
Abstract
The aim of this study was to investigate the efficacy and safety of curcumin formulation with a polyvinylpyrrolidone-hydrophilic carrier (CHC*; Diabec®—AlfaIntes, Italy) for the treatment of macular edema (ME) from uncommon etiologies. We conducted retrospective interventional case series, reviewing the medical records of patients referred to the Eye Center, Humanitas Hospital, Bergamo due to persistent ME related to uncommon causes and treated by oral administration of CHC. The main outcomes assessed were best-corrected visual acuity (BCVA), central macular thickness (CMT), and the presence of intraretinal and/or subretinal fluid (SRF). Only patients with a minimum follow-up (f/u) of 6 months were included. The occurrence of any adverse effect was registered. Thirty-one eyes of 30 patients were included, with a mean f/u of 8.32 ± 1.77 months. Of them, 9 patients (10 eyes) were affected by postoperative ME and 21 by chronic central serous chorioretinopathy. Median BCVA significantly improved after treatment, changing from 0.3 [0.16–0.5] to 0.1 [0–0.3] logarithm of the minimum angle of resolution (P < .001). Also CMT was significantly improved, as it decreased from 400 [364–438] μm before treatment to 280 [242–307] μm at the last f/u visit (P < .001). The complete absorption of intraretinal/SRF was detected in 23 of 31 eyes (74%) at the final f/u. No adverse effects were registered. In conclusion, treatment with CHC was effective and safe for eyes affected by ME of various uncommon etiologies, resulting in significant improvement of both functional and anatomical outcomes, with the complete resolution of the edema in the majority of cases (74%).
Introduction
Awide variety of retinal diseases can be complicated by macular edema (ME), a vision-threatening condition consisting of intraretinal and/or subretinal accumulation of fluid in the macular area. 1 Multiple and not completely understood pathogenetic mechanisms contribute to an altered retinal hydro-ionic homeostasis resulting in fluid accumulation and, potentially, severe anatomic and functional impairment of the retina. 1
The ME is mainly caused by diabetic retinopathy (DR), choroidal neovascularization associated with age-related macular degeneration (AMD), and retinal vein occlusion (RVO), whereas less common causes can be central serous chorioretinopathy (CSC), previous intraocular surgery, inflammatory diseases, inherited retinal dystrophies, and so on. 1 Contrarily to the former, for the latter there is no “on label” treatment currently available. Therefore, different therapeutic options have been used, such as topical, intravitreal, or periocular corticosteroids, topical nonsteroidal anti-inflammatory drugs (NSAIDs), laser photocoagulation (LP), subthreshold micropulse LP (SMLP), photodynamic therapy (PDT), and intravitreal antivascular endothelial growth factor (VEGF) agents. 2 –5
Recently, curcumin, a natural bioactive polyphenol extracted from Curcuma longa L. with its analogous curcuminoids, demethoxycurcumin and bisdemethoxycurcumin, has been proposed as a promising therapeutic option in retinal diseases, including the ones characterized by ME, due to its pleiotropic effects. 6,7 Indeed, this compound has shown anti-inflammatory, antioxidant, immunomodulating, and antiangiogenic properties due to the capability to influence cellular processes, such as inflammation and apoptosis, through the activation and/or expression modulation of several transcription factors, growth factors, chemokines, and interleukins. 6,7 Preclinical studies have reported beneficial effects of curcumin in terms of inhibition of proliferative vitreoretinopathy in rabbit eyes 8 and attenuation of retinal ultrastructural changes induced by diabetes in rat eyes. 9 However, a main limitation of the therapeutic use of curcumin in humans has been the poor bioavailability. 10 To overcome this issue, numerous formulation strategies have been adopted, such as dispersion in a lecithin formulation (Meriva®; Indena SpA, Milan, Italy), 11 curcumin liquid droplet micromicellar formulation, 12 the combination of curcumin formulation (CurcuWIN® Dry Powder 20%) with a polyvinylpyrrolidone-hydrophilic carrier (CHC; Diabec®—AlfaIntes, Italy), 13 nanocurcumin, combination with piperine, and so on. 14 Despite the growing number of promising results from preclinical studies, 6 –9 we found only few clinical studies reporting the outcomes of curcumin-based treatment for retinal diseases. 15 –17 In particular, the curcumin-lecithin (CL) formulation (Meriva; Indena SpA) has been associated with improved visual acuity (VA) and reduced ME in both CSC 15,16 and DR. 17 Compared with the formulation used in the abovementioned studies, CHC showed a significantly higher appearance of the curcuminoid in the blood 13 and provided detectable levels of curcumin in the rabbit retina after oral administration. 18
On the basis of this background, our study aimed to investigate if CHC may be an effective and safe treatment for patients affected by ME from uncommon etiologies.
