
Abstract
The guidelines for the treatment of dyslipidemias include the use of nutraceuticals (NUTs) in association with lifestyle modifications to achieve therapeutic goals. In NUT pill, different substances may be associated; in this study we investigated a combined NUT containing monacolin K (MonK)+KA (1:1), berberine (BBR), and silymarin. The aim of the study was to evaluate low-density lipoprotein cholesterol (LDL-C) reduction in 53 patients suffering from polygenic hypercholesterolemia, characterized by a low/intermediate cardiovascular risk calculated with SCORE algorithm. The effects on lipid profile of 2-month treatment with NUT containing MonK+KA (1:1), BBR, and sylimarin, were compared with Atorvastatin (ATO) 10 mg administrated in a matched control group. Serum proprotein convertase subtilisin/kexin type 9 (PCSK9) levels and the cholesterol loading capacity (CLC) were determined at baseline and at the end of the study in NUT-treated group; variations were assessed. NUT was effective as lipid-lowering agent with a wide interindividual response variability (mean LDL-C from 170.8 ± 19.9 to 123.8 ± 20.0 with a change of −47.0 ± 21.5 mg/dL; P < .001) and the effect was similar to that induced by ATO. The use of NUT significantly modified PCSK9 levels (P < .01) and CLC (P < .001), ultimately suppressing the serum-mediated foam cell generation directly measured on human macrophages. NUT reduces LDL-C levels with an effect similar to what is induced by 10 mg of ATO and ex vivo improves the functional profile of lipoproteins with antiatherogenic action.
Introduction
Hypercholesterolemia is a major cardiovascular (CV) risk factor 1,2 as low-density lipoprotein cholesterol (LDL-C) is directly involved in the atherosclerotic process. 3 Especially foam macrophage generation is the final common pathway of different pathological mechanisms within atherosclerotic plaque. 4 Cholesterol loading capacity (CLC) is a validated method able to assay serum-induced influx of free cholesterol and lipoprotein 5 as well as cholesterol efflux in circulating human macrophages. 6 Increased CLC is a hallmark of foam cell generation thus representing a cellular proatherogenic index. Accordingly, a significant association between CLC and CV risk has been previously reported. 7,8 Proprotein convertase subtilisin/kexin type 9 (PCSK9) has recently attracted interest as negative regulator of hepatic expression of LDL-receptor (LDL-R) reducing LDL-R recycling. Through this mechanism, PCSK9 activity determines an increase in circulating LDL-C. 9,10
Hypercholesterolemia may be counteracted by the inhibitors of HMGCoA-reductase, also referred to as statins, 11 and in patients with low CV risk also nutraceutical (NUT) supplements may act as lipid-lowering agents. These natural compounds exert beneficial effects on lipid profile, by targeting total cholesterol (TC) and LDL-C. NUTs express their lipid-lowering effect through multiple mechanisms 12 and their safety was previously reported. 13 Among them, monacolin K (MonK), a molecule derived from fermented Monascus purpureus, shows the same chemical structure than lovastatin as well as the inhibitory activity on the enzyme HMGCoA-reductase. 14 Commonly used as reference in red yeast extract, MonK has been tested in randomized clinical trials, resulting in a reduced risk of coronary heart disease, stroke, and death for any cause. 15 Similarly, berberine (BBR), from Berberis aristata, shows a lipid-lowering activity due to LDL-R upregulation. 16 Although the activity of the P-glycoprotein (P-gp) might reduce the intestinal absorption of BBR, 17 but P-gp inhibitors, such as silymarin, may be coadministered to restore an adequate bioavailability. 18,19
Berberol®K has been then developed to combine the lipid-lowering activity of those different compounds and potentially obtain a synergistic effect. This pilot interventional clinical trial aims at investigating the effects of BerberolK on lipid profile in comparison with low-dose Atorvastatin (ATO) therapy in a cohort of dyslipidemic patients at a low/intermediate CV risk. The effect of BerberolK on lipid metabolism and PCSK9 levels was also investigated ex vivo through CLC.
