
Abstract
Inadequate dietary fiber intake contributes to irregular bowel movements and may contribute to difficulty with defecation in children. Whole grain foods, such as oatmeal, may improve stool consistency and stool frequency in children; however, no studies have examined its effects. The purpose of this study was to investigate if 2 weeks of oatmeal consumption in children (ages 7–12 years) increases stool frequency, improves stool consistency, and gastrointestinal (GI) symptoms. In this single-arm intervention study, children who reported ≤5 bowel movements per week during screening, consumed two servings of instant oatmeal daily for 2 weeks. The primary outcome was stool frequency and secondary outcomes included stool consistency and GI symptoms. Participants recorded bowel movements daily, food intake, and GI symptoms during baseline and 2 intervention weeks. Photos of the children's stool were taken at three timepoints during the study to assess stool consistency. In total, 33 children (15 female and 18 male) completed the study. Linear mixed models were used to detect change between baseline and the intervention weeks and accounted for repeated measures within subjects. No statistical differences in stool frequency or consistency were observed between the intervention weeks vs. baseline; however, dietary fiber intake significantly increased during the 2 weeks of oatmeal consumption (P = .008). The addition of oatmeal to children's diets is an effective way to increase fiber consumption and may reduce some GI symptoms such as gas, straining, and feeling of incomplete evacuation. Trial identification number: NCT02868515.
Introduction
Dietary fiber helps to increase the frequency of bowel movements and may help to alleviate some common childhood gastrointestinal (GI) disorders. 1 Despite the benefits of fiber for GI health, few children consume the recommended amount of total fiber daily. Children 4–8 years, for example, require 25 g of fiber daily, with older children (9 years +) requiring ≥26 g of fiber daily, depending on age. 2 Data from NHANES 2013–2014 found children at ages 6–11 years consume 14–15 g of fiber daily; nearly half of the recommended amount. 3 Because fiber supports normal laxation, children who continually fall short on fiber in their diet maybe susceptible to GI problems, such as difficulty with defecation.
A recent review examined the effects of fiber-containing foods or supplements on outcomes of GI health in children and found that soluble fibers such as partially hydrolyzed guar gum and glucomannan improved stool frequency and stool consistency. 4 The effects of other soluble fiber sources on stool frequency, stool consistency, and GI symptoms are not well studied in children; therefore, it is difficult to determine which dietary fibers are the most effective for common GI problems. Collectively, there is an urgent need for more research in children to better understand which sources of dietary fiber improve common childhood digestive health problems.
Oatmeal is a whole grain food that is high in the soluble fiber, beta-glucan. 5 Soluble fibers allow stool to absorb water and improve consistency, leading to a stool that is neither too hard nor too soft. The consumption of soluble fiber in the diets of children may therefore help improve common GI problems that children experience, such as difficulty with defecation. Difficulty with defecation is a GI problem that is not well defined in the scientific or medical community. Other GI problems, such as constipation, have clinical diagnostic criteria, whereas difficulty with defecation is thought to trouble a large percentage of children in the United States who do not meet the criteria for constipation. Therefore, the purpose of our pilot study was to examine if 2 weeks of daily oatmeal consumption improved stool frequency, consistency, and GI symptoms in children who report irregular stool production.
Materials and Methods
A total of 40 children were recruited for this study to achieve 80% power to identify a mean change of 0.65 standard deviation (SD) in defecation frequency; however, only 33 children (18 male and 15 female), completed the study. Thirty-three participants gave us 80% power to detect a mean change of 0.72 SD. Participants were recruited by flyers posted around the University of Minnesota campus including student housing and campus daycares. Recruitment e-mails were also sent to Minneapolis neighborhood groups. To determine eligibility, participants completed an online screening questionnaire. Children were included if they were 7–12 years of age, reported ≤5 stools a week, and if they were low-fiber consumers, defined as fewer than 14 g/day. Children were excluded if they used laxatives, were on antibiotics in the last month, used fiber supplements, or were not habitual breakfast eaters. The recruitment methods and study design was approved by the University of Minnesota International Review Board (IRB approval 1604S86583). Written informed consent was obtained from all the participants and their parents or guardians. The participants additionally signed assent forms confirming they could leave the study at any time without consequence.