Materials and Methods
Study design and participants
We conducted a retrospective, uncontrolled interventional study on adult patients referred to the Eye Center of Humanitas Hospital of Bergamo between June 2018 and December 2018 due to persistent ME from uncommon etiologies and treated with oral administration of CHC (Diabec). This study conformed to the Declaration of Helsinki and was approved by the institutional review board.
We included patients older than 18 years affected by symptomatic ME from uncommon etiologies, persistent for more than 3 months and with a minimum follow-up (f/u) of 6 months. Both naive and not naive patients were enrolled, and all previous treatments were registered. We excluded patients with: (1) any other uncontrolled or untreated ocular diseases potentially affecting best-corrected VA (BCVA) and response to treatment; (2) history of AMD, DR, and RVO; (3) angiographic evidence of choroidal neovascularization; (4) history of systemic therapies, laser treatment, or intravitreal injections within 3 months before starting CHC treatment (baseline); (5) history of intravitreal implants of steroids within 6 months of the baseline; and (6) media opacity interfering with BCVA and optical coherence tomography (OCT) acquisition.
All patients underwent a comprehensive ophthalmic examination at the baseline and at each f/u visit. We collected data regarding age, sex, and ocular history. The ophthalmic examination included BCVA assessment in Snellen fractions, applanation tonometry, slit lamp biomicroscopy, dilated fundus examination, and spectral domain (SD)-OCT imaging. At the baseline, the diagnosis was confirmed by fluorescein angiography combined with indocyanine green angiography in case of CSC.
SD-OCT scan protocol
We used the Spectralis SD-OCT with eye tracking (Heidelberg Engineering GmbH, Heidelberg, Germany). At each visit, the following scans were acquired in all eyes: a high-definition horizontal fovea-centered cross line B-scan at 30° and the horizontal macula raster consisting of 49 B-scans 120 μm-spaced over an area of 20° × 20°. The “Thickness Map” function was used to measure automatically the mean central macular thickness (CMT), based on the mean retinal thickness within a circular area of 0.5-mm radius from the foveal center. Two masked observers (M.F. and D.A.) independently evaluated OCT images quantitatively and qualitatively. A third observer (M.R.R.) resolved any case of disagreement.
Treatment protocol
All patients were treated with the same treatment protocol, consisting of a loading phase of two capsules daily for 1 month, one in the morning and one in the evening, followed by a maintenance phase of one capsule every 24 h, in the morning or in the evening, for 2 months. Each CHC capsule contains 60 mg of CurcuWIN Dry Powder 20% (curcuminoids 20–34%, hydrophilic carrier 60–80%, and natural antioxidants 1–5%).
Safety assessment
At each f/u visit we investigated frequency and severity of any adverse events.
Statistical analysis
To carry out the statistical analysis, we used STATA/IC 15.1 software and converted all Snellen BCVA values into logarithm of the minimum angle of resolution (logMAR) units. All data were expressed as median ± interquartile range. For the comparison of variables at baseline and each f/u visit, we used the Wilcoxon test for paired samples. The differences were considered statistically significant if P value was ≤.05.
