
Abstract
Since ancient times, licorice, the root of Glycyrrhiza glabra, has been known to have a wide spectrum of therapeutic effects. Glycyrrhizin is cleaved to glycyrrhizic acid, which is subsequently converted to glycyrrhetic acid by human intestinal microflora. Glycyrrhetic acid is a potent inhibitor of 11β-hydroxysteroid dehydrogenase (11β-HSD) and performs a range of corticosteroid-like activities. The pharmacologic effects of licorice contribute to its anti-inflammatory, antioxidative, anti-allergenic, and antimicrobial properties. Licorice has been used to treat liver disease, gastrointestinal disorders, oral disease, and various skin disorders and has been used in gum, candy, herbs, alcoholic beverages, and food supplements. Licorice and its extracts, especially glycyrrhizin, can be taken orally, through the skin (in the form of gels and oils), and intravenously. Licorice demonstrates mineralocorticoid-like activity not only by inhibiting 11β-HSD2, but also by binding to a mineralocorticoid receptor, leading to potentially adverse risks of mineralocorticoid-like overactivity. Chronic use of licorice can lead to hypokalemia and hypertension, and some people are more sensitive to licorice exposure. Based on clinical trials, this review summarizes the positive effects of licorice and other reported side effects.
Introduction
Licorice, the root of Glycyrrhiza glabra, contains glycyrrhizin as a major ingredient. This ingredient has been used as a traditional herbal medicine in Asian countries and as a sweetener and flavor in candies, foods, and drinks in the United States and Europe. 1,2 Glycyrrhizin is used as an efficient natural sweetener because it is 50–100 times sweeter than sucrose and has a slow sweetness onset. 3 In addition to its use as a sweetener, glycyrrhizin has been used in various therapeutic applications dating back to ancient times. 2
The pharmacological effects of licorice are attributed to its various metabolites including glycyrrhizic acid and glycyrrihetic acid (glycyrrhetinic acid). 4 Glycyrrhizic acid is converted to glycyrrhetic acid, a triterpenoid aglycone conjugated to glucuronide and sulfate, which is 200–1000 times a more potent inhibitor of 11β-hydroxysteroid dehydrogenase (11β-HSD) than glycyrrhizic acid and has a range of corticosteroid-like activities. 5 Numerous clinical studies have highlighted scientific evidence related to the pharmacological properties of licorice including hepatoprotective, 6,7 anti-inflammatory, 7 –9 antiviral, 6 anti-ulcer, 10 and immunoregulatory effects. 9
The general belief, however, is that licorice is a healthy natural herb without any serious adverse effects. This belief may lead to overconsumption or a misuse of glycyrrhizin, which could ultimately be hazardous. Other than glucocorticoid-like activity, licorice also has a potential risk of mineralocorticoid-like overactivity by not only blocking 11β-HSD, but also by directly binding to mineralocorticoid receptors (MRs). 11 Thus, continuous high-dose exposure to glycyrrhizin may result in a state of mineralocorticoid excess and secondary suppression of the renin–angiotensin–aldosterone system. 12 This exposure could induce hypokalemia, metabolic alkalosis, cardiac arrhythmia, edema, hypertension, and other adverse effects related to its mineralocorticoid-like activity. 13
This clinical review aims to summarize the therapeutic effects, potential adverse risks, and the putative biological mechanisms of licorice as determined from human clinical trial data.
