
Abstract
This study investigated the effect of Sinetrol-XPur on weight and body fat reduction in overweight or obese Korean participants. Among 100 overweight or obese participants enrolled in a 12-week randomized, double-blinded, controlled study, 86 participants completed the trial. Participants took either two Sinetrol-XPur tablets (450 mg per tablet) or two placebo tablets once a day. Bodyweight, body fat percentage, body mass index (BMI), body fat mass, waist circumference, and various safety parameters were measured. After the 12-week intervention, a significant reduction was observed in the body fat mass (P = .030) by dual-energy X-ray absorptiometry (DEXA), body weight (P = .002), and BMI (P = .002) compared to the placebo. Body fat percentage (P = .007) by DEXA showed a significant reduction in the Sinetrol-XPur group, but no difference compared to the control group. Abdominal metabolic risks by computed tomography and blood biochemistry analysis were significantly decreased in the Sinetrol-XPur group, but there were no differences between the Sinetrol-XPur and placebo groups. Safety profiles were not different between the two groups. These results suggested that Sinetrol-XPur significantly reduced body weight, body fat mass, and BMI in obese Korean subjects, which confirms the antiobesity effect of Sinetrol-XPur in the Korean population.
Introduction
Obesity is a multifactorial and persistent international issue.
1
Obesity refers to excess fat buildup in the body, which is influenced by genetic, behavioral, and environmental factors.
2
The westernized diet and sedentary lifestyles are responsible for obesity. As per the recent data, body mass index (BMI) equal to or >30 has led to 61% of global deaths.
1
In addition, obesity has many negative repercussions on the human body leading to hypertension, cardiovascular diseases, fatty liver, and type 2 diabetes mellitus.
3
–6
Obesity as a risk factor poses a physical, economic, and psychological global burden.
7
–9
According to a recent report, by 2025, the obesity rate for women and men are expected to rise 21% and 18%, respectively.
10
The obesity prevalence has also been increasing in South Korea for persons aged 19 years or older. A report by the Ministry of Health and Welfare published that the obesity prevalence in the Korean population has been risen by 42.3% for men and 26.4% for women by 2016 (
Recently, a polyphenolic dietary compound, Sinetrol, has turned out to be an active topic for improving obesity and obesity-associated complications. 13 –15 Sinetrol is a mixture of flavonoids, including anthocyanins and flavanones from citrus-based foods. Sinetrol-XPur is extracted by physical methods in a concentrated foam using particular varieties of orange, grapefruit, and guarana. 13,16
The potential mechanisms of Sinetrol-XPur against obesity may be based on antioxidation, 14 antiinflammation, 14 and lowering blood triglyceride (TG), and cholesterol contents. 16 One study attributed the effect of Sinetrol-XPur on lipid profiles to the activation of cAMP-dependent uncoupling protein-2 (UCP-2) in leptin-deficient obese mice. 16 Another study showed the correlation of the lipolytic effect and the increased gene expressions of adipose triglyceride lipase (ATGL), A-kinase anchoring protein 1 (AKAP1), and perilipin-1 (PLIN) and reduced expression of phosphodiesterase 3B (PGE3B). 17
Although few human studies have been published on the effects of Sinetrol-XPur, suggesting that this flavonoid compound has a potential antiobesity effect, Dallas et al. showed that Sinetrol-XPur reduced BMI after 12 weeks of supplementation, although it was a small intervention with 20 overweight subjects. 13 In a continued work, Dallas et al. reported beneficial effects in body fat composition, including the improvement in glycemic, inflammatory, and oxidative status in 12-week, in a double-blinded, parallel, clinical trial with 95 healthy overweight French. 14 Along the same line, Sinetrol-XPur supplementation led to a significant reduction in abdominal fat, waist circumference, and improved skeletal muscle mass in 25 overweight male French subjects. 15
It is well established that genetic factors are among the risk factors for obesity. 18 There may be ethnic differences that are unknown. 19,20 The types of obesity vary in western and Asian countries. Koreans mostly have apple-type obesity, but many westerners have the pear-shaped type of obesity. 21,22 In addition, different lifestyle and dietary environment could have an impact on obesity. 18,23
To the best of our information, no clinical trial has been conducted on the efficacy and safety of Sinetrol-XPur in overweight or obese Korean subjects. Therefore, this study aimed to assess the Sinetrol-XPur's effect against obesity via randomized, double-blind, placebo-controlled clinical trial.
