
Abstract
It can be difficult to identify health/functional foods that exert therapeutic benefits for alleviating gingivitis and periodontitis. Recently, extracts of Boesenbergia pandurata (Roxb.), which is a tropical plant, have shown promising inhibitory activity against lipopolysaccharide-induced periodontitis. As a result, a clinical trial is being planned to assess utility of B. pandurata (Roxb.) extracts for promoting oral health; this study was designed to determine an appropriate human dose of the extracts for the trial. Pharmacokinetic studies of panduratin A, which is an active substance in fingerroot, were carried out in mice, rats, and dogs after oral administration of the extracts. The clearance data for each species were used to estimate clearance in humans through allometric scaling based on the maximum lifespan potential, and a daily dose providing sufficient anti-periodontitis activity was estimated for use in the clinical trial. The findings indicated that allometric scaling is a reasonable approach that is relatively free of safety issues and can be used to determine doses of substances for incorporation into health/functional foods appropriate for humans.
Introduction
Boesenbergia pandurata (Roxb.) is a tropical plant that belongs to the Zingiberaceae family. The rhizome of this plant is commonly referred to as fingerroot because it has a shape akin to human fingers (Fig. 1). It has been traditionally used as both a food ingredient and a folk medicine for the treatment of colic diseases in Thailand, Myanmar, China, and Korea. A variety of pharmacological activities exerted by fingerroot extracts have been reported, including anti-mutagenic, 1 anti-inflammatory, 2 –4 antibacterial, 5,6 antiviral, 7 antioxidant, 8 and anti-obesity effects. 9 In 2012, fingerroot extracts were approved as a health/functional food by the Ministry Food and Drug Safety of Korea (No.2012–36) and were indicated for use as a dietary supplement, a skin moisturizing ingredient, and for protection of skin against ultraviolet (UV) exposure. 10

Fingerroot and panduratin A.
Although many studies have investigated the biological functions of these extracts, only a single pharmacokinetic (rat) study of a marker substance in the extracts, panduratin A, 11 has been reported. 12 This lack of data is likely because of the fact that food researchers are primarily interested in the pharmacodynamics, rather than pharmacokinetics, of foods. Although the dose–effect relationships of foods are often evaluated, the behaviors of active ingredients in health/functional foods do not appear to be a primary concern; thus, determining appropriate human doses requires experimental testing. For potentially toxic compounds, the human dose of a substance should be selected based on a lack of adverse effects 13 ; a pharmacologically active dose can be used in products, including foods and food-grade resources, if the dose is proven to be safe. Although interspecies differences in biological activities are difficult to determine, the differential pharmacokinetic effects of a substance among animal species, and between animals and humans, must be taken into account. Allometric scaling can be used to adjust for interspecies differences in the pharmacokinetics of a substance. 14
This study aimed to determine a human dose of fingerroot extracts for use as a health/functional food for alleviation of periodontal inflammation. Panduratin A levels were measured in mice, rats, and dogs after the oral administration of standardized fingerroot extracts and the pharmacokinetic effects of the extracts in humans were predicted based on allometric scaling. Finally, a daily dose of fingerroot extracts was suggested for use in a clinical trial, based on its panduratin A content.
Materials and Methods
Materials
The fingerroot extracts were prepared by following a standard operating procedure. 2 In brief, the dried rhizomes of B. pandurata (Roxb.) were ground and then extracted using 95% ethanol over 3 days at room temperature. The filtrates were evaporated and the panduratin A content in the extracts was measured. Flufenamic acid and acetonitrile were purchased from Sigma-Aldrich (St. Louis, MO, USA) and all other chemicals and solvents were of the highest analytical grade available.