Glycyrrhizin Pharmacokinetics, Pharmacology, and Toxicology
Pharmacokinetics of glycyrrhizin
The absorption, distribution, metabolism, and elimination of glycyrrhizin are summarized in Figure 1. After oral ingestion, glycyrrhizin is cleaved to glycyrrhizic acid and subsequently converted to glycyrrhetic acid (glycyrrhetinic acid) by human intestinal microflora. Glycyrrhetic acid is 200–1000 times a more potent inhibitor of 11β-HSD than glycyrrhizic acid. 14 It is absorbed through the intestine, transported to the liver, metabolized into glucuronide and sulfate conjugates through phase II biotransformation, and excreted to the biliary system. 15
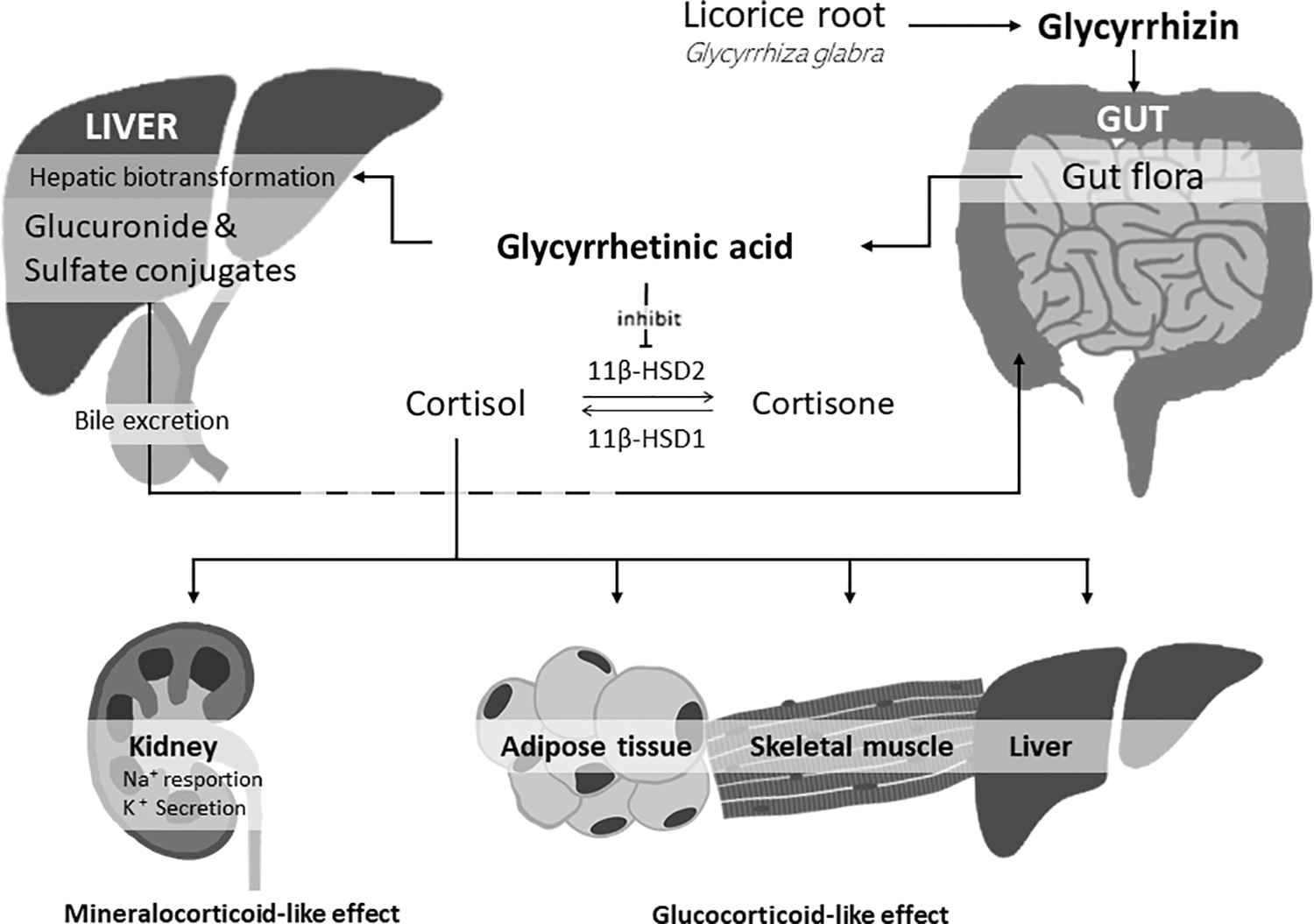
Metabolism and elimination of glycyrrhetic acid. 11β-HSD, 11β-hydroxysteroid dehydrogenase; K+, potassium; Na+, sodium.
