
Abstract
Acute radiation-induced esophagitis (ARIE) is among the most serious form of toxicities associated with definitive radiotherapy or chemoradiotherapy used for treatment of patients with esophageal cancer. Our preliminary phase I and II trials of lung cancer patients who received radiotherapy indicated epigallocatechin-3-gallate (EGCG) as a promising therapeutic option against ARIE. Therefore, we conducted a prospective phase II study to validate the efficacy and safety of EGCG in the treatment of ARIE. The patients who received chemoradiotherapy or definitive radiotherapy for treatment of esophageal cancer in the Shandong Cancer Hospital and Institute in China were enrolled for the present study. EGCG (440 μM) was administered with first onset of ARIE and then at weeks after final radiotherapy. The patients were monitored every week for dysphagia, Radiation Therapy Oncology Group (RTOG) score, and esophagitis-related pain. Moreover, tumor response and the effect on survival following the treatment were also evaluated. Comparison of the RTOG score in the first, second, third, fourth, fifth, and even sixth week after EGCG prescription and the first and second week after radiotherapy with baseline indicates a significant reduction. The tumor response rate was 86.3%. The overall survival rate in 1, 2, and 3 years was found to be 74.5%, 58%, and 40.5%. Oral administration of EGCG solution seems to be feasible for treating ARIE in patients with esophageal cancer who receive radiation therapy. EGCG might be an ARIE-reliever without compromising the efficacy of radiation therapy. A randomized study with a control group is needed for further evaluation.
Introduction
Esophageal cancer is among the deadliest forms of cancer. 1 In China, the most common form of esophageal cancer is esophageal squamous cell carcinoma (ESCC), mainly affecting the upper and middle thoracic esophagus. 2 Chemoradiation therapy is considered the standard treatment option for locally advanced esophageal cancer. 3 However, definitive radiotherapy frequently leads to the development of acute radiation-induced esophagitis (ARIE) characterized by odynophagia and dysphagia within 90 days of thoracic irradiation. The severity of such ARIE is commonly determined by Radiation Therapy Oncology Group (RTOG) and Common Terminology Criteria for Adverse Events (CTCAE) scores. Although the development of accurate radiotherapy, such as image-guided radiotherapy, has decreased the occurrence of ARIE, 4,5 it remains the most common dose-limiting adverse effect especially in cases of definitive radiation therapy.
Esophagitis is commonly managed by avoiding an irritant diet, as well as antidehydration and nutrition infusions 6 ; the WHO recommended analgesics, antacids, proton pump inhibitors, fungal preparations, immunomodulators, and topical anesthetics. 7 However, negative results were shown in many studies. Therefore, a new strategy for relieving ARIE is important to oncologists for the proper clinical management of affected patients.
Epigallocatechin-3-gallate (EGCG) is a molecule extracted from green tea. Previous research on green tea extracts has shown them to prevent the onset of carcinogenesis in epithelial cells due to their anti-inflammatory and antioxidative properties. 8 Many studies have also demonstrated that EGCG could be a potent radiation therapy sensitizer for killing cancer cells. 9 Other research has also demonstrated the anticancer potential of EGCG. 9,10
To investigate this potential further, we previously carried out a phase I study of EGCG for the treatment for ARIE induced by radiation. 8 We found oral application of EGCG to be feasible, safe, and effective for the treatment of ARIE for lung cancer patients. The findings of our phase I study prompted a subsequent prospective evaluation of other studies. RTOG scores of patients who received radiation therapy were significantly lower in patients prescribed EGCG compared with the untreated controls in lung cancer and breast cancer. 11 –13 These trials supported the safety and efficacy of orally administered EGCG for the treatment of ARIE.
Based upon the results of the previous study conducted by our research team, we designed this prospective phase II study aimed to evaluate the efficacy and safety of EGCG against ARIE in ESCC patients treated with chemoradiotherapy or definitively radiation therapy.
Materials and Methods
This prospective phase II study was designed to validate the safety of EGCG as well as to determine its efficacy against ARIE. It was carried out with prior approval by the Ethics Review Board of our center (registration no.-NCT01481818). All patients provided informed consent.