Results
We retrospectively collected data on 31 eyes of 30 patients affected by persistent postoperative macular edema (pME) (10 eyes of 9 patients) and chronic CSC (21 eyes of 21 patients). The overall mean age was 52.93 ± 13.66 years, ranging from 54 to 74 years in pME group and from 28 to 65 years in CSC group. In CSC group there was a clear male predominance (male/female ratio of 6). The baseline demographic and clinical findings are shown in Table 1. At the baseline, all eyes with chronic CSC had a diffuse and broad leaking pattern without distinct leaking points on angiography. Ten patients were previously treated with a combination of topical NSAIDs and oral acetazolamide, whereas four patients received a laser treatment more than 5 months before CHC therapy, namely PDT in two patients, LP in one patient, and SMLP in one patient. Among the patients suffering from pME, seven eyes experienced ME after cataract surgery, one after pars plana vitrectomy, and two after combined phaco-vitrectomy. The mean interval between the surgery and the onset of ME was 6.3 ± 2.63 weeks. With regard to previous therapies, three patients received topical NSAIDs and one patient underwent an anti-VEGF injection 6 months before CHC treatment.
Baseline Demographic and Clinical Findings
BCVA, best-corrected visual acuity; CMT, central macular thickness; CSC, central serous chorioretinopathy; IQR, interquartile range; logMAR, logarithm of the minimum angle of resolution; pME, postoperative macular edema.
All patients were assessed 1, 3, and 6 months after starting CHC treatment. The overall mean f/u was 8.32 ± 1.77 months (range: 6–12 months).
Best-corrected VA
The comparison between BCVA at the baseline and each f/u showed a statistically significant improvement in BCVA in overall patients (P < .001 for all), as well as in both groups (P ≤ .01 in pME group for all time points and P < .001 in CSC group for all time points) (Fig. 1). In pME group the median BCVA (logMAR) was 0.45 [0.3–0.5] at the baseline, 0.3 [0.3–0.5] at 1-month f/u, 0.26 [0.16–0.4] at 3-month f/u, 0.26 [0.16–0.5] at 6-month f/u, and 0.31 [0.16–0.5] at the last f/u, whereas in CSC group the BCVA was 0.22 [0.16–0.3] before starting CHC treatment, 0.1 [0.05–0.22] at 1-month f/u, 0.05 [0–0.1] at 3-month f/u, 0.05 [0–0.1] at 6-month f/u, and 0.05 [0.05–0.13] at the last f/u. Comparing the BCVA at the end of CHC treatment (3-month f/u) with the final BCVA, no statistically significant difference was detected in both pME (P = .24) and CSC patients (P = .4).

BCVA in patients treated with CHC. BCVA before starting treatment (baseline) and at 1-month follow-up (1-m), 3-month follow-up (3-m), 6-month follow-up (6-m), and the last follow-up (final f/u) in overall patients
Anatomical findings on OCT
The overall CMT and CMT in both groups at baseline and at each f/u visits are shown in Figure 2. The reduction in CMT was statistically significant at each f/u visit in both pME (P = .005) and CSC group (P < .001). In pME group, CMT changed from 503.5 [435–569] μm at the baseline to 291 [257–328] μm at the last f/u visit in pME group, whereas in CSC group CMT changed from 376 [359–405] μm before treatment to 274 [242–305] μm at the final f/u.