Pharmacology and toxicology of glycyrrhizin
The active metabolites in licorice extract are glycyrrhizic acid and glycyrrhetic acid. Glycyrrhetic acid is the more potent metabolite, with corticosteroid-like properties. There are two stereoisomers of glycyrrhetic acid, 18α-glycyrrhetinic acid and 18β-glycyrrhetinic acid. 4 These two stereoisomers have different bioactivities: 18α-glycyrrhetinic acid selectively inhibits the 11β-HSD1 enzyme, but not 11β-HSD2, whereas 18β-glycyrrhetinic acid inhibits both the 11β-HSD1 and the 11β-HSD2 enzymes. 16 The two 11β-HSD isozymes catalyze the interconversion between cortisol and cortisone. The enzyme 11β-HSD1 converts inactive cortisone into active cortisol in glucocorticoid target tissues such as adipose tissue, skeletal muscle, and liver. 11β-HSD1 regulates the tissue-specific effects of circulating glucocorticoid. 16 Thus, 11β-HSD1 inhibition by glycyrrhetic acid could ameliorate insulin resistance and type 2 diabetes. 16 The enzyme 11β-HSD2 follows two major physiologic paths. First, the enzyme converts active cortisol into inactive cortisone. Second, it plays a role in preventing overstimulation of mineralocorticoid tissue by cortisol. Of interest, only the 11β-HSD2 isomer protects the MR, so an 11β-HSD1-deficient mouse does not have elevated mineralocorticoid level. 17 Thus, glycyrrhetic acid could enhance the glucocorticoid-like effects in addition to presenting a potential risk of mineralocorticoid-like overactivity. 5
The major pharmacological mechanisms of glucocorticoid are broadly classified into immunological and metabolic effects. Glycyrrhetic acid is more likely to affect immunological responses. 18 Glycyrrhizin acts as an immunoregulator by inhibiting the activation of T cells and cytokines. 19 For unresponsive patients or those with intolerance or absolute contraindication to standard therapy, licorice could be considered as an alternative therapeutic strategy. 20 Many studies have been conducted to determine the effects of glycyrrhizin on the underlying inflammation or autoimmune mechanisms of various skin diseases. Licorice has an antiviral effect by enhancing T cell-mediated immunity through the regulation of T cell cytotoxicity, interferon-γ (IFN-γ), and interleukin (IL)-12. 19 Licorice also exhibits antibacterial effects against Helicobacter pylori and Streptococci mutans, which may increase the eradication rate of H. pylori and decrease dental decay. 21,22 In addition, carbenoxolone, a glycyrrhetic acid derivative, can be used as a mucosal protective agent to help heal peptic ulcers and oral mucosal ulcers. 10
From a metabolic perspective, the active form of glycyrrhizin, glycyrrhetic acid, regulates energy metabolism and fat distribution by inhibiting the 11β-HSD1 enzyme at the adipocyte level. The underlying mechanism is the regulation of the expression of genes related to fatty acid oxidation and food cravings, which may influence metabolism and body composition. 23 –25
The toxicological effects associated with licorice use arise from the inhibition of the enzyme 11β-HSD2. Glycyrrhetic acid also inhibits hepatic metabolism of aldosterone through suppression of 5-β reductase activity, which leads to an excess of mineraloocorticoids. 26 In this regard, licorice also exerts a mineralocorticoid-like effect on the kidney both directly and indirectly by increasing the effect of aldosterone. 27 High doses of glycyrrhizin and large amounts of licorice consumption, however, decreased 11β-HSD2 activity and led to elevated blood pressure thorough cortisol overstimulation of the MR. 28 Excess mineralocorticoid stimulates sodium (Na+) reabsorption and potassium (K+) excretion, leading to increased Na+ retention and hypokalemia.
Clinical Implications of Glycyrrhizin
Previous clinical studies have focused on the pharmacological effects of glycyrrhizin on liver disorders (nonalcoholic fatty liver diseases [NAFLD], hepatitis B, and hepatitis C), gastrointestinal disorders (H. pylori and peptic ulcer), oral disorders (oral ulcer, dental caries, and xerostomia), skin disorders (erythema, atopic dermatitis, vitiligo, and alopecia areata), and metabolic disorders. Table 1 summarizes the various clinical implications of licorice, as well as its derivates and pharmacological activities with underlying action mechanisms.
Clinical Implications of Licorice and Its Derivatives and Putative Biological Mechanisms from Clinical Trials
11β-HSD, 11β-hydroxysteroid dehydrogenase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; NAFLD, nonalcoholic fatty liver diseases.