Patients and Methods
Study design
The present study is a pilot single-center clinical trial in the context of the common clinical practice designed to test the efficacy of a lipid-lowering NUT, BerberolK, containing 10% MonK+KA (1:1), 500 mg of BBR, and silymarin. Fifty-three volunteers were enrolled and, in accordance with their risk score (RS), were divided to receive NUT (n = 25) or ATO 10 mg (n = 28) through the algorithm for patient allocation as reported in Figure 1. All recruited patients suffered from polygenic hypercholesterolemia and underwent hypolipidemic diet for 3 months at least in a primary prevention setting. Exclusion criteria included: recognized intolerance to NUT components, obesity, high or very high CV risk according to RS, 20 severe liver disease, nonpharmacologically controlled thyroid disease, active peptic ulcer, chronic inflammatory bowel disease, pregnancy and breastfeeding, and treatment with lipid-lowering therapy in the 30 days before enrollment.
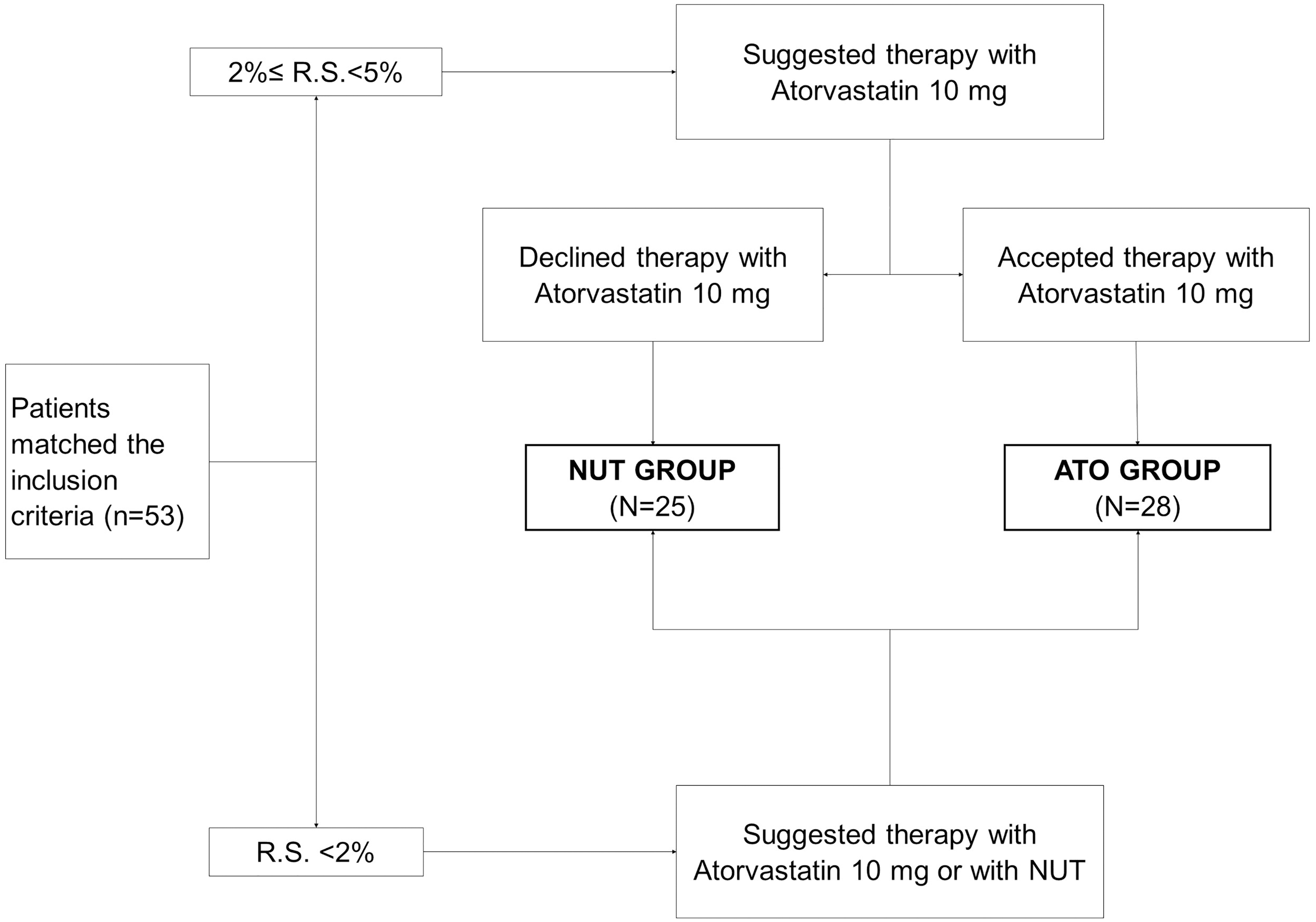
CONSORT flow diagram. Fifty-three patients matched the inclusion criteria and were divided into two different decision directions according to individual RS. When 2% ≤ RS <5% ATO was primarily suggested to the patients and, just if they declined it, NUT was suggested. According to their decision, they were assigned to ATO or NUT groups. Otherwise, when RS <2% was suggested to both ATO and NUT and, according to their preference, they were assigned to ATO or NUT groups. ATO, Atorvastatin; NUT, nutraceutical; RS, risk score.