Pharmacokinetic study
All the animals were acclimated to the animal facility for 1 week before the experiments. The animal facility was maintained at a temperature of 23°C ± 3°C and a relative humidity of 50% ± 10%, had 10–20 air changes/hour, a light intensity of 150–300 Lux, and a 12-h light/dark cycle. The pharmacokinetic studies were conducted using 30 male ICR mice (28–32 g), five male Sprague-Dawley rats (295–325 g), and five male beagle dogs (8.5–10.5 kg). While a serial blood sampling was available in rats and dogs, only two samplings were allowed in mice to minimize the hemodynamic changes. Therefore, 30 mice were divided into six groups, and each group was randomly allocated for 2 of 12 sampling times. Blood samples were obtained from the retro-orbital plexus of the mice (100 μL; two samples from each mouse) and from the jugular veins of the rats (200 μL) and dogs (200 μL). Twelve samples were serially collected at 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 12, 24, and 36 h after a single oral administration of the fingerroot extracts (200 mg/kg), which were suspended in corn oil. The blood samples were centrifuged at 19,500 g for 10 min and the plasma was separated and stored at −20°C. Plasma concentrations of panduratin A were determined using a validated analytical method. 12 The mouse and rat experiments in this study were approved by the Chung-Ang University Animal Care and Use Committee (2016-00088; Seoul, Korea) and the dog experiments were approved by the Knotus Co. Animal Care and Use Committee (KNOTUS IACUC 16-KE-212; Kyunggi Province, Korea).
Data analysis and allometric scaling
The time courses of the plasma panduratin A concentrations were used to calculate the pharmacokinetic parameters of the extracts: the peak concentration (C max) and time to C max (T max) were directly obtained from the individual time courses; the elimination rate constant (k) was obtained by linear regression of the log-transformed plasma concentrations in the terminal phase; the area under the plasma concentration time curve (AUCt) was calculated using the trapezoidal rule and the concentration at the last sampling time (C last)/k was added to obtain the AUC to infinite (AUCinf); and clearance was calculated as dose/AUCinf. Naive-pooled analysis was used to obtain the plasma concentration/time profiles in the mice owing to the minimal sampling from each individual as described previously; in brief, five plasma concentrations from five mice were obtained at each sampling time, and their mean values were used to calculate the pharmacokinetic parameters. The standard two-stage method was adapted to obtain the mean values of the pharmacokinetic parameters for the rats and dogs. All data are presented as mean ± standard deviation, except for the mouse data. The pharmacokinetic parameters were statistically compared using Student's t-tests and P < .05 was considered to indicate statistical significance.
The clearance data for panduratin A obtained from the mice, rats, and dogs were used to predict clearance from humans by simple allometric scaling. The equation for calculating clearance is as follows:
where Y is the clearance, BW is the body weight, and log(a) and b are the y-intercept and slope, respectively, of the allometric equation. 14 The total clearance values for mice, rats, and dogs were used to predict clearance in humans. The mean clearance value and mean species weight were plotted using log–log coordinates and a linear relationship was fitted to the log-transformed data to estimate parameters a and b. If necessary, the maximum lifespan potential (MLP) and brain weight were incorporated into the equations, depending on the value of the clearance slope derived by simple allometry. The total clearance estimated by allometric scaling was used to predict the required human dose of panduratin A, which was ultimately used to select a daily dose of the standardized fingerroot extracts, i.e., clearance was multiplied by the AUC at a dose of 100 mg/kg; this represents significant anti-inflammatory activities, as observed in a previous rat model of lipopolysaccharide (LPS)-induced periodontitis. 2
Results
The panduratin A content in the extracts was ∼12% and the dose (200 mg/kg) of the extracts used in this study was equivalent to 24 mg/kg of panduratin A. This dose exerted significant anti-inflammatory activities in a previous rat study. 2
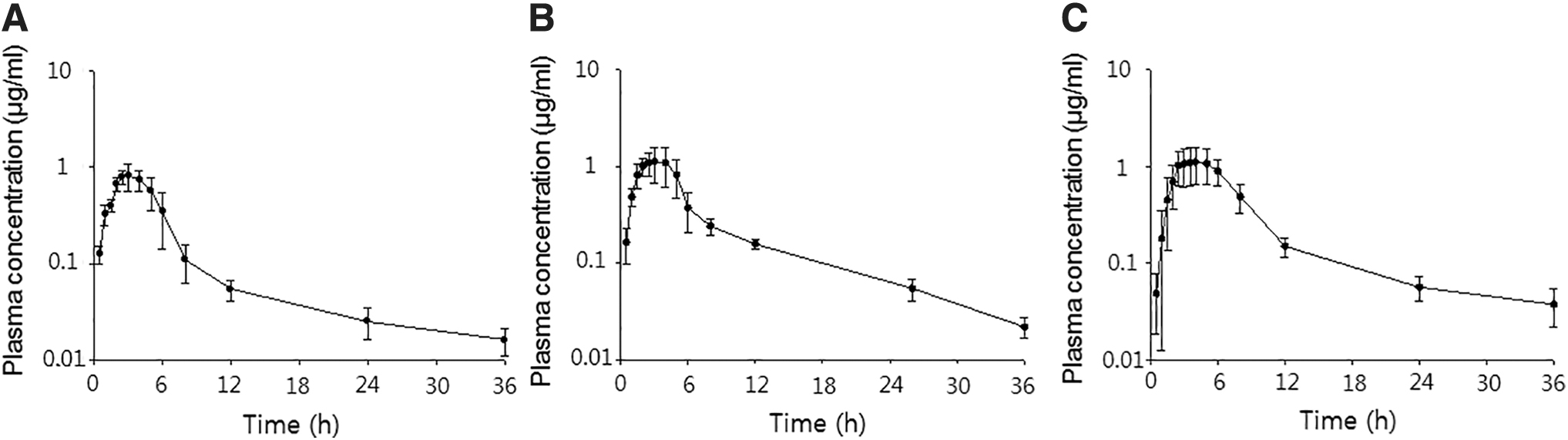
The mean panduratin A plasma concentration/time profiles of the mice, rats, and dogs after a single oral administration of 200 mg/kg of the fingerroot extracts are given in Figure 2. The pharmacokinetic parameters of panduratin A are given in Table 1.
The time courses of plasma panduratin A concentrations after oral administration of 200 mg/kg of fingerroot extracts to mice
Pharmacokinetic Parameters of Panduratin A After an Oral Administration of 200 mg/kg of the Dose Boesenbergia Pandurata Extracts (24 mg/kg as Panduratin A) in Mice, Rats, and Beagle Dogs
Data in mice were obtained by naive pooled method, and the others by the standard two-stage method.
AUCinf, area under the plasma concentration infinite; C max, peak concentration; T max, time to C max.
Panduratin A was slowly absorbed and the plasma concentration decayed bi-exponentially. The C max values at 3–4 h were 0.81, 1.30, and 1.16 μg/mL in the mice, rats, and dogs, respectively. The half-life and clearance values were 7.2 h and 5.02 L/h/kg for mice, 8.5 h and 2.96 L/h/kg for rats, and 14.8 h and 2.53 L/h/kg for dogs, respectively. The terminal half-life in dogs was significantly longer than that in rodents (P < .05) and the clearance times in rats and dogs tended to be shorter than in mice; the significance of these differences could not be evaluated owing to the use of naive-pooled mouse data.
Compared with data obtained after oral administration of panduratin A (5 mg/kg) to rats (AUC: 1.4 μg·h/mL; clearance: 2.7 L/h/kg; 12), the systemic concentration linearly increased with dose and there was no difference in clearance. In this study, the marker substance (24 mg/kg) was administered with the other ingredients in the extracts and the results indicated that it did not affect the pharmacokinetics of panduratin A. The short half-life (3.6 h) in the previous study might be attributable to the final sampling time (12 h), which was not long enough to evaluate the terminal phase.