Materials and Methods
Study subjects, inclusion, and exclusion criteria
The study subjects were recruited from Kangbuk Samsung Hospital, Seoul, Korea. A total of 100 healthy obese and overweight male and female subjects were enrolled in the study. The subjects were >19 years and <60 years and had BMIs of >25.0 kg/m2 or <30.0 kg/m2. All agreed to participate, and those who were not diagnosed with any disease were included in this study. Exclusion criteria included the following: having any cerebrovascular disease (cerebral infarction, cerebral hemorrhage, and so on) within the last 6 months; have a heart illness (angina, myocardial infarction, heart failure, and arrhythmia requiring treatment); any history of cerebrovascular disease and heart disease, but clinically stable; consumed drugs affecting body weight within the last month (inhibitors and appetite suppressants); have consumed functional food/supplement for obesity improvement; central nervous system disorder, sign of depression, treated with drugs, or rehabilitation; taking psychiatric drugs, beta-blockers, diuretics, contraceptives, steroids, and female hormones; uncontrolled hypertension >160/100 mmHg, fasting blood sugar (126 mg/dL or more), random blood sugar (200 mg/dL or more); diabetic taking autologous or oral hypoglycemic agents or insulin; person with <0.1 μU/mL of TSH or >10 μU/mL; creatinine level more than twice; AST or ALT is three times higher; gastrointestinal disorders, alcohol use, medical history; unable to exercise due to musculoskeletal disorders, joined any commercial obesity program within the last 3 months; participated or planned to participate in other clinical trials within the last month, pregnant or plan to become pregnant or nursing mothers; lost >5% of their weight in the last 3 months; and a person deemed inappropriate by the investigator for other reasons were excluded from the trial.
Test material
Sinetrol-Xpur is mainly a citrus fruit extract of grapefruit (Citrus paradisi), orange (Citrus sinensis Osbeck), and guarana (Paullinia cupana). In particular, Sinetrol-Xpur is a polyphenolic-rich ingredient, of which naringin and hesperidin are the main markers of grapefruit and orange, respectively. And the guarana extract provides a small amount of caffeine. 13 –15 The participants were instructed to take two tablets once a day before a meal for 12 weeks; a test tablet contained 450 mg of Sinetrol-XPur. The placebo has an identical quantity of maltodextrin. The placebo tablet was produced with the same look, taste, and energy content. The Rpbio Company, Korea, prepared the test and placebo tablets.
Study design
This 12-week randomized, double-blind, placebo-controlled parallel trial on overweight and obese Korean was conducted from June 2018 to February 2019. The Ethics Board Committee of Kangbuk Samsung Hospital, Seoul, Korea approved the study protocol (IRB No. 2018-04-003).
The prescreening was conducted by a telephone conversation and subjects who met the eligibility criteria were scheduled for a baseline visit. Participants were satisfied with the inclusion and exclusion criteria. Written informed consent was obtained from all participants before enrollment. Assessments were conducted every 6 weeks, that is, week 6 and week 12 after randomization (first visit for screening: −2 weeks, second visit: 0 weeks, third visit: 6 weeks, fourth visit: 12 weeks). At the baseline visit (second visit), subjects were randomly assigned to receive either Sinetrol-XPur supplements or placebo. Randomization lists were computer-generated by a statistician. Subjects, as well as investigators, were blind to the intervention assignment until the end of the study.