Patients underwent evaluation of body mass index (BMI), RS, and treatment tolerance at both enrollment and end of the study. The study planned an 8-week-long treatment with NUT or ATO and, at the final visit, patients were invited to return the used blisters to check their adherence, counting the remaining pills. The study was approved by the Institutional Review Board of IRCCS Ospedale Policlinico San Martino (Genoa, Italy) and conducted in accordance with the guidelines of the Declaration of Helsinki. An informed consent was signed by all patients before the study entry.
Laboratory measurements
TC, high-density lipoprotein cholesterol (HDL-C), LDL-C, and triglycerides (TG) were measured in all patients, whereas PCSK9 levels and CLC were measured only in the NUT group. The laboratory workers were not aware of the treatment assigned to the patients.
For PCSK9 assay one serum aliquot from each patient was tested by colorimetric enzyme-linked immunosorbent assay from R&D Systems (Minneapolis, MN, USA). The minimal limit of detection was 125 pg/mL, the mean intra- and interassay coefficient of variation was at the accepted threshold of less than 8%. Measurement of CLC is carried out by enzymatic determination on cell extracts as already described and well established. 21
Treatments
ATO 10 mg was prescribed as common clinical practice (one tablet/day). A NUT supplement, produced by PharmExtracta (PC, Italy), registered at the Italian Ministry of Health as BerberolK in accordance with Legislative Decree 2004 May 21, n.169 was used in the NUT group. BerberolK (one tablet/day) contains 500 mg/dose of BBR from B. aristata (96% as BBR), 105 mg/dose of silymarin from Silybum marianum (≥60% as flavanolignans), and 50 mg/dose of Monakopure™-K20 from M. purpureus fermented rice extract (20% MonK and KA in the ratio 1:1; secondary monacolins J, JA, M, MA, L, LA, X, and XA, plus dehydromonacolins DMK, DMJ, DMM, DML, and DMX <0.2% total, and citrinin <50 ppb). The total duration of the treatments was 8 weeks.
Study endpoint
The primary endpoint of the study was to evaluate the effects of BerberolK on lipid profile in comparison with low-dose ATO therapy in a cohort of dyslipidemic patients at low/intermediate CV risk. As secondary endpoints, PCSK9 serum levels and CLC were measured in patients receiving NUT to better investigate the antiatherogenic effect of this dietary supplement.
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistics 22 (Armonk, NY, USA). A post hoc analysis was performed and resulted in a power of .82 considering a noninferiority margin of 16 mg/dL of LDL-C variation between ATO and NUT groups. The normality of variables was verified by Kolmogorov–Smirnov test. Intergroup and intragroup comparisons were then drawn by two-tailed Student's t-test for unpaired and paired samples, as appropriate. Univariate and multiple regression analyses were also performed. Data are expressed as mean ± standard deviation.
Results
Baseline and overtime differences among the two study groups
All enrolled patients (33 women and 20 men) completed the trial according to the study design and returned after 2 months. No bias of tablet assumption occurred at blister check. According to the study design, we categorized patients in the ATO (n = 28) and NUT (n = 25) groups. Nobody reported adverse events to treatment. Demographic and anthropometric parameters at baseline overall and according to the group division are shown in Table 1. No significant differences were found in terms of age, sex, BMI, HDL-C, and TG across the two study groups. Instead, mean values of TC, LDL-C, and RS were higher in patients treated with ATO 10 mg (P < .05 for all) (Fig. 2A – D). Figure 2 also reports overtime variations after 8 weeks of treatment.

Baseline and follow-up after treatment of lipid parameters, PCSK9, and CLC in ATO Group and NUT Group.
Baseline Demographic and Anthropometric Characteristics in All Patients Together, in ATO Group, and NUT Group
Data are expressed as mean ± standard deviation.
P < .05 (ATO group vs. NUT group).