The oatmeal packages each contained 1.5 ounces of dry, instant oatmeal and came in Maple Brown Sugar and Cinnamon Spice flavors. Each package contained 3 g of fiber. Participants were instructed to prepare the oatmeal with either water or milk of any type in the microwave. Participants could include additives such as honey, sugar, maple sugar, and spices; however, they were instructed not to add fiber supplements or foods high in fiber such as fruit, or other grains. A list of allowed and prohibited additives was provided to participants. Additive use was additionally recorded in a food diary. To ensure compliance, participants were instructed to return empty oatmeal packets to the research staff. If subjects had difficulty finishing an oatmeal serving, they were instructed to document the actual amount consumed in the food diary.
Subjects, with their parents' help, kept bowel movement diaries where they recorded the date and time of each bowel movement during the baseline week and the subsequent 14 days of oatmeal intervention. Physical activity diaries with the type of exercise and the time in minutes of the activity were recorded as well. Food diaries were kept at two points during the study where participants recorded everything they ate and drank for 3-day periods. Subjects were instructed to estimate portions using measurements like cups, tablespoons, teaspoons, a. Participants were additionally provided a Nutritional Data System for Research (NDSR) food portion visual poster to help estimate food consumed. The food diaries were analyzed for total calories, carbohydrate, fat, protein, and fiber consumed using NDSR 2014 software. To assess GI symptoms, children filled out two validated questionnaires, the Child Regularity Questionnaires and the GI Tolerance Questionnaire. 6,7 Participants or their parents were also required to take photographs of the participant's stool on 3 days of the study. The stool was to be photographed in the toilet with no tissue paper obstructing the view. Most parents used a cellphone camera and were instructed to avoid blurry photograph. The photos were e-mailed to the study staff and were assigned a Bristol stool score depending on the consistency of the stool. For consistency, the same staff member was responsible for assigning Bristol stool scores.
Subjects attended a prestudy visit at the University of Minnesota along with a parent or guardian to review the study protocol, sign assent and consent forms, and to receive instructions on oatmeal preparation and taking stool photographs. The questionnaires, diaries, and oatmeal packets were dispensed at this time. During the first week of the study, days 1–7, subjects consumed their normal diet with no oatmeal and baseline measurements were recorded. The measurements included filling out the bowel movement and physical activity diaries. On days 5–7, the food diary recorded the child's diet each day. Finally, on day 7 participants filled out the GI Tolerance Questionnaire and the Child Regularity Questionnaire and the first stool picture was taken, although we accepted any stool photos taken during this week if a bowel movement did not happen on day 7.
Days 8–13 were a washout period where no information was recorded. Day 14 started the 2 weeks of oatmeal consumption. Two packets of oatmeal were consumed each day. For the entire 2-week period, days 14–27, a bowel movement diary and physical activity diary were recorded. At the end of the first week of oatmeal consumption, day 20, the GI Tolerance Questionnaire, Child Regularity Questionnaire, and stool photograph were completed. As with day 7, a stool photo from another day that week was also acceptable. A food diary was completed for the last 3 days of the oatmeal intervention, days 25–27. Also on the final day of oatmeal consumption, day 27, the GI Tolerance Questionnaire, Child Regularity Questionnaire, and the third stool photo were completed.
Participants were provided with a calendar and checklist that listed all the questionnaires and diaries and when each had to be completed. Participant's parents were also sent e-mails as an additional reminder every day paperwork or a photo was due. Once the study was completed, participants returned to the University of Minnesota to drop off the questionnaires, diaries, and empty or unused oatmeal packets. Stool photos were e-mailed to the study staff and the staff assigned a score from the Bristol stool scale to each photo based on stool consistency. The food diaries were analyzed using NDSR software.
Descriptive statistics were calculated and presented using mean values and SDs for continuous outcomes and frequencies and percentages for categorical outcomes. Linear mixed models were used to evaluate change from baseline to week 1 and 2. Models included a fixed effect of time and a random intercept to account for repeated measures within subject. Models were conducted for male and female children combined, and also separately by male and female children.
Analysis was performed using Statistical Analysis Software (version 9.3; SAS Institute, Inc., Cary, NC, USA). A two-sided P < .05 was considered statistically significant.