Patient enrollment
All patients who were enrolled had been admitted to our center for treatment. The criteria for inclusion were as follows: age >18 years, the Eastern Cooperative Oncology Group Performance Status (ECOG PS) 0–1, confirmed pathological ESCC, no previous exposure of thoracic radiation, adequate hematocyte count, normal hepatic and renal functions, FEV1 > 800 cc, and candidacy for definitive radiation therapy or chemoradiation therapy. The exclusion criteria were as follows: unknown or multiple esophageal cancer sites, unclear staging, lactating or pregnant women, known hypersensitivity or allergy to any kind green tea extract, and patients with esophageal fistula. Tumor staging was determined as described by the American Joint Committee on Cancer (AJCC), seventh edition.
Radiation/chemoradiation treatment
Chemoradiotherapy and definitive radiotherapy were carried out according to the standard prescribed dosage of intensity modulated radiation therapy (IMRT) at 1.8–2.0 Gy per fraction with total dose of 59.4–60 Gy. Computed tomography (CT) scans were obtained using Philips Brilliance CT Big Bore Oncology Configuration (Cleveland, OH) with patients in the supine position. The CT scan images were moved to an Eclipse treatment planning system (Eclipse 8.6; Varian Medical Systems). Gross tumor volume was determined depending upon positron emission tomography imaging or CT imaging based upon contoured maximal intensity projections aided by the results of X-ray and endoscopy.
Planning target volume (PTV) was set at 3 cm beyond the superior and inferior tumor borders and 1.5 cm beyond the lateral borders. The target dose to the edge of PTV was between 95% minimum and 105% maximum dose. Dosing constraints were mean lung dose ≤18 Gy and V20 of total lung ≤30%. Dosing to the spinal cord was less than 45.0 Gy; V50 of heart ≤45%. Dose–volume histograms were used to determine dosage to normal tissues. For concurrent chemoradiation therapy, patients were treated with either docetaxel plus cisplatin or with fluorouracil and cisplatin.
Study design
The primary endpoints of our study were the response of ARIE to EGCG and the toxicity of EGCG. Secondary endpoints were radiotherapy-induced tumor response and overall survival (OS).
To determine prognosis of ARIE response, we monitored RTOG ARIE score and patient-reported pain weekly. If we observed grade 1 RTOG score, the patient received EGCG solution. We chose an EGCG concentration of 440 μM concentration for this trial according to the results of our previous research. 11 EGCG (purity ≥95% by high-performance liquid chromatography) was purchased from HEP Biotech Co., Ltd (Ningbo, Zhejiang, China) and freshly dissolved in 0.9% saline. The time of administration was set as baseline. We recorded the dose of radiation therapy when grade 1 ARIE occurred. We then compared RTOG scores after the usage of EGCG with baseline scores. The purity and storage of EGCG are outlined in the previous study. 11
We also recorded pain using a numerical rating scale (NRS) and side effects according to CTCAE every week during radiation therapy and 2 weeks after radiation therapy using the same method. When grade 3 ARIE occurred, steroids, nonsteroidal anti-inflammatory drugs, and narcotics were prescribed to patients. Gastrostomy tubes were not to be used until grade 4 toxicity persisted for more than 3–4 days after the weekly adverse event evaluation.
Acute toxicities caused by EGCG were all scored using CTCAE and were evaluated when the first time EGCG was used. Toxicities were scored weekly during the course of radiotherapy until 2 weeks after the final dose.
For the secondary outcomes, tumor response was evaluated with CT imaging of the tumor 1 month after RT using standard version 1.1 of Response Evaluation Criteria in Solid Tumors (RECIST) guidelines. Tumor responses were grouped into progressive disease (PD) indicating nonresponders, and stable disease (SD) indicating partial response (PR) or complete response (CR) groups; the latter indicating response to radiation therapy. In the first year after enrollment, patients were followed up every 3 months, in the second year every 6 months, and thereafter once a year. OS of follow-up was calculated from the day of enrollment to the day of patient's death. Finally, we also recorded the adverse events due to chemoradiation therapy.