ATO, Atorvastatin; BMI, body mass index; NUT, nutraceutical.
The ATO group was characterized by a significant decrease of TC (−22.3%), HDL-C (−5.5%), LDL-C (−27.5%), and TG (15.0%). Significant reduction in TC (−18.6%), LDL-C (−25.8%), and TG (11.0%), but not HDL-C were also observed in the NUT group (Fig. 2A – D and Fig. 3). At the end of treatment, no significant differences in the lipid profile were observed among the two study groups.

Individual LDL-C variations after treatment in
Effect of NUT on serum PCSK9 levels
Figure 2 also showed baseline and follow-up levels of PCSK9 and CLC in the NUT treatment group. After 8 weeks of treatment, PCSK9 significantly increased (+25.6%; from 294.3 ± 109.5 to 369.7 ± 109.8 ng/mL; P < .01). Furthermore, a direct linear relationship of baseline PCSK9 values was observed with TC at baseline and with both TC and LDL-C at follow-up (Fig. 4A–C). Furthermore, multiple regression statistics showed a proportionally direct linear correlation between PCSK9 levels at baseline and follow-up, and the levels of TC and LDL-C. According to the LDL-C percentage reduction, 19 patients in the NUT group were then categorized into three groups: nonresponder (NR) in which LDL-C increased, low responder (LR), and high responder (HR) characterized by LDL-C of 0–20% and >20%, respectively (Fig. 5). Analyzing the mean variability of PCSK9 within these groups we observed that in both the LR and HR groups, PCSK9 variation was statistically significant between baseline and follow-up (P = .01 and P = .04, respectively); Furthermore, PCSK9 levels were significantly higher in the low as compared with the HR group (P = .09). Conversely, nonsignificant decreasing trend of variations were recorded in the NR group (P = .13), which was characterized by higher levels at baseline in comparison with both LR and HR groups (P = .03 and P = .04, respectively).

Cartesian representation of linear regression between
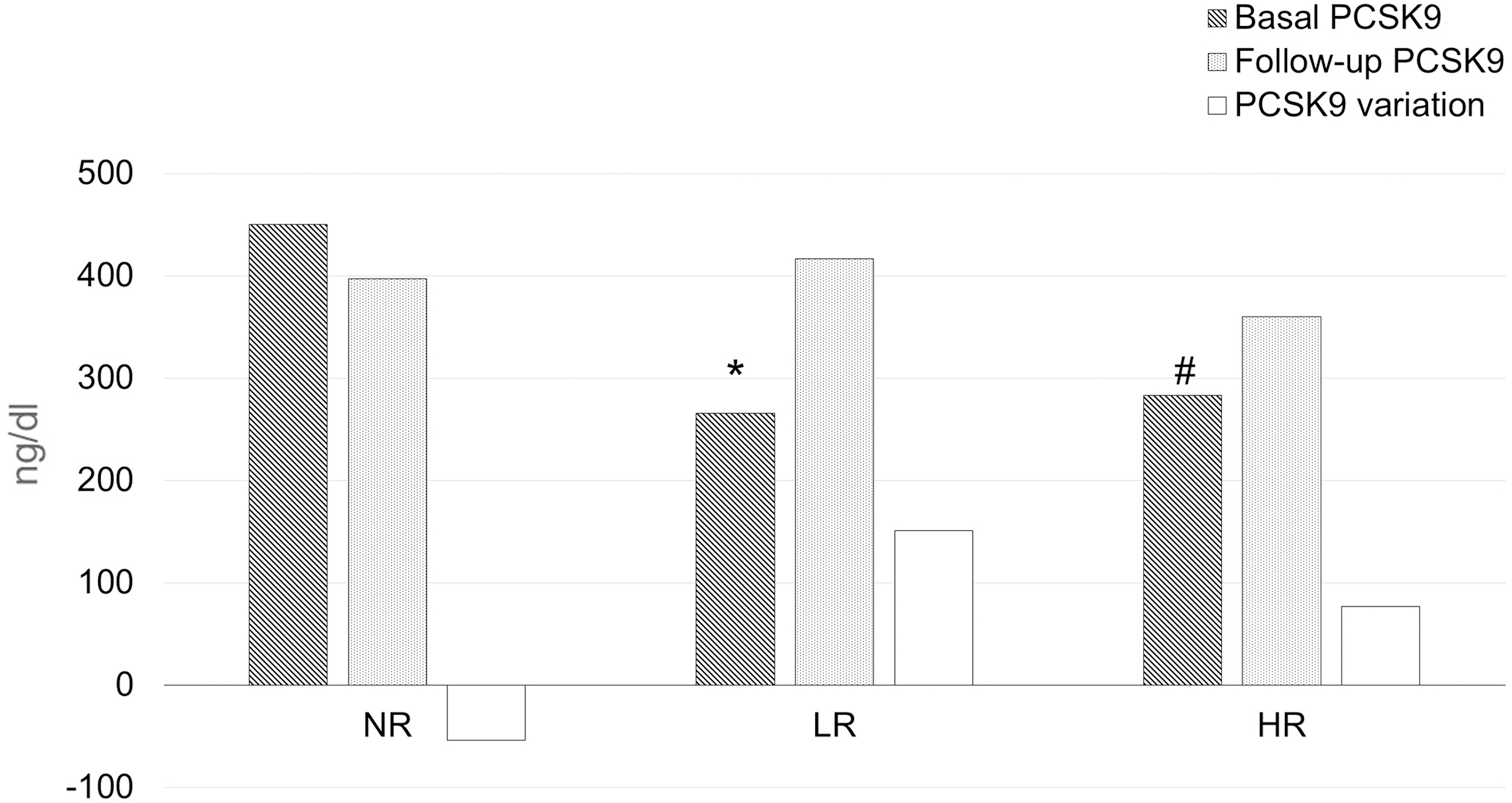