Results
Stool frequency and consistency
The average number of bowel movements recorded in the bowel movement diaries for the baseline week, week 1, and week 2 were 5.6 ± 2.7, 5.4 ± 2.6, and 5.2 ± 2.1, respectively (Table 1). No statistical differences were observed for stool frequency when comparing baseline with week 1, baseline with week 2, and between weeks 1 and 2 (P = .58, P = .24, and P = .52, respectively). When a subgroup analysis by gender was performed, there were still no differences in stool frequency between each week. The average stool consistency scores according to the Bristol stool scale for each photograph on days 7, 20, and 27 were 3.9 ± 1.3, 3.8 ± 1.3, and 4.1 ± 1.4, respectively (Table 2). No significant differences were seen in the Bristol stool score between the three photographs from days 7 to 20, days 7 to 27, or days 20 to 27 (P = .85, P = .62, and P = .50, respectively). Again, when analysis of stool consistency was separated by gender, the differences were not statistically significant.
Number of Bowel Movements Recorded in Bowel Movement Diaries by 33 Children Who Experience Difficulty with Defecation
Bristol Stool Consistency Scores from Stool Photographs Sent in Before and During Oatmeal Consumption by 33 Children Who Experience Difficulty with Defecation
Child Regularity Questionnaire
The mean responses from the Child Regularity Questionnaire are included in Table 3. For all participants, significant decreases were seen in self-reported scores of straining and gas from baseline compared with week 1 of oatmeal consumption (P = .05 and P = .04, respectively). A significant decrease in reports of incomplete evacuations of bowel movements was seen in the second week of oatmeal consumption compared with the baseline (P = .01). Self-reported stool frequency was significantly increased from baseline to both weeks 1 and 2 of oatmeal consumption (P = .02 and P = .007, respectively). No significant differences were seen in any symptoms when comparing weeks 1 and 2 of oatmeal consumption. Table 3 also provides the average responses from the Child Regularity Questionnaire separated by female and male children. When female children were analyzed separately, significant differences were seen only in flatulence symptoms between the baseline week and both weeks 1 and 2 of oatmeal consumption (P = .02 and P = .04, respectively). In male children, significant differences were seen between baseline and week 2 for both complete evacuation of stool and ratings of abdominal discomfort (P = .03 and P = .04, respectively). Self-reports of stool frequency were also significantly greater from baseline to weeks 1 and 2 of oatmeal consumption (P = .003 and P = .02, respectively). In both male and female children, no significant differences were seen between weeks 1 and 2 of oatmeal consumption.
Summary of Results from the Child Regularity Questionnaire Completed by 15 Female and 18 Male Children, Before and During Oatmeal Consumption
Significant P-values and symptoms are given in bold. The first six responses were ranked on a scale of 1 to 5. “Bristol scale” was a list of options 1 to 8. “Never missed school or activities” is listed in the table not as an average of the ratings reported but as number of participants who reported no school or activities missed during the study. “Stool size” was on a scale of 1 to 4.
GI Tolerance Questionnaire
The responses from the GI Tolerance Questionnaire are displayed in Figure 1. No significant differences were seen in the number of participants reporting any of the GI symptoms when comparing the baseline week, week 1 of oatmeal, and week 2 of oatmeal. In addition, no significant differences were observed in the total number of GI symptoms participants reported between each week. When analysis was split between male and female children, no significant differences were observed in the number of GI symptoms.