Statistical analyses
We calculated the estimated sample size using the per-protocol patient population receiving concurrent chemoradiation, and 78.6% esophagitis reduction from combined modality therapy. Assuming a significance level of 0.05 (2-sided), 48 assessable patients were needed to distinguish a grade 3–5 radiation-induced esophagitis from an alternative rate of 62% 7 with 80% power. We increased the number to 51 patients to allow for a 6% patient loss. Statistical analyses were executed using SPSS statistical software, version 19.0. Paired t-test was used for determining the differences in RTOG score and NRS score of each patient.
Dependent variables were analyzed for correlation using the Spearman rank correlation test. Differences in numerical data were analyzed using the chi-square test, Fisher's test, or t-test. The Kaplan and Meier method was used to estimate survival, comparisons were made by the log-rank test, and differences were tested by the Mantel–Cox log-rank test. A two-sided confidence interval of 95% was applied for determining significance for all the statistical tests.
Results
A total of 51 patients admitted to our research center from 2014 to 2016 were included in this study. Twenty-two patients received concurrent chemoradiation therapy, and 29 patients received definitive radiation therapy. Fourteen patients were treated with docetaxel plus cisplatin and eight patients were treated with fluorouracil and cisplatin. The patients in the concurrent chemoradiation therapy were treated with chemotherapy one cycle per 3 weeks for 2–3 cycles. The clinicopathological details of this patient population are summarized in Table 1.
Clinical Characteristics of the Patient
CRT, chemoradiation therapy; ECOG, Eastern Cooperative Oncology Group.
The earliest appearance of ARIE among our sample was 2 weeks after initiating radiation therapy, with a median of 3 weeks (range, 2–4 weeks). A median dose of 25.8 Gy (range, 14.4–40 Gy) was associated with the development of ARIE. The RTOG scores in EGCG-prescribed patients were significantly lower compared with baseline (details in Table 2). The mean scores of all patients at each week are shown in Figure 1. In the patients enrolled in this trial treated with chemoradiation therapy or definitively radiation therapy, there was no recorded grade 3–4 esophagitis or esophageal stricture. Therefore, no nasogastric tubes or parenteral nutrition was required for these patients.
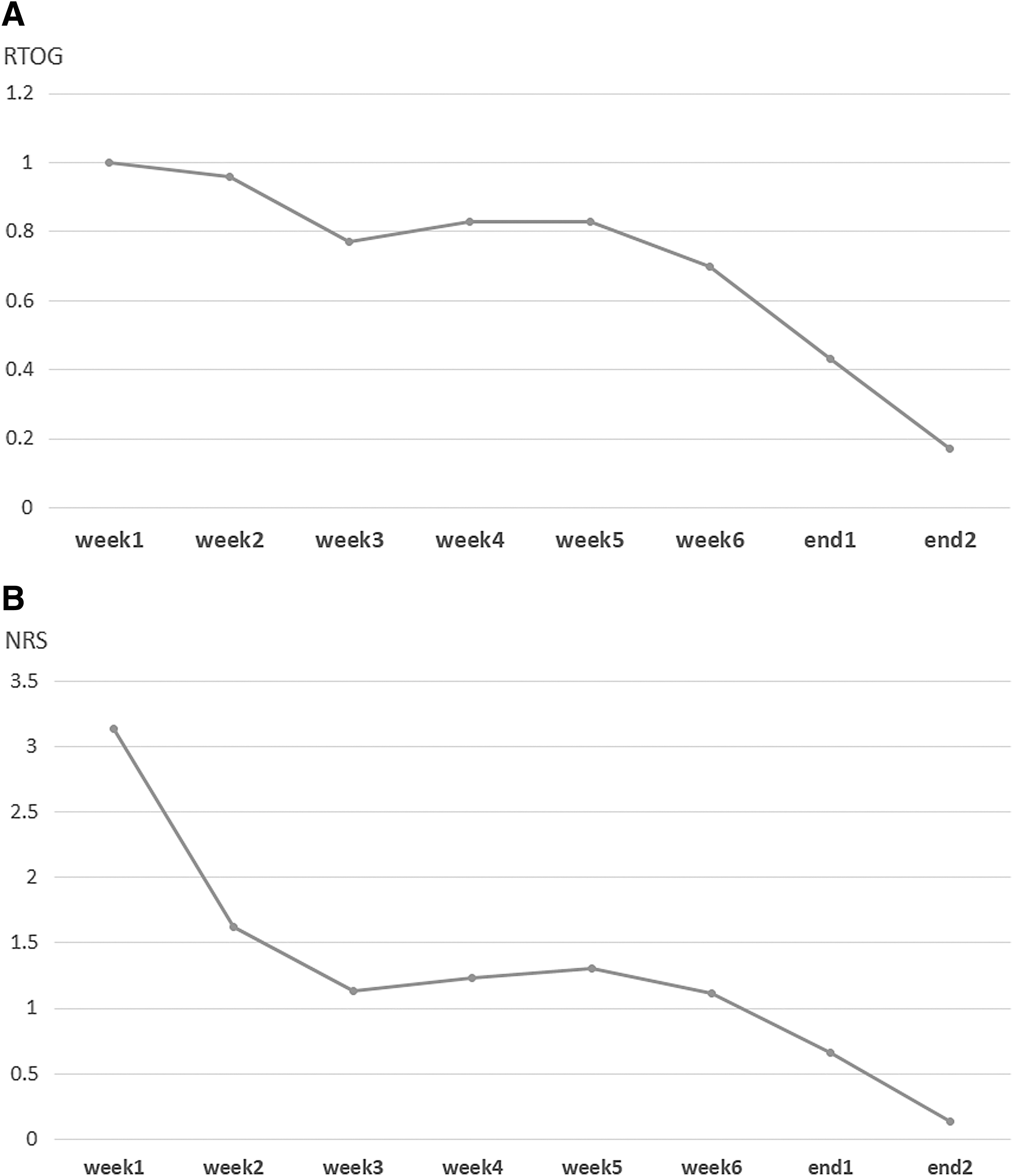
Relief of Pain Score (Numerical Rating Scale) in Every Week