Schematic view of basal, follow-up, and variations of PCSK9 levels in the three different response groups: NR with LDL-C reduction ≤0%, LR with reduction 0% < LDL-C ≤ 20% and HR with reduction LDL-C > 20%. *P < .05 basal versus follow-up in LR group; # P < .05 basal versus follow-up in HR. HR, high responder group; LR, low responder group; NR, nonresponder group.
Effect of NUT on CLC
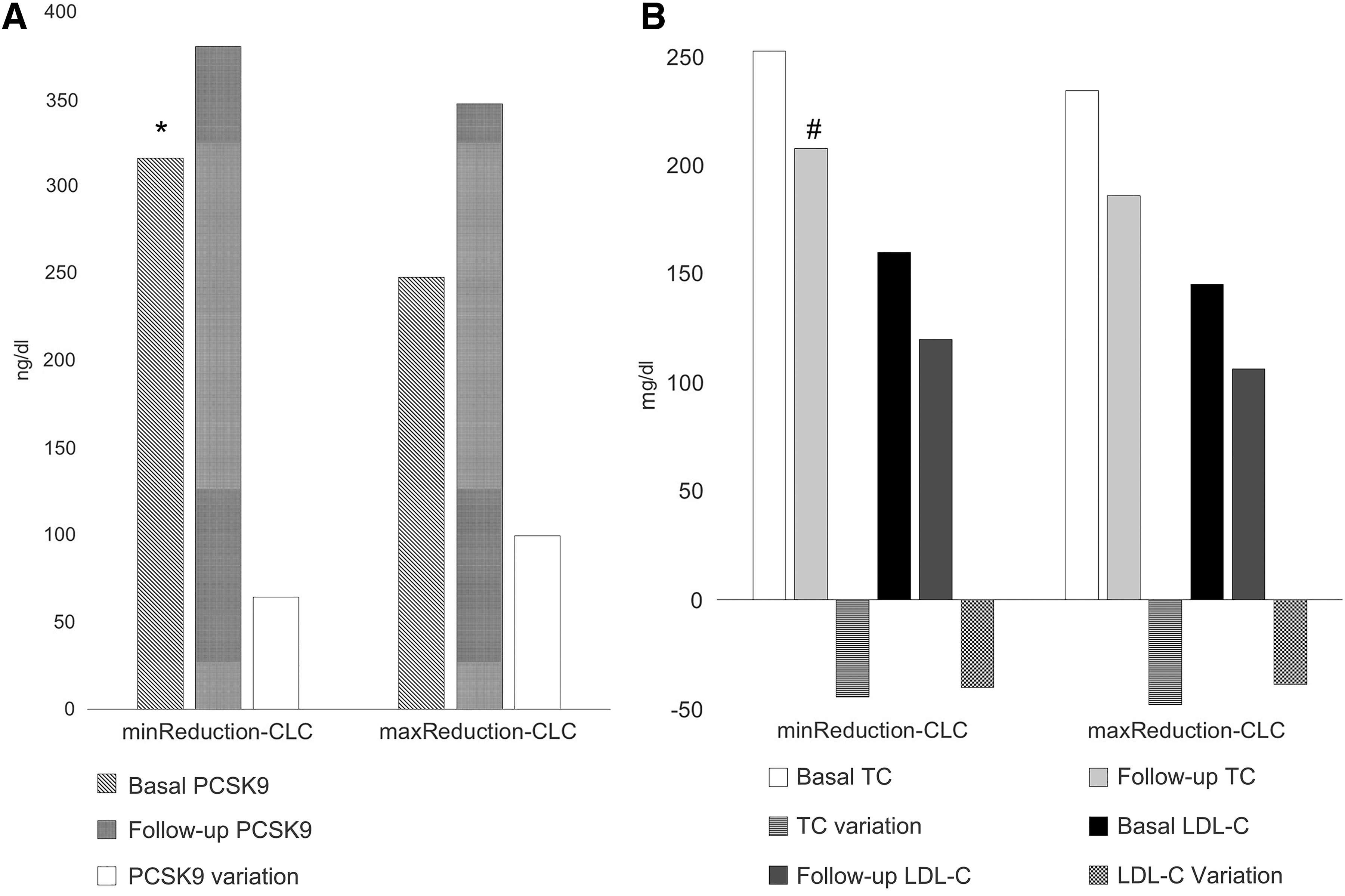
After 8 weeks, CLC was reduced in all NUT-treated patients, from 34.2 ± 11.6 to 26.0 ± 10.9 μg/mg protein (−24%; P < .001). According to the mean CLC reduction, patients were categorized in maximum or minimum CLC reduction (min/max CLC reduction), whether it was lower than −8.22 μg/mg protein or greater. Baseline PCSK9 values were higher in the min CLC reduction group (P < .05). However, no significant differences in variation were observed after treatment in the two study groups, but only slight nonstatistical PCSK9 increase in the max CLC reduction group (+99 vs. +64 ng/mL; P = .45) (Fig. 6A). Finally, lower levels of TC and LDL-C characterized min CLC reduction group, achieving statistical significance for CT at follow-up (P < .05) (Fig. 6B).
Discussion
The main finding of the present pilot study is that NUT is comparable to ATO 10 mg in improving lipid profile. In fact, although, in our study, we found a significant difference in TC reduction (respectively −58.25 ± 24.2 vs. −46.0 ± 23.3 mg/dL, P < .05) between ATO Group and NUT Group, this difference may be influenced by higher baseline TC (260.9 ± 25.0 vs. 246.8 ± 32.2 mg/dL, P < .05) and a significant reduction of HDL-C values in ATO group. LDL-C variation comparing the two treatment groups, was not statistically different although post hoc statistical power achieved significance just for difference of mean higher than 16 mg/dL. Figure 3 shows the individual reductions of LDL-C for all patients. We observed a strong individual variability that, in a small number of cases, such as ours, can largely influence the mean reduction and further explain the slight difference in effectiveness that is observed between treatment groups.