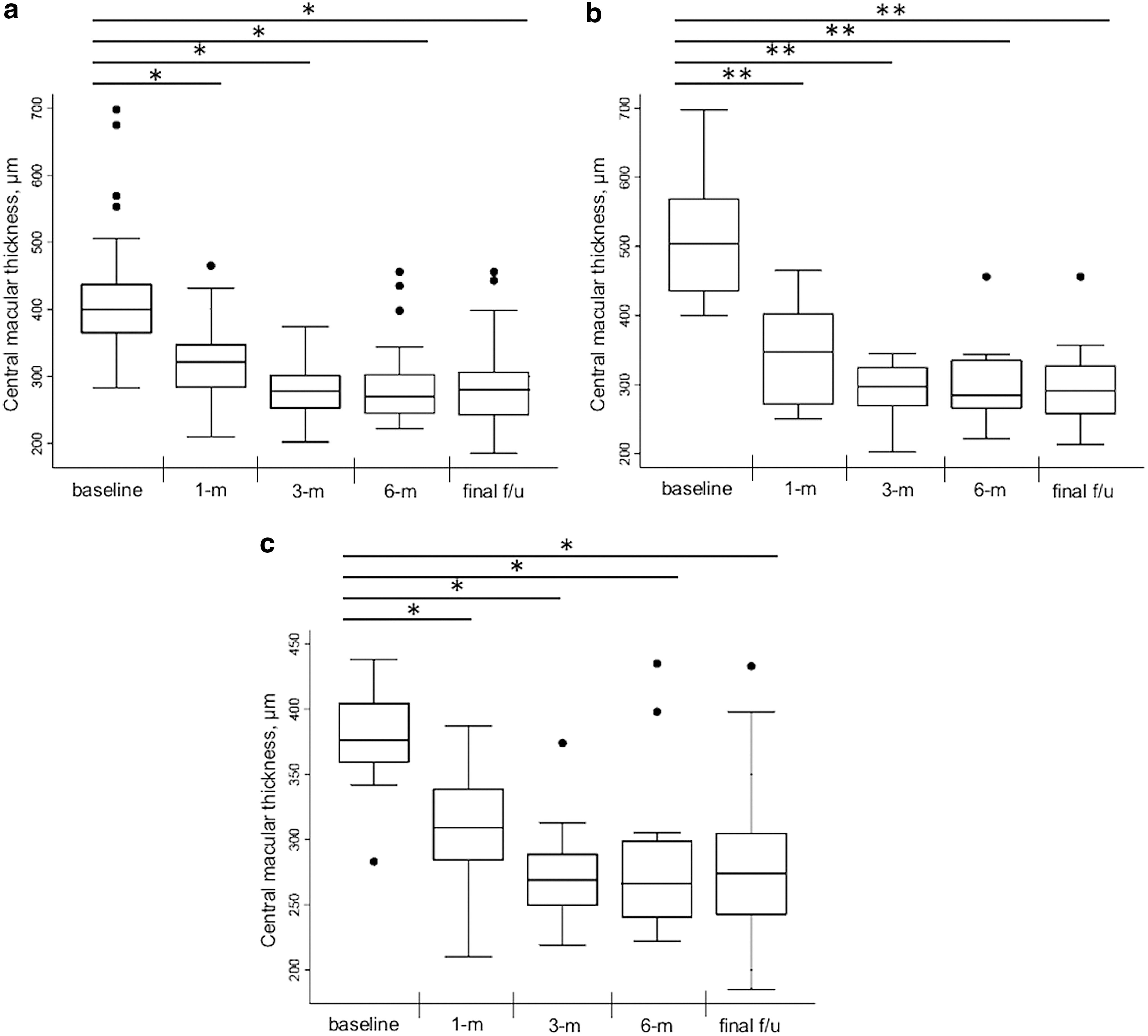
CMT in patients treated with CHC. CMT before starting treatment (baseline) and at 1-month follow-up (1-m), 3-month follow-up (3-m), 6-month follow-up (6-m), and the last follow-up (final f/u) in overall patients
The CMT at 3-month f/u did not significantly decrease compared with the CMT at both 6-month and last f/u visit (P = .8 in pME group and P = .5 in CSC group).
At the last f/u visit, 23 of 31 eyes (74%) had complete absorption of intraretinal and/or subretinal fluid (SRF) (Fig. 3). In the pME group, the complete resolution of ME was detected in five eyes (50%) at 1-month f/u and in seven eyes (70%) at the following f/u visits. Of the remaining cases, two eyes had small residual cysts with stable VA, and one patient experienced the recurrence of ME at 6-month f/u visit. In the CSC group, the SRF appeared completely reabsorbed on OCT in 2 eyes (9%) at 1-month f/u and in 15 eyes (71%) at 3-month f/u. At 6-month visit, further three eyes showed the complete disappearance of SRF, whereas one eye experienced recurrence. At the last f/u recurrence was detected in two eyes (6 and 10 months after starting CHC treatment, respectively), and three eyes (14%) showed persistent SRF for the entire f/u period.