The sample size was calculated with a significance between treatment and placebo groups at P = .05 and a power of 80% using the result of body fat mass and percentage reported by Nosaka et al. 24 The required number of subjects was determined using a power calculation according to published guidelines for human dietary intervention studies. 25,26
The Sinetrol-XPur and placebo tablets were provided by the investigators every 6 weeks, and compliance was assessed at every follow-up. Compliance was monitored through a trained researcher by calculating remnant tablet strips from the participants at the third and fourth visits. Before and after the intervention, both groups were evaluated for various parameters, namely anthropometric, biochemical assessments, vital signs, energy intake, and exercise. The participants were also examined for any adverse effects during the intervention.
Efficacy measurement
On each visit, the anthropometric parameters, including height, weight, hip circumference, waist circumference, diastolic blood pressure (DBP), and systolic blood pressure (SBP) were measured and recorded by the trained workforce. As for the primary outcome, the dual-energy X-ray absorptiometry (DEXA; Lunar Prodigy Advance, GE, USA) was used to assess the total body fat percentage and body fat mass (kg) before and after the 12-week intervention. As for trunk fat, computed tomography (CT; Light Speed VCT XTE, GE, Japan) was used to assess visceral fat, subcutaneous fat, total abdominal fat, and visceral subcutaneous ratio. Bioelectrical impedance analysis (BIA, Inbody 720; Biospace, Korea) was conducted to measure body fat mass, body fat percentage, and visceral fat area.
The blood samples were collected after 12 h overnight fasting. Blood samples were assessed for lipid profile (total cholesterol [TC], TG, high-density lipoprotein [HDL] cholesterol, and low-density lipoprotein [LDL] cholesterol), fasting glucose, and high-sensitivity C-reactive protein (hs-CRP).
Safety measurement
For all the subjects before and after 12 weeks of intervention, safety assessments included the following: blood parameters such as white blood cells, red blood cells, hemoglobin, hematocrit, platelets, lymphocytes, aspartate aminotransferase, alanine aminotransferase, total bilirubin, gamma-glutamyl transpeptidase, creatinine, blood urea nitrogen, uric acid, and pulse.
Diet and exercise
All participants were provided education on diet and physical activity during the intervention period. It was recommended to reduce the energy intake to 500 kcal/day less than usual. In addition, they were trained to perform exercises corresponding to 300 kcal or more every day. Participants were instructed to carefully consume high fat and high carbohydrates and alcohol drink, and refrain from high-calorie snacks or midnight snacks. The participants were instructed to submit their dietary records and exercise logs on the next visit. The dietary intake data were estimated using the CAN PRO 4.0 program (The Korean Nutrition Society, Seoul, Korea).
Statistics
Statistical data were analyzed using SAS 9.4 (SAS Institute, Cary, North Carolina, USA). Significances of efficacy assessment and safety assessment were performed in the per-protocol groups (n = 86) and intention-to-treat group (n = 100), respectively. Differences in efficacy parameters before and after 12 weeks intervention were determined using the paired t-test. Between groups with changes before and after treatment, the two sample t-test or Wilcoxon rank-sum tests were used according to normal distribution or not. Finally, obesity could be associated with sex and baseline characteristics so that the final significant differences between Sinetrol-XPur and placebo groups were determined using an ANCOVA test adjusted for baseline values and sex. The difference of safety parameters within and between groups was determined by using the paired t-test and two-sample t-test, respectively. All continuous data are shown as mean ± standard deviation, and the P-value <.05 was considered as statistically significant.
Results
The baseline characteristics and dietary assessment
One hundred six (106) subjects were screened for this intervention trial. One hundred subjects were randomly assigned to the Sinetrol-XPur (n = 50) group and placebo (n = 50) groups. Fourteen participants were excluded due to consent being withdrawn (n = 4), primary efficacy test was lost (n = 1), participants with <75% compliance (n = 2), subjects forgot to return remnant blister strips (n = 2), subjects missed visit window (n = 3), and subjects lost to follow-up (n = 2). At the end of the study, 86 subjects, Sinetrol-XPur (n = 44) and placebo (n = 42) were included in the study (Fig. 1). The baseline demographic characteristics were similar for both test and control groups. For energy intake and physical activity for each group during the intervention period, no significant differences were observed (Table 1). No adverse effects were reported for the participants of the full analysis set.