The results of the allometric regression are given in Figure 3. The log-transformed clearance data correlated well with the log-transformed body weights (r 2 > 0.997) and the estimated exponent using simple allometric scaling was 0.98 (Fig. 3A); thus, the estimated clearance value was greater than the actual value (14). Therefore, the rule of exponents was used to improve prediction performance (14). The MLP of each species was incorporated into the clearance calculations (Fig. 3B) and estimated using the following equation 15 :

Allometric scaling of panduratin A Cl
The mean body weight and MLP of each species were adapted from the work by Mahmood. 16 After considering the MLP (Fig. 3B), the clearance for a 60 kg human was predicted to be 43.6 L/h (0.73 L/h/kg). A daily dose can be obtained by multiplying the clearance by the AUC to accurately represent pharmacodynamic activities. Because a previous study 2 showed that a 100 mg/kg dose of fingerroot extracts would likely exert sufficient inhibitory action against periodontitis, the AUC at that dose was extrapolated from the present results, i.e., half of the AUC for a 200 mg/kg dose of extracts. As mentioned previously, the systemic concentration of panduratin A after the administration of fingerroot extracts exhibited a linear increase with dose; thus, this extrapolation is reasonable. The proposed daily dose of panduratin A for a 60 kg human is 183 mg (∼3 mg/kg), which was calculated by multiplying the AUC (4.2 mg·h/L) by the clearance rate (43.6 L/h). Finally, the daily dose of fingerroot extracts of 1500 mg is suggested for a 60 kg human based on the panduratin A content (12%) in the extracts.
Discussion
Six over-the-counter drugs have long been used in Korea for treating complications associated with gum disease. Of the brands advertised as a treatment for gingivitis and periodontitis, five are derived from a titrated extract of the unsaponifiable fraction of Zea mays L., and one is a mixture of carbazochrome, ascorbic acid, calcium tocopherol succinate, and lysozyme chloride. Recently, all these products were downgraded to supplement status based on the recommendations of the Ministry Food and Drug Safety of Korea, because their pharmacological and clinical benefits were exaggerated by commercial advertisements. However, the inhibitory actions of fingerroot extracts against LPS-induced gingivitis and periodontitis in rats are promising, 2 and a clinical trial is being planned for human subjects with mild complications in the gum and periodontium. Therefore, determination of an appropriate daily dose of fingerroot extract is urgently needed. Only a few methods, based on either toxicity or pharmacological activity, are available for human dose determination. If no-observed-adverse-effect level of a substance is obtained, a first-in-man dose could be predicted in terms of body surface area and safety factor as suggested by the guideline provided by the U.S. Food and Drug Administration. 13 Although a lot of researchers have been using the method, its appropriateness was recently revisited with an example of resveratrol by Blanchard and Smoliga. 17 They insisted that interspecies scaling can be justified using pharmacokinetic data rather than simple conversion with body surface area. Furthermore, one may use pharmacologically active dose to estimate a human dose, when no toxicity information is given. Although a computational modeling approach using physiologically base pharmacokinetic model can be a candidate, 18 a model-independent analysis such as allometric scaling is more popular because of its simplicity.