w1 means the week when we observed the grade 1 RTOG score, the EGCG solution was given to the patient. The time point was set as baseline. w2 means the second week after prescribing the EGCG to the patient. w3 means the third week as the same. And so on.
No. of patients means the number of patients whose pain score decreased. The number of patients recorded every week is different because the starting time of EGCG is different.
wend1 means 1 week after end of the treatment. wend2 means 2 weeks after end of the treatment.
Mean changes: the decrease of the mean pain score of this week for all patients compared with baseline (week 1; w1).
EGCG, epigallocatechin-3-gallate; RTOG, Radiation Therapy Oncology Group.
At the point of 1 week after radiation therapy, 27 of 47 patients (two patients stopped radiation therapy and EGCG because of pneumonia and esophageal fistula; two patients stopped EGCG because of nausea and heartburn) had NRS scores that decreased to grade 0, there was a persistence of grade 1 esophagitis in 11 patients. No significant increase in NRS score was observed after cessation of treatment.
EGCG was well tolerated in most patients. EGCG for one patient was discontinued after 1 week due to grade 2 nausea persisting for a week until usage of tropisetron. Another patient had grade 1 heartburn and quit the trial after using EGCG for 1 week; proton pump inhibitors were subsequently prescribed. Finally, another patient had grade 2 stomach upset and discontinued further medications after 1 week. None of these patients stopped radiation therapy due to side effects from EGCG. In our research, the allergic reaction related to EGCG was not observed during and after the treatment.
Two of 51 patients did not receive complete dose of radiation therapy due to pneumonia and esophageal fistula. Of the 51 patients evaluated for efficacy, 44 had a clinical response (10 CRs and 34 PRs), yielding a clinical response rate of 86.3%. Three patients developed PD and four others were evaluated as SD. Adverse events due to chemoradiation or definitive radiation therapy are summarized in Table 3.
Adverse Events, from the Beginning of Chemoradiation or Definitive Radiation Therapy to the 2 Weeks After the Treatment
The follow-up time had a median value of 34.6 months and a range of 1.5–70.33 months. The total OS had an OS range of 1.5–69 months with a median of 31 months.
Three patients were assessed as PD and two of them died during the period of scheduled follow-up visits. Twelve patients died due to esophageal fistula, pneumonia, or tumor progression. The OS rate was 74.5%, 58%, and 40.5% for 1, 2, and 3 years (Fig. 2). The flow chart of the patients' enrollment in this study is shown in Figure 3.