Flow diagram of study design. FA, full analysis; PP, per-protocol.
Demographic Characteristics of Participants
P-value by chi-square test.
P-value by two sample t-test.
P-value by Fisher's exact test.
Efficacy assessment
After 12 weeks of intervention, the body weight was significantly decreased by 1.81% (1.35 ± 2.40 kg; P = .000) in the Sinetrol-XPur group compared with 0.25% reduction in the control group (0.20 ± 1.63 kg; P = .431) (Fig. 2A). The change observed was statistically significant (P = .003 by Wilcoxon rank sum test; P = .002 as determined by ANCOVA test) (Table 2). The BMI in the Sinetrol-XPur group was reduced by 2.32% (0.64 ± 0.85 kg/m2; P < .000), compared with the control group 0.65% (0.18 ± 0.62 kg/m2; P = .065). A statistically significant difference was observed between the two groups (P = .002 by Wilcoxon rank sum test; P = .002 by ANCOVA test) (Table 2 and Fig. 2B).
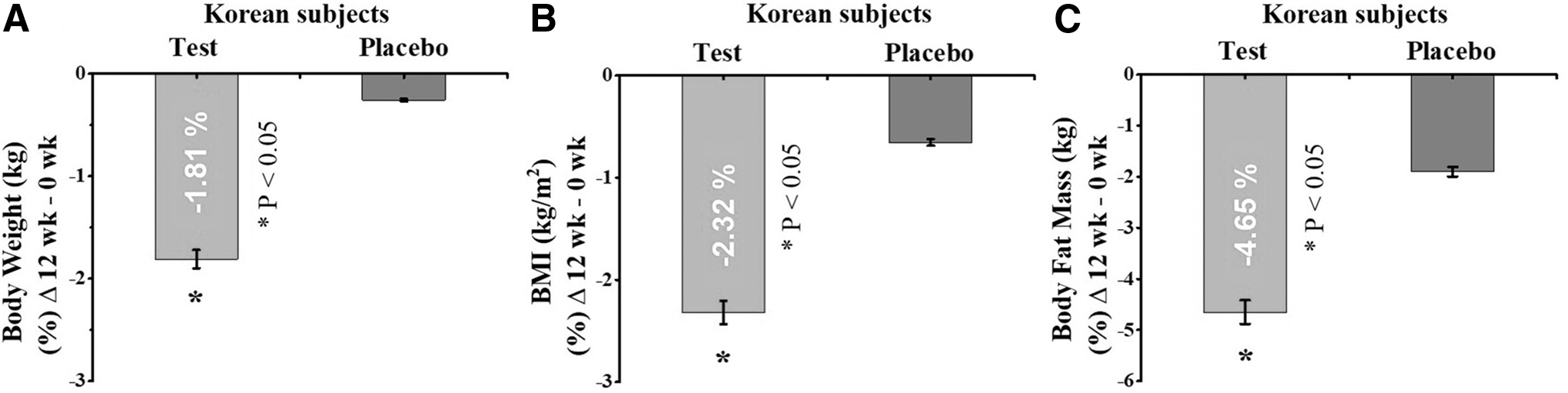
Effect of Sinetrol-XPur supplementation on
Efficacy Assessment in Anthropometrics, Blood Chemistry, and Blood Pressure Before and After 12-Week Treatment
Values are presented as mean ± SD.
Compared within groups: P-value by paired t-test.
Compared between groups: P-value by Wilcoxon rank sum test.
Compared between groups: P-value by ANCOVA adjusted baseline values and sex.
BIA, bioelectrical impedance analysis; BMI, body mass index; CT, computed tomography; DEXA, dual-energy X-ray absorptiometry; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; WC, waist circumference.