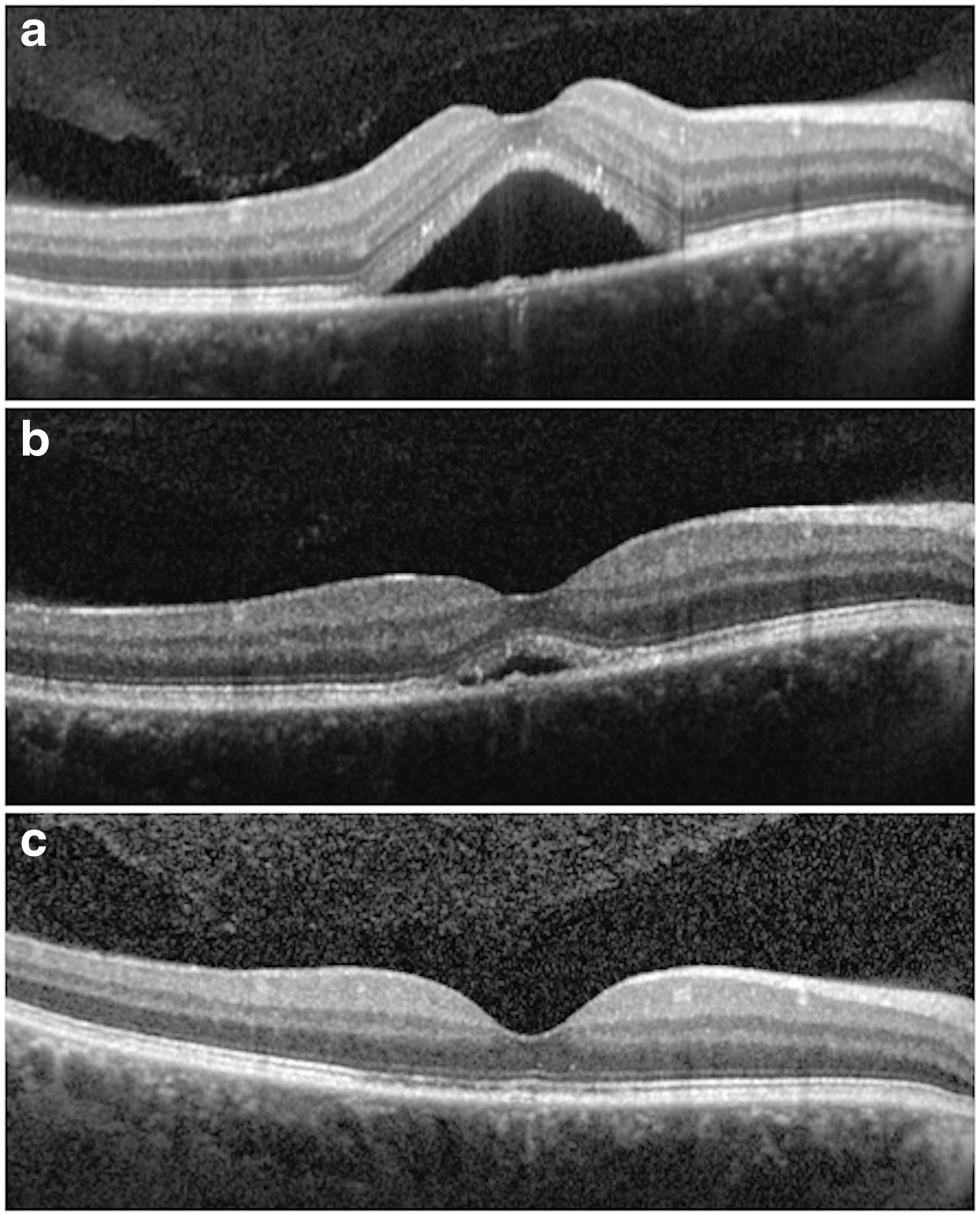
Structural finding in chronic CSC after CHC treatment.
Safety assessment
No patient experienced adverse effect during the f/u period.