In general, because food-grade natural products do not induce severe adverse effects, clinical doses could be suggested by allometry. To date, the method has been widely applied to a human dose prediction of herbal medicines such as avicularin, a bioactive flavonol isolated from a number of plants, 19 morphine in diluted tincture of opium, 20 rutin in a polyherbal product, 21 and mitragynine and 7-hydroxymitragynine in kratom extracts. 22 It can also be used to extrapolate a systemic exposure of toxic substance in food to humans: Faeste et al. estimated that human volume of distribution (1.24 L/kg) and clearance (0.24 L/h/kg) of deoxynivalenol, the most prevalent mycotoxin in cereals. 23
The pharmacokinetics of marker substances must be known to conduct interspecies allometry, and the relationship between the kinetic behaviors of these substances and pharmacodynamic effects of the extracts should be established in advance. In the present experiments, systemic levels of panduratin A, which is a marker compound of fingerroot extracts, were investigated in three species and allometric scaling was used to predict clearance in humans. Allometric scaling is based on the principle that energy requirements for, and rates of, physiological processes are closely associated with body size. 24 This type of scaling has been used to predict pharmacokinetic parameters (i.e., clearance, distribution volume, and half-life) of candidate drugs for humans using data derived from various animals. 25,26 However, the predictability of allometric scaling is a key issue and use of the rule of exponents was suggested by Mahmood and Balian 14 to improve predictive accuracy. Either MLP or brain weight can be integrated into a simple allometric equation obtained from a log–log plot of pharmacokinetic parameters versus body weight; if the slope value is 0.55–0.70, then simple allometry would provide more accurate data; if the slope value is 0.71–0.99, then MLP × parameter would be a better approach to estimate effects in humans; and if the slope value exceeds 1.0, then brain weight × parameter would be the best approach. Because the slope value obtained by simple allometry in this study was 0.98 (Fig. 3A), MLP was considered the best predictor of clearance in humans.
In addition to clearance, the distribution volume can be a useful parameter for determining the initial dose. However, when using this parameter, the substance should be administered intravenously because the distribution volume cannot be accurately determined with oral administration, owing to factors associated with bioavailability. In contrast, clearance can be estimated by the relationship between dose and systemic exposure (e.g., AUC) independent of the route of administration. This parameter could inform dosing rate and yield an AUC value corresponding to pharmacodynamic activity.
Kim et al. 2 reported that a 200 mg/kg dose of fingerroot extract and a 20 mg/kg dose of panduratin A resulted in significant improvements in LPS-induced periodontitis in rats. In this study, a daily dose for the upcoming clinical trial was suggested based on the expected results of a 100 mg/kg dose of the extracts, because the subjects in the trial will not be severe cases. Rather, the subjects will have a health status intermediate between patients and healthy volunteers, and the extracts will be framed as a health/functional food rather than a drug. Because this extract is currently administered daily at a dose of ∼700 mg in Korea, the 1500 mg dose suggested herein is not likely to cause any safety issues.
Although this approach may be a useful tool to predict the human dose, a couple of limitations should be considered. As mentioned by Wojcikowski and Gobe, 27 animal studies on herbal medicines could not perfectly reflect the unique evolution of each species because of interspecies differences in pharmacokinetic parameters, such as protein binding, tissue distribution, metabolism, and excretion. In addition, there would be more difficulties in pharmacodynamic aspects, because the capacity and sensitivity of receptors in animals may be different from those in humans. 28 AUC at the dose representing a proper anti-periodontitis action in rats was used for the dose selection, which could be a flaw in this study, because the efficacy in rats may not be equivalent to humans. Therefore, one has to carefully monitor whether the current dose would be therapeutically robust enough in clinical trials. Some errors are inevitable in the extrapolation of results from animals to humans. Nevertheless, animal studies properly designed can be useful for estimating an appropriate human dose using allometric scaling, which may not be an ideal method, but is one of the best scientific knowledge-based choices.
This study was the first to investigate systemic levels of panduratin A, which is an active substance in fingerroot extracts, after oral administration of the extracts to mice, rats, and dogs. The clearance rate of panduratin A in humans was predicted by allometric scaling based on the MLPs derived from animal data, which were subsequently used to estimate an appropriate daily dose of the extracts (1500 mg) for alleviation of gingivitis and periodontitis in humans. A clinical trial is being planned to determine the efficacy of the extracts. Although predicting the optimal dose for clinical studies is difficult, it is essential for both candidate drugs and health/functional foods. The allometric scaling approach is a reasonable method for determining appropriate doses, particularly of health/functional foods.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea Government (MSIP) (No. 2015R1A5A1008958), and by the World Class 300 project R&D grant funded by the Korea Small and Medium Business Administration (SMBA).