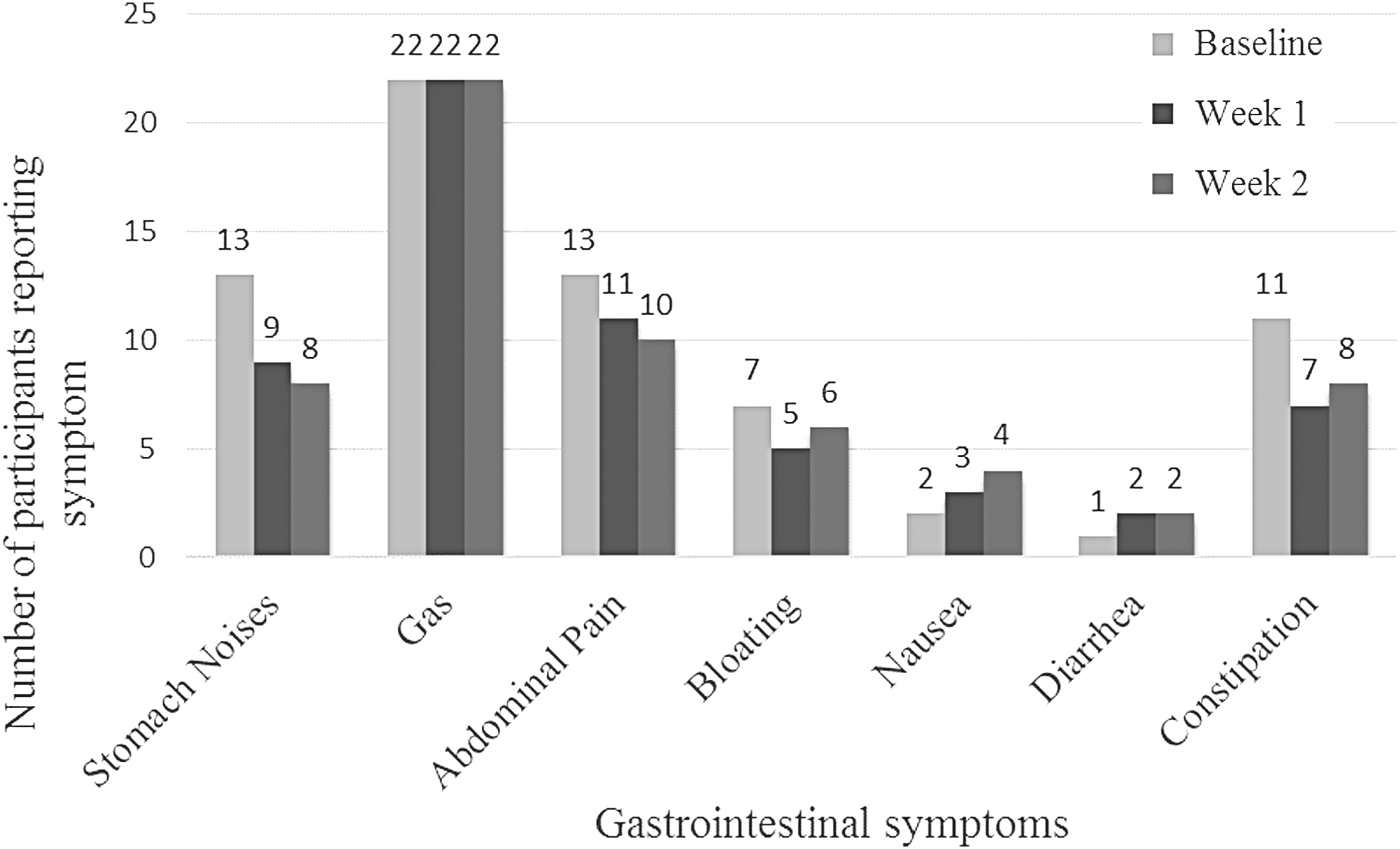
Gastrointestinal Tolerance Questionnaire responses.
Food diaries
The average intakes of calories, carbohydrate, fat, protein, and fiber from the food diaries are given in Table 4. Overall, an increase in total grams of carbohydrates and fiber consumed was observed between the baseline food diaries, days 5–7, and the food diaries collected during the oatmeal intervention, days 25–27 (P = .0008 and P = .008, respectively). In male children, differences were also seen in total carbohydrates and fiber intake (P = .0014 and P = .005) and an increase in total calories (P = .04) between the first food diary and the second. When female children were analyzed separately, no differences were seen in any nutrient from the pre-oatmeal food diary to the oatmeal intervention diary.
Nutrient Intake Data Reported in Food Diaries Before and During Oatmeal Consumption in Children Who Experience Difficulty with Defecation
Significant P-values are given in bold.
Discussion
In children who experience difficulty with defecation, we did not observe a change in stool frequency or stool consistency with 2 weeks of oatmeal consumption. Several factors in our study may have impacted these results and we acknowledge several limitations with recruitment and execution of this pilot study. To our knowledge, there is no standardized amount of oatmeal that has been scientifically shown to help children who experience difficulties with defecation. Perhaps a greater amount of oatmeal per day would have resulted in greater changes in stool frequency and stool consistency.
We attempted to enroll children by our screening tool who reported ≤5 bowel movements per week. We also measured stool frequency during the baseline of our study and found that the mean stool frequency was 5.6 stools per week, rather than <5 as was reported during screening. The subjects then consumed the oatmeal treatment and stool frequency did not significantly increase.