Discussion
Our study evaluated functional and anatomical outcomes of oral CHC treatment in patients affected by ME from CSC and pME. Both conditions are indicated as uncommon causes of ME as they are less frequent than the most common retinal vascular diseases, namely DR, RVO, and neovascular AMD. 1 Postoperative ME and CSC can have a self-resolving course without functional consequences and, thereby, therapy may not be required in the acute phase; however, the ME can persist or recur leading to retinal damage and severe functional impairment. 19,20 In this study we included only patients with ME persistent from more than 3 months, since in these cases the spontaneous resolution is unlikely. Several therapeutic strategies have been proposed with variable results, including NSAIDs, oral acetazolamide, and intravitreal anti-VEGF agents for both pME and CSC, corticosteroids for pME, and laser treatments (LP, SMLP, and PDT) for CSC. 2 –5 However, so far, no treatment has been approved by health authorities, and there is no consensus on the treatment of choice.
The emerging evidence of the pharmacological effects of curcumin led to consider this pleiotropic compound as a potential beneficial treatment in various retinal diseases, including ones complicated by ME. 6,7 Indeed, on one hand, ME is a multifactorial process in which many pathogenetic mechanisms play a role, such as release of inflammatory mediators, microglial activation, VEGF pathway, junctional complex alteration, oxidative stress damage, alteration of blood–retinal barriers (BRBs), and loss of the cells constituting the BRBs. 1 On the other hand, curcumin shows anti-inflammatory, antioxidant, antiangiogenic, neuronal- and vascular-protective, anticancer, and antimicrobial properties due to its capability to target and regulate multiple signaling pathways. 7 It has been documented about direct or indirect inhibitory effects of curcumin on cyclooxygenase, nuclear factor-κB (NF-κB), tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), IL-6, IL-8, and free radical production. 6 All the abovementioned molecules play a crucial role in the multifactorial pathogenesis of ME. Moreover, it has also been reported about an inhibitory activity of curcumin on lipoteichoic acid-activated microglial cells. 21 These cells are primarily involved in neuroinflammation and ocular inflammation. 21,22
However, the clinical use of curcumin has been limited by relevant disadvantages in its pharmacokinetic profile. Indeed, the compound is poorly soluble, poorly absorbed by gut, and rapidly metabolized and eliminated, resulting in poor bioavailability. 10,13 A multitude of formulation strategies have been made to increase its bioavailability. 11 –14 Moreover, it has to be noted that curcumin is one of three curcuminoids extracted from turmeric, namely demethoxycurcumin and bisdemethoxycurcumin, and different commercially available formulations can vary significantly in the relative concentrations of these analogs. 13 This finding may be clinically relevant since the three curcuminoids are not equivalent in terms of bioactivity and curcumin has the strongest antioxidant and anti-inflammatory activity. 23,24 In this study we administered CHC (Diabec), in which the turmeric extract, together with cellulosic derivatives and natural antioxidants, is dispersed on a polyvinylpyrrolidone-hydrophilic carrier to obtain a water soluble formulation. It has been reported that CHC was associated with the significantly higher hematic concentration of curcuminoids, whose curcumin was the major component, compared with unformulated standard curcumin, a combination of volatile oils of turmeric rhizome and curcuminoids, and a CL formulation. 13 Moreover, the oral administration of CHC in rabbits has been shown to provide retinal curcumin levels comparable to the concentrations assessed as effective in the in vitro tests, whereas the oral intake of two different formulations, namely CL and curcumin-piperine combination, led to undetectable retinal levels in the rabbit retina. 18
After CHC treatment, we found that overall BCVA and CMT significantly improved and the majority of patients experienced the complete resolution of intraretinal/SRF.