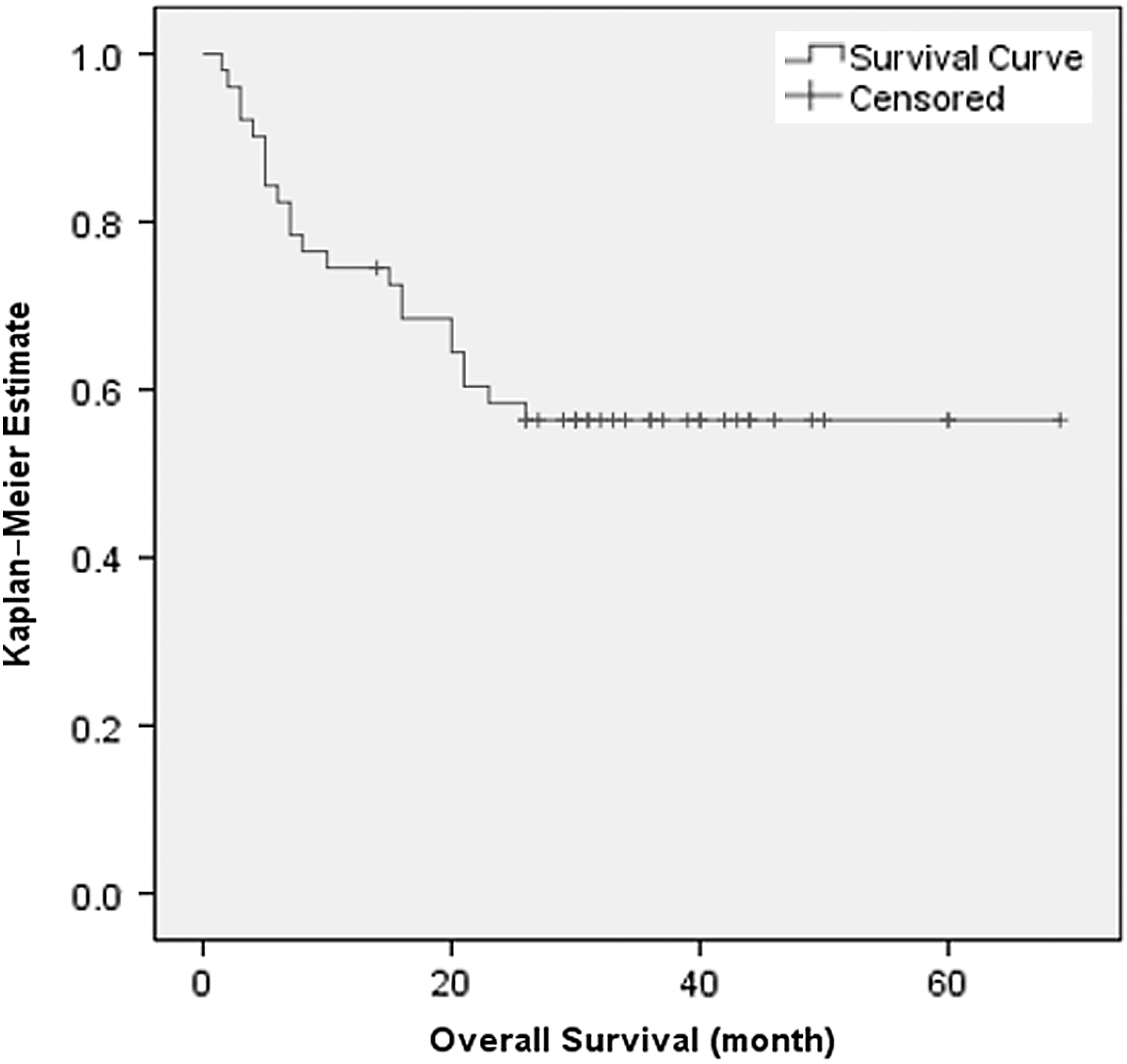
Kaplan–Meier overall survival curves for the entire cohort of patients.
