syndrome ranging in age from 53 to 60 years and taking a daily dose of 400 mg for 56 days of treatment.
With respect to formulation typology, the overall ES of berberine taken alone was −0.56 (−0.76 to −0.36), representing a mild effect.
On the contrary, berberine and silymarin taken in combination yielded an ES of −0.84 (−1.01 to −0.68), representing a great effect, whereas mixtures yielded an ES of −0.31 (−0.50 to −0.13), representing a small effect.
Thus, berberine associated with silymarin had an ES value that was higher than the other formulations.
Age, daily dose, and duration of treatment were evaluated using a meta-regression analysis because considerable heterogeneity (I 2 = 89%) was obtained.
For age and daily dose, values of 0.62 and 0.44, respectively, were obtained; therefore these variables did show a significant correlation with treatment efficacy. On the contrary, treatment duration was observed to be quasi-significant (value of 0.06), suggesting that the duration of treatment may influence the reduction of triglycerides (Fig. 6).
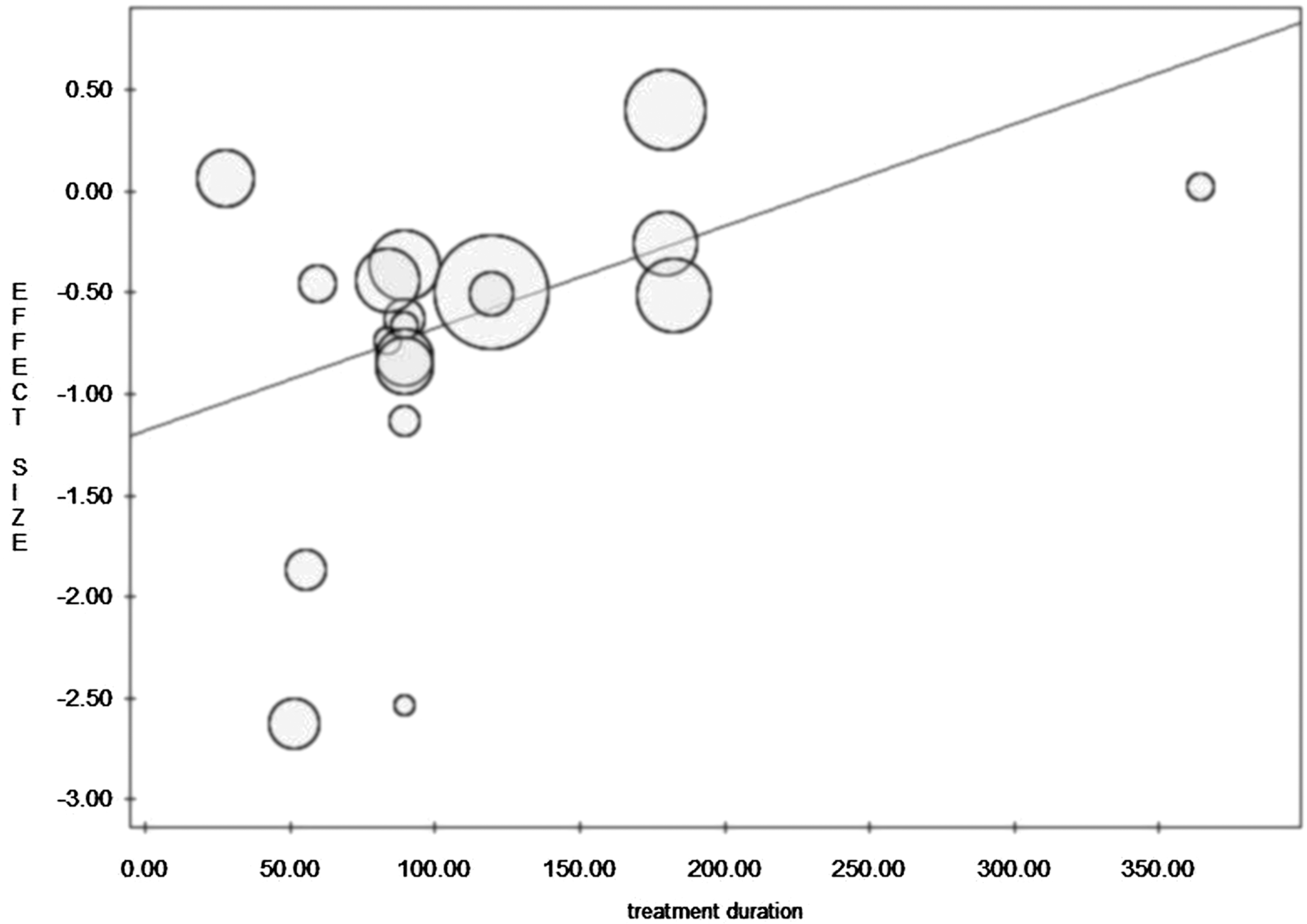
Meta-regression. Effects of berberine on triglycerides according to treatment duration.
Discussion
This meta-analysis shows that berberine is effective in reducing TC, LDL cholesterol, and triglycerides and may result in a slight increase in HDL cholesterol.
Regarding formulations, berberine associated with silymarin was found to be particularly effective in reducing TC and LDL cholesterol in dyslipidemic subjects of any age and triglycerides in diabetic subjects with altered lipid profiles.
Indeed, as far as the type of formulation is concerned, the main point of interest of this study, it can be said that the formulation of berberine with silymarin is of particular interest because of its significant impact on TC, LDL cholesterol, and triglycerides. The effectiveness of this formulation may be because of the ability of silymarin to increase the bioavailability of berberine.
However, in the other two cases (berberine alone and other mixtures), efficacy was also shown in terms of LDL and triglyceride reduction, although their impact was smaller than that which was obtained with berberine and silymarin.
With respect to HDL, the formulation of berberine and silymarin was the most effective of the three formulations considered, although it only yielded a moderate effect.
With regard to age, daily dose, and duration of treatment for all the variables considered (TC, LDL, HDL, and triglycerides), no significant effects were found, with the exception of the slight impact of the duration of treatment on triglycerides.
Wide ranges were found for age, dose, and duration of treatment. Indeed, age ranged from 17 to 77 years, daily dose from 200 to 1500 mg, and the duration of treatment from 30 to 365 days.
Statistical heterogeneity was considerable and may be because of either methodological heterogeneity or clinical heterogeneity or both.
Hence, more specific clinical studies with even more restrictive inclusion criteria are necessary to better define the efficacy of berberine and its formulations and the type of patient that best responds to such treatments.
Footnotes
Author Disclosure Statement
A.B. has affiliations with organizations with indirect financial interest in the subject matter discussed in the article. No competing financial interests exist for the other authors.
Funding Information
No funding was received for this article.