The effect of treatment with ATO 10 mg was not as effective as in large clinical trials, 22,23 which respectively showed a reduction after 1 year of TC treatment between 24% and 26%, LDL-C between 35% and 39%, and TG between 17% and 19%. Some smaller studies 24 –26 observed lower reductions in TC, LDL-C, and TG that are similar to the reductions obtained in our study. We also observed in the ATO group a significant reduction of HDL-C (−5.5%) in agreement with some literature data. 22 In a retrospective analysis, 27 which analyzed the treatment with the same NUT, a higher reduction, than in our study, of TC (−24.7%), LDL-C (−31.7%), and TG (−19.1%) was obtained. However, in this retrospective analysis, the baseline levels of TC, LDL-C, and TG were higher than ours and furthermore, according to the authors of the article, a retrospective study can suffer by some bias and limitations. In a prospective study, 28 a sample of patients comparable to ours for baseline LDL-C, showed a reduction of LDL-C similar to our patients. Banach et al. 12 reported that the MonK–BBR combination induced an LDL-C reduction between −20% and −25%, like one obtained in our study. Furthermore, products containing MonK alone, cause a lower LDL-C reduction (−15% to −25%) compared with the NUT used in our study. To the current knowledge, there are no comparative studies between ATO and the NUT used in our study. In the previously considered retrospective analysis, Lovastatin 20 mg was compared with the same NUT used in our study and the NUT treatment was more effective. 27 Statin treatment, and similarly MonK, act both on the inhibition of HMGCoA-reductase, 29 –31 and also on the upregulation of sterol regulatory element-binding protein-2, a transcriptional factor responsible for increase in the expression of genes such as LDL-R and PCSK9. 32 –34 On the other hand, PCSK9 promotes a degradation activity on LDL-R and may cause a lower LDL-R expression on the expressing cell membrane 35 –37 (Fig. 7).