Among our cohort, nine patients were affected by pME (10 eyes). Postoperative ME, also known as Irvine–Gass syndrome when ME follows cataract removal, is a potential complication of any ocular surgical procedure. Although all the pathogenetic mechanisms leading to pME are not completely elucidated, it has been well established the predominant role of inflammation. 1 Indeed, the surgical trauma induces the alteration of the BRB and the release of various inflammatory mediators with consequent increase of vascular permeability and accumulation of intraretinal fluid. 1,25 In our subgroup of pME, we found that BCVA (logMAR) significantly improved at f/u visits changing from 0.45 [0.3–0.5] at the baseline to 0.31 [0.16–0.5] at the last visit. The reduction in CMT was significant, and ME completely disappeared in seven eyes (70%). Moreover, the two eyes with small residual cysts at the final f/u were stable in terms of BCVA and CMT, not requiring additional therapies. These encouraging results could be consistent with the established anti-inflammatory activity of curcumin. In particular, curcumin activates peroxisome proliferator-activated receptor-γ and transcriptional factors involved in anti-inflammatory and microglial response. 26,27 Moreover, curcumin has been associated to the downregulation of prostaglandin E-2, in addition to the abovementioned inhibitory activity on several pro-inflammatory molecules. 6 No previous studies evaluated the use of curcumin in pME; however, our results are consistent with those obtained with other therapeutic regimens. 19,28,29
With regard to the patients affected by CSC, we also found a statistically significant improvement in terms of both BCVA and CMT. Indeed, BCVA (logMAR) changed from 0.22 [0.16–0.3] at the baseline to 0.1 [0.05–0.22] at the last f/u visit, whereas CMT decreased from 376 [359–405] μm to 274 [242–305] μm with the complete reabsorption of SRF in 16 eyes (76%). Contrarily to pME, the exact pathogenesis of CSC has not been established yet. 1,19 However, the pleiotropic properties of curcumin may influence many of the mechanisms assumed to play a role in determining this condition. Among them, the relevant role of the focal disruption of the retinal pigment epithelium (RPE) and RPE barrier dysfunction is widely accepted. 1 In this regard, inflammatory mediators, such as TNF-α and IL-1β, have been shown to influence RPE polarity and permeability through their effects on junction proteins, 1 while the activation of NF-κB has been involved in the disruption of RPE barrier induced by oxidative stress. This may explain the beneficial effect of curcumin due to its anti-inflammatory and antioxidative activities (as described above). 6 Moreover, VEGF has been implicated in RPE enhanced permeability. 1 Preclinical studies reported that curcumin may decrease VEGF and that diabetic rats fed a curcumin diet had lower retinal levels of VEGF compared to controls. 30,31 It may also be argued that the vascular protective properties of curcumin may exert a beneficial effect on the choroidal vascular abnormalities described in CSC. 7
To the best of our knowledge, there are only two previous studies (on the same cohort of eyes at different follow-up times) reporting the outcomes in patients affected by CSC and treated with a CL formulation (Meriva; Indena SpA). 15,16 As we used a different curcumin formulation, a comparison may be interesting; however, we cannot directly compare the two studies for relevant methodological differences. First, Mazzolani et al. 15 included both non-naive and naive patients without specifying if the latter were in acute or chronic phase; we included patients with persistent edema to avoid the potential bias due to spontaneous resolution. Second, it has stated that patients received CL for the entire follow-up of the first study (6 months), but it is not clear the total duration of treatment regimen 15,16 ; contrarily, we treated all patients according to the same protocol for an overall duration of 3 months to evaluate if this regimen may lead to durable results. In this regard, we found that there was no statistically significant difference in both BCVA and CMT at 3-month f/u and the following f/u visits, suggesting that CHC may result in significant functional and anatomical improvement that may be maintained once the therapy is stopped. Finally, previous studies only described increase in BCVA and reduction in CMT without stating if the edema was completely resolved in any eyes. 15,16
This is a pilot study assessing the functional and anatomical results of an oral curcumin-based therapy in ME for CSC and, for the first time, pME; however, we acknowledge that there are some pitfalls, namely the small size of the sample and the duration of follow-up. Moreover, further studies will be necessary to compare different therapeutic strategies.
In conclusion, the oral administration of CHC in patients affected by ME from CSC and pME resulted in the increase of VA and the reduction of CMT, with the majority of eyes (74%) having the complete reabsorption of the intraretinal/SRF. Therefore, CHC may be an effective and safe therapeutic option in case of ME from uncommon etiologies.
Footnotes
Author Disclosure Statement
No competing financial interests exist
Funding Information
No additional funding was received for this article.