Effects on liver disorders
Nonalcoholic fatty liver disease
NAFLD is a common and important cause of chronic liver disease. 29 The risk factors for NAFLD include central obesity, type 2 diabetes mellitus, and dyslipidemia. 29 Although modification of these risk factors is generally recommended, there is no proven effective treatment for nonalcoholic steatohepatitis, a progressive type of NAFLD. 7 Sixty-six patients were confirmed to have NAFLD by ultrasonography and the presence of elevated levels of aspartate aminotransferase (AST) and alanine aminotransferase (ALT). 7 The patients were divided into a case (licorice) group and a control group. In the licorice group, the mean values of AST and ALT level decreased significantly from 58.18 to 49.45 (U/L) and from 64.09 to 51.27 (U/L), respectively (all P < .001). There were no statistically significant changes in the control group. Several plausible mechanisms may be offered to explain the improved liver enzyme numbers. The hepatic anti-inflammatory effect of glycyrrhizin may be associated with increased hepatic lymphocyte activation, inhibition of the complement's lytic pathway, and decreased production of IL-10 by liver dendritic cells. 30 –32 Some animal studies support that licorice could improve lipoprotein lipase expression, serum lipids, and insulin sensitivity, which might also improve the degrees of hepatic steatosis and hepatic inflammation. 33,34
Hepatitis B and hepatitis C
Hepatitis B virus and hepatitis C virus (HCV) infections can be associated with progressive liver disease that may lead to cirrhosis, increased risk of hepatocellular carcinoma (HCC), and liver failure. 35,36 Glycyrrhizin had been used intravenously for treatment of Chinese patients with chronic hepatitis B. Concomitant therapy with glycyrrhizin and tenofovir significantly improved serum transaminases compared with tenofovir alone. 20 Although peginterferon plus ribavirin is the only treatment with proven efficacy in patients with chronic HCV infection, sustained virologic response is achieved in only ∼50% of the patients. 37 For those not responding or patients with absolute contraindication to standard therapy, alternative therapeutic strategies have to be developed. In this regard, a number of clinical trials have been examined to evaluate the effect of glycyrrhizin on chronic HCV infection. A long-term use of glycyrrhizin in patients with chronic hepatitis C was effective in preventing the development of HCC. 38 Moreover, restorative effects on AST and ALT activities after administration of glycyrrhizin for 2 weeks were reported in both human and rat studies. 6 From a double-blind, randomized trial evaluating the effect of glycyrrhizin on serum ALT and HCV-RNA levels in European patients, glycyrrhizin lowered serum ALT by 26% at the end of active treatment, which was significantly higher compared with the placebo group (6%). 39 However, the positive effect of glycyrrhizin was not found in HCV-RNA expression levels. 39 In another study, van Rossum et al. reported that 10% (4 of 41) and 20% (3 of 15) of the patients reached normal ALT levels in the three-times-per-week and six-times-per-week treatment groups, respectively. 40 Although the underlying mechanism of its antiviral effect is not fully understood, one of the proposed mechanisms is that glycyrrhizin reduces serum ALT through hepatocyte membrane stabilization. 41 Both suppression and increase in T cell cytotoxicity have been reported and also stimulation of the endogenous production of IFNs. IFN-γ and IL-12 are Th1-type cytokines and are important in T cell-mediated immunity and viral clearance. 19 Furthermore, a retrospective study conducted in Japan showed that long-term glycyrrhizin injection therapy decreases HCC rate in patients with IFN-resistant HCV-related chronic hepatitis and cirrhosis. 42
Effects on gastrointestinal disorders
Helicobacter pylori
The most common cause of peptic ulcers is H. pylori infection. If it is not eradicated after discontinuing treatment, the recurrence rate is reported to be 50–80% between 6 and 12 months. 21 Recently, antibiotic resistance to H. pylori has gradually increased, limiting the effectiveness of standard therapy for H. pylori infection. 43 Hajiaghamohammadi et al. found that the addition of licorice to the standard clarithromycin-based triple regimen for treating H. pylori infection increased the eradication rate in patients with peptic ulcer dyspepsia. 21 The positive therapeutic response was 83.3% in the licorice group compared with 62.5% in the control group (P = .018). Licorice exhibits antibacterial and anti-adhesive effects against H. pylori by blocking the dihydrofolate reductase enzyme and inhibiting DNA gyrase, a crucial enzyme for bacterial replication and transcription. 44 The polysaccharide released from licorice root also inhibits H. pylori adhesion to the human gastric mucosa. 45