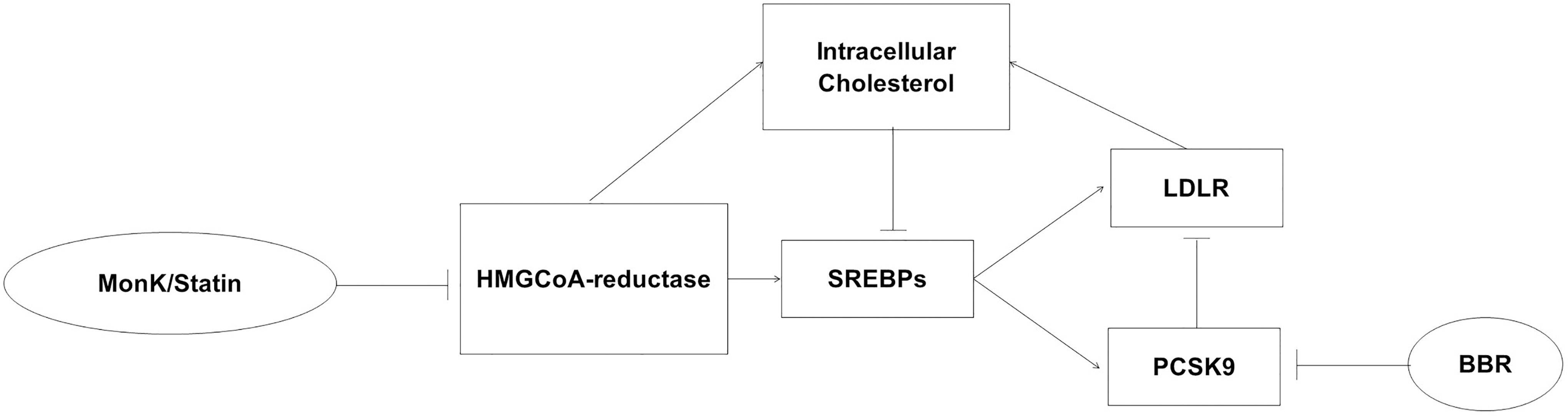
Schematic view of the cholesterol homeostasis and of the MonK/statin and BBR effects on this biological pattern. LDL-R and HMGCoA-reductase actions are mainly responsible for the increase in intracellular cholesterol that, on the other hand, inhibits SREBPs; these groups of transcriptional factors upregulate both LDL-R and PCSK9. This latter has an inhibitory action on LDL-R, resulting in a decrease in intracellular cholesterol and in a greater HMGCoA-reductase activity by SREBPs. The net result of these homeostatic loop determines the levels of hepatic origin lipoproteins in the body. MonK and BBR, by inhibiting HMGCoA-reductase and PCSK9, respectively, they are able to move this complex mechanism toward a lower capacity to produce cholesterol. BBR, Berberine; HMGCoA-reductase, 3-hydroxy-3-methyl-glutaryl-CoA reductase; LDL-R, low-density lipoprotein receptor; MonK, monacolin K; SREBPs, sterol regulatory element-binding proteins.
Despite increase of PCSK9 levels in serum during treatments with HMGCoA-reductase inhibitors, the key role of these treatments in the reduction of CV disease-associated morbidity and mortality and all-cause mortality is largely supported by very strong scientific evidence. 38,39 In a study by Adorni et al., 40 23 patients were treated with a different NUT combination containing 3.3 mg of MonK, and after 16 weeks, the authors did not observe a significant increase in serum PCSK9 levels; in contrast, in our study, we observed a significant increase in PCSK9 levels that could be caused by both the higher concentration of MonK (10 mg) and the purification and standardization technique used in the extraction from the red yeast rice, as if we had achieved a more statin-like effect.