Following 12 weeks of Sinetrol-XPur intervention, the waist circumference (−1.97 ± 3.81 cm; P = .001 by paired t-test), the visceral fat area (−14.60 ± 24.72 cm2; P = .000 by paired t-test), and total abdominal fat area (−22.64 ± 51.10 cm2; P = .005 by paired t-test) as measured by CT were significantly changed. However, the changes between the groups were not statistically significant. No significant differences were observed for the subcutaneous fat area and visceral/subcutaneous fat ratio between the groups (Table 2).
Compared to 1.9% reduction in placebo (0.51 ± 1.63; P = .046), the body fat mass was decreased by 4.65% (1.17 ± 2.11; P = .000) in the Sinetrol-XPur group as measured by DEXA. The ANCOVA test showed a statistically significant (P = .030) difference between groups (Table 2 and Fig. 2C). Compared to placebo, change in body fat percentage (−0.87 ± 2.07; P = .007 by paired t-test) was significant in the test group (Table 2); however, no significant differences were seen between the Sinetrol-XPur and placebo groups. After 12 weeks of intervention, no significant changes were observed in body fat mass, body fat percentage, and visceral fat cross-sectional area, measured by BIA (Table 2).
Changes in blood chemistry parameters during the 12-week Sinetrol-XPur intervention are shown in Table 2. No significant changes were observed between groups for lipid profile, fasting blood sugar, and hs-CRP (an inflammation marker). No significant change was observed for SBP and DBP (Table 2).
Safety
The safety evaluation was performed on blood parameters and vital signs. Compared to baseline, the hepatotoxicity markers, such as ALT, AST, gamma-glutamic transpeptidase (γ-GTP), showed a significant reduction in the intervention group. No significant differences were observed between the two groups for safety parameters (Table 3). At each visit, the subjects were evaluated for side effects or symptoms. No moderate or severe side effects were observed during the intervention study (Table 4). Total calorie intake and physical activity by exercise were not different between Sinetrol-XPur and placebo group, respectively (data not shown).
Safety Assessment in Blood Biochemistry Before and After 12-Week Treatment
Values are presented as mean ± SD.
Compared within groups: P-value by paired t-test.
Compared between groups: P-value by two sample t-test.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; γ-GTP, gamma-glutamic transpeptidase; Hb, hemoglobin; Hct, hematocrit; RBC, red blood cell; WBC, white blood cell.
Adverse Events Between Sinestrol and Placebo Group During 12-Week Intervention
Discussion
We investigated the effects of Sinetrol-XPur supplementation on body fat (%) and body fat content by DEXA, anthropometric parameters, and blood chemistry in overweight/obese Korean subjects.
Obesity and excess body fat are threatening the global population during the past decade. Many studies have shown that health/functional foods have emerged as a substitute to prevent or treat obesity. 27 The bioactivities of functional foods have been ascribed to the presence of several polyphenols that have their impact on the metabolic pathways. 28
Several studies have revealed that the inhibitory action of flavonoids on cAMP-phosphodiesterase activity leads to rising cellular cAMP levels. 13,29 Elevated cAMP levels stimulate lipolysis by activating cAMP-dependent protein kinase A (PKA). 30 The latter activates AMP response element-binding protein (CREB), 31,32 leading to the increased expression of UCP-2. UCP-2 plays an important role in body weight regulation, energy stability, and thermoregulation in humans. 33 Hence, these flavonoids could plausibly be used in the management of obesity.
There has been a growing interest in the use of citrus derivatives to treat obesity. The animal studies based on blood orange juice 34 and grapefruit juice 35 have provided insight. Later, a clinical study by Fujioka et al. described the weight loss effect of grapefruit consumption in ninety-one obese adults. Compared to placebo, a 12-week supplementation of naringin (flavanone) rich raw grapefruit, grapefruit juice, and grapefruit capsules (500 mg) resulted in 1.6, 1.5, and 1.1 kg weight loss, respectively. 36 In contrast, another study showed that the intake of grapefruit or its juice had no significant effects on physiological variables except for a slight increase in HDL in obese subjects. 37 Still, the data on the potential health benefits of fruits containing polyphenols on obesity are inconclusive.