Peptic ulcer (gastric/duodenal ulcer)
The therapeutic effects of licorice on peptic ulcers were found to be related to the pharmacological activity of carbenoxolone, a synthesized metabolite from glycyrrhetic acid. 10 The first controlled clinical trial to demonstrate the efficacy of carbenoxolone in healing gastric ulcerations was conducted by Doll and Hill. 46 Of the 30 patients treated with carbenoxolone, 11 showed complete healing of gastric ulcers, whereas only 1 of the 20 control subjects showed complete healing. Since then, many clinical trials for peptic ulcers have been conducted, and a growing body of subsequent studies has generally shown similar positive findings. 47 –50 However, seven clinical trials administrating licorice or carbenoxolone in patients with gastric or duodenal ulcer did not show significant differences between the treatment and placebo groups by clinical and radiological assessment. 51 –57
The following pharmacological mechanisms could explain how glycyrrhizin is involved in the peptic ulcer healing process. First, carbenoxolone, a glycyrrhetic acid derivative, is rapidly absorbed from the stomach, excreted in the bile, and reabsorbed in the small bowel. When carbenoxolone passes through the gastric mucosa, it interacts with a number of proteins within the cells, including functional proteins such as the nuclear histones, which regulate the metabolic activity of the cells and the synthesis of glycoprotein. 10 Second, carbenoxolone also extends the life span of gastric epithelial cells and stimulates the prolongation period for glycoprotein synthesis and secretion. 58 Increased production of gastric mucus plays a key role in promoting ulcer healing. Third, carbenoxolone inhibits the reverse diffusion of bile-derived hydrogen ions and possibly inhibits peptic activity. 10 The anti-ulcer effects of licorice are also owing to inhibition of 15-hydroxyprostaglandin dehydrogenase and delta13-prostaglandin reductase. 59
Effects on oral health disorders
Oral cavity ulcer
As mentioned previously, licorice is a potent mucosal agent used effectively in the treatment of peptic ulcers. Ghalayani et al. reported that licorice mucoadhesive films were effective in treating oral mucositis for patients undergoing postoperative adjuvant or definitive radiotherapy. 8 The mean values of pain score and mucositis scale assessed by Friedman's test showed a significant improvement (both P < .05) over four consecutive weeks. Although further evaluation over a longer period is required, licorice mucoadhesive films may be considered for pain relief in patients with oral ulcerations. 8
Dental caries
Dental caries is one of the most common health problems in childhood. 60 Nearly 60% of children in the United States between the ages of 5 and 17 suffer from some type of corrupted, decayed, or missing permanent teeth. 60 In this regard, various methods for preventing and reducing dental caries are necessary, and the use of licorice extract has emerged as one promising intervention. 61,62 S. mutans is an important factor in the development of dental caries and disease progression. 63 Almaz et al. conducted a randomized control study to evaluate the efficacy of herbal lollipops made from licorice on salivary S. mutans. 22 This study was conducted using three groups of children aged 5–11 years: a caries-free group (group 1), a high-caries risk group whose dental treatment was complete (group 2), and a high-caries risk group who had not complied with dental treatment (group 3). Each group was divided into a placebo lollipop group and a herbal (licorice) lollipop group. Children assigned to group 3 showed significant reduction (P = .014) in salivary S. mutans level after lollipop use. The potential mechanisms that explain the efficacy of herbal lollipops (licorice) are inhibition of bacterial glucosyltransferase activity, 12,64,65 antibacterial activity against cariogenic bacteria S. mutans and Streptococci sobrinus, and periodontal pathogens Porphyromonas gingivalis and Prevotella intermedia 66,67 increasing salivary flow to act as a gustatory stimulus. 68