The correlation between PCSK9 levels and some lipid parameters observed in our study is consistent with the literature 41 –43 ; this direct linear correlation exists both at baseline and at follow-up, however, the ordinate at the origin (intercept) at follow-up results to be shifted toward lower lipid values to confirm the weak relationship existing between reduction of TC and LDL-C and variation of PCSK9 in our study. As further confirmation of the latter analysis, the linear regression between PCSK9 variations, and baseline and follow-up lipid parameters, and their reduction after NUT treatment is not statistically significant, so LDL-C reduction resulted independent from PCSK9 variation.
In the literature, the treatments with statin/MonK and BBR are described to have an opposite effect on the PCSK9 expression and, therefore, also on its serum levels. The action of BBR is to reduce disruption of LDL-R by inhibiting the PCSK9-mRNA expression. 44 Moreover, the association of HMGCoA-reductase inhibitor and BBR leads to higher expression of LDL-R-mRNA compared with statin alone. 36 In our clinical records, circulating PCSK9 levels were on average higher than baseline, with strong individual variability after treatment with NUT. By comparing NUT treatment response groups, PCSK9 levels increased less in HR than in the LR group, and in the NR group it was not changed. The interindividual efficacy of treatment in the three groups may explain the different results: in NR patients, the lack of PCSK9 increase may be related to the low influence of MonK, whereas the lower increase of PCSK9 in HR compared with LR can be linked to the PCSK9 inhibitory action of BBR. Different efficacy of BBR may depend on its great individual variability of intestinal absorption. The BBR is a substrate of some membrane transporters, such as P-gp and multidrug resistance protein 1 (MRP1), which extrude BBR from the enterocytes. In addition, BBR increases the expression of P-gp, further reducing its absorption. 17,45
CLC is used as a surrogate parameter to evaluate the risk of developing atherosclerosis promoting the foam cell formation. Therefore, a reduction in CLC correlates with a lower atherogenic capacity of the circulating macrophages. 5,7 In our study, we observed a significant CLC reduction in all NUT-treated patients. This effect may be related, in most cases, to the reduction of CT and LDL-C levels caused by treatment with NUT. In support of this hypothesis, we observed at follow-up lower TC (P < .05) and lower LDL-C levels (P = .13 NS) in the maxReduction-CLC group compared with minReduction-CLC group. Another support for our data comes from the literature that highlights how LDL-C reduction causes direct CLC reduction. 8 In agreement with the previous discussion about the average reduction of PCSK9 levels in NR, the CLC reduction observed in this group (NR) can be caused by BBR action. In fact, BBR showed on human and mouse macrophages in vitro, an inhibitory effect on serum-induced cholesterol accumulation through cholesterol macropinocytosis inhibition. 46 Furthermore, BBR is described as a mild inhibitor of PCSK9-mRNA. 36 In the maxReduction-CLC group, PCSK9, TC, and LDL-C levels both at baseline and at follow-up were on average lower than in the minReduction-CLC group, considering that the statistical significance was achieved just for PCSK9 basal levels and TC follow-up levels, probably due to the low sample size. We can suppose that a lower PCSK9-mediated inhibition of LDL-R in the liver, due to lower mean PCSK9 levels, results in greater efficacy of MonK treatment. Therefore, TC and LDL-C lower levels and greater CLC reduction were observed with lower PCSK9 mean levels.
This study has some limitations represented by the small sample size and the lack of data concerning the plasma modifications of PCSK9 and CLC in the ATO group. Certainly, the low data available did not allow for many statistically significant results. Moreover, it would have been remarkable measuring the BBR's bioavailability; unfortunately, the biochemical assay was not available. Finally, the lack of blinding in treatment allocation is another limitation of this pilot study conducted in the context of common clinical practice. With these limitations, this work may be considered a pilot study and is necessary to carry out new studies to confirm our results.
In conclusion, NUT is comparable in LDL-C-lowering efficacy to the ATO 10 mg treatment in the context of common clinical practice. Highly purified MonK+KA in NUT treatment is effective to raise PCSK9 levels, but probably BBR action may partially inhibit the PCSK9 increase only when more bioavailable. Ex vivo NUT treatment reduces CLC with a probable antiatherogenic action.
Footnotes
Author Disclosure Statement
Livia Pisciotta received support for this study from Pharmextracta. Francesco Di Pierro is a member of the Pharmextracta Scientific Board. For all other authors, no competing financial interests exist.
Funding Information
No funds were received for this study.