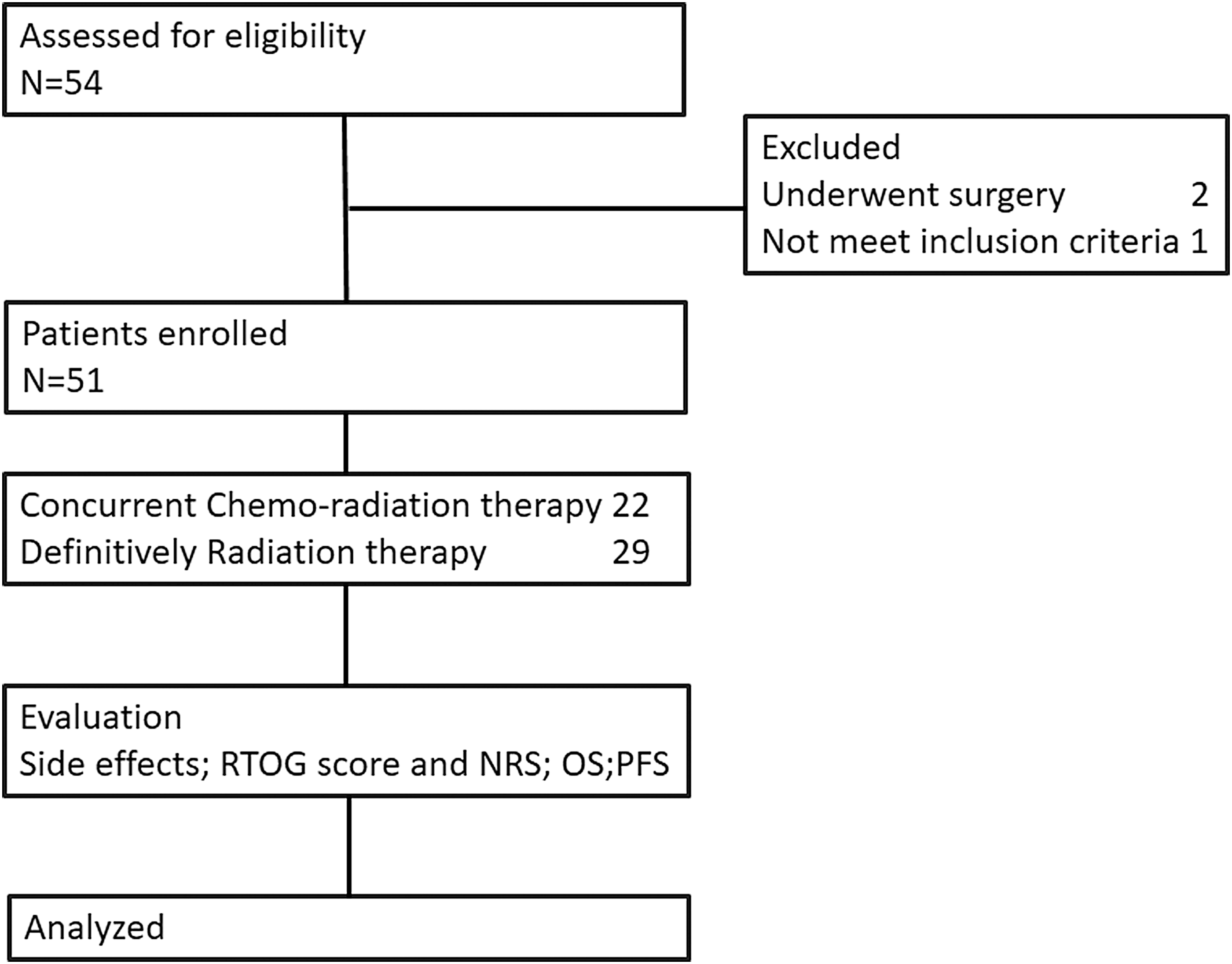
Flow chart of patients' enrollment in this study.
Discussion
The rate of ARIE in ESCC patients with chemoradiation therapy was 100% in the research published in 2010. 14 Although advanced techniques such as 3D conformal radiotherapy and IMRT have allowed increased dosing of targets and decrease treatment-associated toxicity in radiation oncology, 5 ARIE still remains a common toxicity associated with chemoradiation and definitive radiation therapy. The total esophagitis rate was 91.7% in Zhao's research, which was published in 2019. 15 While weight loss is the most common outcome of severe ARIE, 5 if acute esophagitis leads to an interruption of the radiotherapy treatment, this treatment advantage may disappear.