Xerostomia
Dry mouth (xerostomia) is a common symptom in hemodialysis patients. It not only affects oral health, but also the quality of life for patients undergoing hemodialysis. 69,70 Yu et al. compared the mouthwash intervention effect of pure water and licorice in hemodialysis patients. 71 The licorice mouthwash was effective in increasing salivary flow rate and relieving mouth dryness. Although both intervention groups showed improvement in salivary flow, the subjective feeling of mouth dryness was significantly improved only for the licorice mouthwash group (P < .001). Perception of sweetness of licorice may improve the secretion of saliva and symptoms of dry mouth by stimulating the taste receptors. 71
Effects on metabolism and body composition
Licorice flavonoid oil (LFO) has been reported to have beneficial effects on obesity and insulin resistance. Tominaga et al. 72 reported that overweight postmenopausal women who took 900 mg/day of LFO showed significantly decreased visceral fat, body mass index, and low-density lipoprotein cholesterol. The beneficial effects of licorice on body composition changes have also been reported in normal body weight individuals. Armanini et al. 23 found that a dose of 3.5 g/day of licorice resulted in reduced body fat mass in healthy, normal weight people without significant changes in body mass index. The topical application of licorice also has advantages as it was shown to diminish subcutaneous thigh fat. 24 These studies suggest that licorice has an effect on fat distribution and fat oxidation. A recent clinical trial showed that LFO consumption affected metabolism by decreasing respiratory exchange rate and increasing fat oxidation in 34 healthy women. 73 In another double-blind, randomized trial, LFO administration had favorable effects on body composition with a decrease of body fat mass and increase of muscle mass in adults 54–90 years of age who underwent rehabilitation treatment for knee osteoarthritis. 74
There are several possible mechanisms that explain this redistribution of body composition. First, the active form of glycyrrhizin, glycyrrhetic acid, regulates energy metabolism and fat distribution by inhibiting the 11β-HSD1 enzyme at the adipocyte level. 23,24,73 Second, licorice influences the gene expression of enzymes related to the fatty acid oxidative pathway in the liver. 73,75 Third, licorice is known to suppress food cravings. 25 A recent meta-analysis including 26 clinical trials in human have demonstrated that licorice consumption reduced body weight (weighted mean differences [WMDs] = −0.433 kg; 95% CI [confidence interval] = −0.683 to −0.183), and body mass index (WMD = −0.150 kg/m2; 95% CI = −0.241 to −0.058). 76
Effects on skin disorders
Erythema
As glycyrrhizin has been shown to have various pharmacological effects such as anti-inflammatory, anti-immune-mediated cytotoxicity, and anti-allergenic activities, many studies have been conducted to determine the effect of glycyrrhizin on the underlying inflammation of various skin diseases. Kolbe et al. reported that applying a topical gel with licochalcone A, another natural phenol derivative of glycyrrhizin, significantly reduced erythema induced by shaving and ultraviolet (UV) light. 77 In another study conducted by Weber et al., licochalcone A showed significantly improved average erythema scores and quality-of-life scores as assessed by questionnaires. 78 The anti-inflammatory mechanism of licochalcone A was also demonstrated by an in vitro study conducted by Sulzberger et al. 79 Licochalcone A stimulation significantly reduced prostaglandin E2, a proinflammatory mediator, and reduced tumor necrosis factor-α-induced nuclear factor κB activation. 79
Atopic dermatitis
Glycyrrhizin has been reported to relieve immunoglobulin E-induced type 1 allergic diseases such as allergic dermatitis. 9 Saeedi et al. reported that licorice gel dose-dependently reduced erythema score, edema, and itching sense among 90 atopic dermatitis patients (placebo vs. treatment group and 1% vs. 2% licorice gel, all P < .01). 80 The standard treatment for atopic dermatitis is a topical steroid, but some patients are resistant. Glycyrrhizin enhances cortisol's stress reaction inhibition, antibody formation, and inflammation. 80 Thus, glycyrrhizin has the potential to be used more widely as a treatment for atopic dermatitis because it has similar actions to steroids, but with relatively few side effects.