As a polyphenolic compound, Sinetrol-XPur showed a significant effect on fat reduction in human subjects mainly from the western countries. 13 –15 However, no clinical study has been conducted on the Korean population. Ethnically, Koreans are between non-Korean western and African populations. Notably, the intake of flavonoid (Sinetrol) concentration in natural foam (fruits) is less compared to Sinetrol-XPur (prepared with much higher concentration).
In this study, Sinetrol-XPur supplementation resulted in a significant reduction of body weight in the Korean subjects. Our results are supported by clinical trial (12-weeks) findings by Dallas et al. and Cases et al. 14,15 We have shown that the body fat mass content was significantly reduced with Sinetrol-XPur supplementation compared with placebo, similar to the study findings of Dallas et al., where Sinetrol-XPur resulted in a significant reduction of body fat compared with control. 14 In contrast, no significant difference was reported for body fat percentage in healthy overweight adults, as described in a previous study. The authors highlighted that the grapefruit had a specific effect on central obesity. 38 On BMI reduction, in contrast to our study, no statistically significant change was reported by Dallas et al. 14 As per the recent studies, BMI is an important tool to assess abdominal obesity. 39,40
In this study, supplementation with Sinetrol-XPur was effective for reducing body fat (%) and waist circumference. However, the difference was not statistically significant. In contrast, body fat (%), waist circumference, and hip circumference were significantly changed after the supplementation of Sinetrol-XPur in a previous clinical study. 14 Similarly, Cases et al. showed that Sinetrol-XPur supplementation led to a significant change in abdominal fat, waist circumference, hip circumference, and the waist-to-hip ratio. 15
Another study by Dow et al. reported that grapefruit consumption for 6 weeks significantly reduced waist circumference (a measure of central obesity) in healthy overweight adults, without any significant between-treatment difference. 38 Previous studies have shown significant reductions in body fat percentage 14 and waist circumference. 14,15 Although there were no significant differences in the above parameters between the Sinetrol-XPur and the placebo groups, the parameters still showed the reductions. Similar to previous report, 14 no significant changes in TC, TG, LDL-C, HDL-C, hs-CRP, SBP, and DBP were observed in this study after 12 weeks of Sinetrol-XPur supplementation. In contrast, a significant reduction was reported for hs-CRP, as reported by previous studies. 14,15 This contrariwise continent-dependent difference in the effect of Sinetrol-XPur may be the result of not only the race of Koreans but also other dietary environments.
The strengths of the present study include the design of the study, which is a randomized, double-blind, placebo-controlled parallel trial, and the large sample size. In addition, the study results have supported the findings of previous clinical trials. The participants were recruited from one clinical center of Korea; this could cause selection bias. Therefore, to verify this result, a longer intervention study is required in multiple clinical centers. In this study, a 12-week supplementation of Sinetrol-XPur displayed a reducing trend for body weight, body fat mass, and BMI, suggesting a plausible role of Sinetrol-XPur in obesity reduction without any adverse effects. This is the first clinical study assessing the effects of Sinetrol-XPur on overweight/obese Korean subjects.
In conclusion, in the present study, our outcomes indicated that 12 weeks of Sinetrol-XPur intake might have a positive effect on ameliorating body weight, body fat mass, and BMI in overweight and obese Korean individuals. No adverse effects were observed in the participants. Our data have supported the previously reported clinical studies from France. Taken together, we suggested that Sinetrol-XPur could act as a potential antiobesity compound. Further studies are warranted to investigate the long-term effects of Sinetrol-XPur.
Footnotes
Author Disclosure Statement
N.K.K., H.C.S., and M.H.B. are employees of Rpbio Co. Ltd. Republic of Korea. For all other authors, no competing financial interests exist.
Funding Information
The study was funded by Rpbio Co. Ltd. company, Korea, and partly supported by Gachon University Research fund of 2019 (GCU-2019-0318).