One of the strengths of this pilot study is that we did observe a significant increase in fiber intake during the 2 weeks of oatmeal consumption compared with the baseline week. This suggests that a whole grain food, such as oatmeal, may be a vehicle to introduce more fiber into the diets of children and one way to help fill the fiber gap.
A promising result from the Child Regularity Questionnaire is that self-reports of gas frequency decreased significantly after a week of oatmeal consumption compared with baseline. We hypothesize that one fear associated with increased intake of fiber is unwanted GI responses such as flatulence. However, our results suggest that gas occurrence does not increase with oatmeal intake, but actually decreases. There were also decreases in reports of straining during defecation and decreases in incomplete evacuations of stool during a bowel movement. This suggests that consumption of oatmeal may offer some relief from difficulty with defecation.
Furthermore, children reported in the Child Regularity Questionnaire a significantly higher stool frequency after oatmeal consumption compared with baseline; however, this increase in stool frequency was not reflected in the bowel movement diaries. Children believed they were defecating more after oatmeal treatment; however, according to their diaries, stool frequency was not significantly increased. It seems that children believed they had more bowel movements during oatmeal consumption even when stool frequency did not increase. It is also possible that the oatmeal intervention created a placebo effect that made children think they were defecating more often, even when that was not the case.
Finally, it is also interesting to note the differences in responses to the Child Regularity Questionnaire between male and female children. The only significant change in symptoms in female children was decrease in reported gas. Male children reported no significant difference in gas, but in stool frequency, abdominal pain, and straining.
A systematic review and meta-analysis of the use of fiber in childhood constipation treatment found no statistical significance for bowel movement frequency, stool consistency, therapeutic success, fecal incontinence, and abdominal pain with fiber intake in patients with childhood constipation. 8 They note that these results should be interpreted with care, because of the high clinical heterogeneity between the studies and the methodological limitation of the articles on the topic. Although the scientific literature does not provide evidence-based support for fiber supplements for children with constipation, children do not get the recommended amounts of dietary fiber from whole foods. Public health messaging, along with nutrition education for health care practitioners, parents, and children, is needed to increase the consumption of fiber-rich foods for the benefit of children who may suffer from common GI problems.
A shift to more plant-based diets including whole grains, legumes, vegetables, nuts, and fruits should help in prevention of digestive health problems in children. But many factors affect laxation beyond diet and dietary fiber. Exercise, drugs, stress, change in schedule, and regular habits are all known to alter gut health and be related to irregular stool output. 9 Designing a food intervention study to improve stool output or stool consistency in children is a challenge and it is likely that the amount of high fiber foods that children are willing to eat for a research study will limit the ability of seeing significant improvement in gut health measures.
In conclusion, overall, although we did not observe changes in stool frequency or stool consistency, we observed increases in fiber intake and reduction in some GI symptoms. Our research suggests that two packets of instant oatmeal per day effectively increases fiber intake in children who are low-fiber consumers. The changes in self-reported symptoms like gas, incomplete evacuation, and straining, suggest that some GI symptoms may be improved by regular oatmeal consumption.
Whole food interventions in children are challenging as consumption of the same food daily for days and days is a large participant burden. The wide variability in response to high fiber foods among subjects may also require a larger sample size than is practical in most settings. Isolated fibers may be a more likely solution to the low fiber intake problem seen in the pediatric population. Public health policies to increase consumption of plant-based foods high in dietary fiber are also welcome to improve gut health in children.
Footnotes
Acknowledgments
The authors appreciate the hard work and dedication of our subjects and their parents to participate in this study.
Authors' Contributions
H.P. was the study coordinator. She recruited subjects, managed the day-to-day aspects of the study, collected the data, and wrote the first draft of the article. R.K. wrote the study protocol, participated in the conduct of the study, and reviewed and commented on subsequent drafts of the article. Q.W. designed the statistical plan for the study, assisted in data analysis and wrote the statistical analysis section of the article. J.S. was the Principal Investigator for the grant, supervised all aspects of the study, and reviewed and commented on all drafts of the article.
Author Disclosure Statement
This study was initially enabled through funding provided by PepsiCo, Inc. PepsiCo subsequently withdrew its sponsorship because of discrepancies in the study protocols and execution. Although PepsiCo did not prevent publication, it has asked that the authors include this disclaimer noting that the study and views expressed herein are solely the authors and do not reflect the position or policy of PepsiCo, Inc.
Funding Information
Financial support from PepsiCo Global R&D.