Vitiligo
Vitiligo is a common, idiopathic-acquired depigmentation disorder. As a treatment option for active stage vitiligo, narrow-band UVB light therapy and oral cortisone or methotrexate have been considered. However, some patients or children may experience side effects from those treatment modalities. 81 Mou et al. compared the effects of treatment with glycyrrhizin alone, UVB alone, and combination therapy of glycyrrhizin and UVB on active stage vitiligo. 82 In this study, all three treatments showed positive results, with the combination therapy of glycyrrhizin and UVB being the most effective. Although vitiligo's pathogenesis is not yet clear, it is believed to be the result of genetic susceptibility triggered by similar environmental factors as those that trigger autoimmune diseases. A more recent study has shown that patients with vitiligo have inflammation in the dermis and express the IL-1β and IL-18 enzymes at high levels. 83 Glycyrrhizin can regulate T cell activation and inhibit inflammatory cascades. 82 Thus, the anti-inflammatory effect of glycyrrhizin may explain its effect on improving vitiligo.
Alopecia areata
The cause of alopecia areata is not clear yet, but recent studies have suggested that is a T cell-mediated autoimmune disease. 84 In histological examinations, infiltration of a large number of T lymphocytes around affected follicles has been found. 85 Glycyrrhizin acts as an immunoregulator by inhibiting the activation of T cells and cytokines generated by CD4+ and CD8+ T cells. 86 A Chinese study including children (2–14 years of age) found that both glycyrrhizin tablets plus total glucosides of paeony capsule and glycyrrhizin tablets only were effective for treatment of alopecia areata. 87 Another Chinese study also found that glycyrrhizin compound with topical 2% minoxidil was effective for treatment of alopecia areata. 88
Potential Glycyrrhizin-Related Complications
Physiologically, the 11β-HSD2 enzyme prevents cortisol from binding to the MR by changing it to inactive cortisone. 89 Glycyrrhizic acid increases cortisol level by inhibiting the 11β-HSD2 enzyme. Licorice-induced pseudoaldosteronism is characterized by hypokalemia, metabolic alkalosis, cardiac arrhythmia, edema, and hypertension. Low levels of plasma renin activity and aldosterone were seen among individuals receiving high doses of glycyrrhizin-based pharmaceuticals or consuming large amounts of licorice-containing health products over a prolonged period. Leskinen et al. 90 reported that 2 weeks of licorice intake increased extracellular volume and elevated systolic blood pressure (SBP) and diastolic blood pressure (DBP). Hautaniemi et al. 91 showed that licorice consumption lead to elevated blood pressure by increasing extracellular fluid volume and large artery stiffness. A recent meta-analysis of 18 studies (n = 337) revealed that chronic licorice intake increases blood pressure (5.45 mmHg for SBP and 3.19 mmHg for DBP) and decreases serum potassium level. 27 As described earlier, the active form of glycyrrhizin, glycyrrhetinic acid, has a mineralocorticoid-like effect, which can exert a direct effect on the kidney or indirectly increase the effect of aldosterone. 27 Consequently, K+ excretion is elevated after enhanced Na+ resorption in the distal tubules, leading to hypokalemia and water retention. Thus, careful monitoring of blood potassium levels and electrocardiography are important because of the possibility of cardiac arrhythmias and prolonged QT intervals associated with severe hypokalemia in the high-risk group. Rare but possible adverse effects of licorice are rhabdomyolysis, acute tubular necrosis, asthenia, and muscle cramps. 5
Conclusion
In conclusion, the therapeutic effects of licorice on liver, gastrointestinal, oral, skin and metabolic disorders were found in a growing body of clinical trials, implying that licorice could have various therapeutic properties through its anti-inflammatory, antioxidant, and immunomodulatory properties. However, licorice and glycyrrhizin should be used with caution, and their side effects must be taken into consideration especially in hypertensive patients. Potential limitations of this study are as follows. This review could not uncover all the possible therapeutic mechanisms of licorice. Another limitation is that we only evaluated studies written in English with summaries and abstracts. Future extended reviews including clinical trials in the area of complementary and alternative medicines worldwide are warranted.
Footnotes
Authors' Contributions
Y.J.K. and Y.J.L. developed the idea, designed the research, and developed the search strategy. Y.J.K. and D.H.S. selected, included, and extracted studies. Y.J.K., D.H.S., T.H.C., and Y.J.L. interpreted the analysis and drafted the final review. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a grant from the Korea Society of Dietary Therapy for Cancer and Chronic Disease.