Amifostine (WR-1035) is an organic thiophosphate administered intravenously or subcutaneously. Neutralization of free radicals after exposure to ionizing radiation or some cytotoxic agents limits DNA damage and blocks the regulation of the inflammatory signals. However, several publications have reported contradictory results of reducing mucositis followed by potential side effects. 7,16 –18 No effective method for ARIE and, to our knowledge, no formal prospective or retrospective studies comparing reducing ARIE and treatment outcomes of ESCC patients with chemoradiotherapy regimens have been performed.
Our previous phase I study enrolled lung cancer patients treated with standard chemoradiation therapy. EGCG solution was prescribed after the development of grade 2 ARIE and a safe and effective dose of EGCG was determined through a dose/escalation study. Results showed that none of the EGCG dosed groups had dose-limiting toxicities. A significant decrease in ARIE to grade 0/1 was observed in most patients after EGCG administration. NRS was also significantly lower in most patients. 8 Therefore, we concluded that EGCG was a safe and effective treatment for ARIE. Therefore, we continued this current phase II trial in patients with esophageal cancer.
In our trial, during the radiation therapy, all the RTOG scores and NRS scores were recorded once the ARIE appeared. The ARIE and pain score were all reduced compared with baseline. What is more, ARIE exhibited significant declines after EGCG treatment, which was inspiring and exciting in patients during radiation therapy.
There is potential for concern about the impact of EGCG on the treatment of cancer. However, EGCG might also have anticancer effects, which is known for its antiangiogenic properties, 19,20 arrest of cell cycle, 21 –23 modulation of folate metabolism, 24 prevention of DNA damage, 25 inhibition of telomerase activity, 26,27 downregulation of antiapoptotic factors, 28 and induction of reactive oxygen species generation. 29 These properties of green tea extracts are possible mechanisms by which EGCG may impart anticancer properties. Phase I and II trials involving oral polyphenon E against stage 0 to II chronic lymphocytic leukemia (CLL) indicated that EGCG is safe and effective for reducing lymphadenopathy in CLL patients. 10,30
In our study, the clinical response rate was lower than 97.7% observed in another multicenter research involving ESCC conducted at our center. 31 The rate was still a little lower than 94% found in other studies of patients with stage II–III esophageal cancer undergoing chemoradiotherapy. 32 That might be because not all patients received concurrent chemoradiation therapy. Contrary to that study, we observed a median OS of 31 months, which is higher than 13 and 26 months in the previous study. Remarkably, in the RTOG 8501 trial, they enrolled patients who received chemoradiation or radiation therapy alone. The 5-year OS rates were 26% and 0%, respectively, and 14% for nonrandomized patients. 33
The results of this trial indicated that EGCG mediated an increase in the response rate against ARIE and was a safe treatment. Compared with previous studies, this response rate is high in our study and the OS is similar to the results of previous studies. However, two patients did not respond to treatment possibly due to high doses of radiation and chemotherapy, but the detailed mechanisms were unknown. EGCG may protect patients from developing severe side effects that would cause an interruption in radiotherapy regimens, thus leading to better tumor control and quality of life postradiotherapy. In this way, EGCG may therefore positively influence the survival rate.
This study has a few limitations that should be noted. First, the number of patients in this study is limited and this study did not have a control group. Finally, the enrollment period was almost 2 years long, which is not ideal. Thus, a randomized trial with a control group is needed for further evaluation of EGCG.
Based on the clinical results of this trial, oral administration of EGCG solution seems to be feasible for treating ARIE in patients with esophageal cancer who received radiation therapy. EGCG might also be a protective intervention against other radiation treatment hazards without compromising the efficacy of radiotherapy. A randomized study with a control group is needed for further evaluation of this promising compound.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (grant no. 81502667), the Shandong Provincial Natural Science Foundation (ZR2015HZ004; ZR2016HM35), and the Key Research and Development Plan of Shandong Province (grant nos. 2016GSF201167; 2018GSF118232; ZR2014HP041).