
Abstract
Deep seawater (DSW) has been investigated for its lipid-lowering effects, but clinical evidence is still far from conclusive. Therefore, this study was conducted to examine the effects of refined DSW (RDSW) on hypercholesterolemia. In this randomized, double-blind, placebo-controlled trial, 78 Korean participants were randomized to either an RDSW group that drank RDSW for 8 weeks or a placebo group. Clinical laboratory information was collected from all subjects at 0, 4, and 8 weeks. Both groups showed a significant reduction in total cholesterol (TC), whereas only the RDSW group demonstrated a significant decrease in low-density lipoprotein cholesterol (LDL-c) during the study. Stratified analysis of both groups revealed a significant reduction of TC in the moderately high TC subgroup. However, only the RDSW exhibited a significant decline of LDL-c in the high LDL-c subgroup. In addition, lipoprotein(a) decreased significantly in the RDSW group, but not in the placebo. RDSW did not affect other lipid profiles, including high-density lipoprotein cholesterol (HDL-c), triglyceride, free fatty acid, apolipoproteins, and other markers including inflammation marker, hematological parameters, blood and urine chemistry, and vital signs. RDSW improved lipid profiles by decreasing TC and LDL-c while maintaining HDL-c levels in people with hypercholesterolemia.
Introduction
The incidences of cardiovascular diseases (CVDs) have increased steadily worldwide mainly because of the westernization of eating and living habits, 1 and these diseases now account for 31% of all global death. 2 In addition, growth and aging of the population are the two vital factors that contribute to the increased number of CVD deaths. 3 Hypercholesterolemia is a pathological condition in which the total cholesterol (TC) concentration is elevated to 240 mg/dL or higher. 4 This event can facilitate O-GlcNAcylation, a post-translational modification of proteins that is mediated by addition of O-linked N-acetylglucosamine (O-GlcNAc) moieties to the specific serine and threonine residues of the protein molecules. Such a process is also known to trigger dyslipidemia. 5 Dyslipidemia, a risk factor for CVDs, is a pathological condition in which the concentrations of TC, especially low-density lipoprotein cholesterol (LDL-c) and triglyceride (TG), are elevated, but the concentration of high-density lipoprotein cholesterol (HDL-c) is decreased. 6 Dyslipidemia can also lead to various complications, including atherosclerosis 7 and metabolic disorders including type 2 diabetes and obesity. 5 However, early recognition of dyslipidemia is difficult because there are few objective symptoms associated with its progression. 8
Oxidation of accumulated LDL-c in the blood generates chemoattractant cytokines that attract different types of white blood cells (WBCs) to the arterial wall. At the same time, macrophages absorb the oxidized LDL-c and convert it into foam cells containing lipids. As the converted foam cells accumulate in the endothelium of the vessel, the circulation of the bloodstream decreases and atherosclerosis may develop gradually. 9 This can create stenosis or blood clots in legs or organs such as the brain and heart, eventually leading to CVD. 10 Because dyslipidemia is the major cause of these diseases, it is important to manage it to prevent their occurrence.
In general, most patients with dyslipidemia are prescribed LDL-c lowering drugs, which are commonly statin derivatives that are inhibitors of 3-hydroxy-3-methylglutaryl-coenzyme A reductase. 9 However, these statin derivatives have been reported to potentially cause various side effects, including myalgia, weakness, and liver or renal dysfunction. 11 Therefore, alternative therapies to replace them have recently been attracting attention. These treatments include red yeast rice, berberine, phytosterols, polyphenols, and flavonoids. 12
Deep seawater (DSW), seawater from a depth of >200 m, is relatively free from contaminants compared with surface water. Moreover, water from that depth is characterized by less photosynthesis and low temperature, implying that there is minimal to no bacterial activity. DSW contains a number of minerals among which magnesium (Mg) and calcium (Ca) are the most abundant. 13,14 Mg is associated with energy production, muscle tone, heart rhythm control, and enzyme activity 15 ; whereas Ca plays an important role in bone structure, hormone secretion, and vasomotor control. 16 Moreover, DSW has been reported to combat diseases such as obesity, hypertension, diabetes, osteoporosis, inflammation, and gastric ulcers. 17
There is also substantial evidence that DSW could improve lipid profiles. In vivo experiments with high-cholesterol-fed rats revealed that DSW decreased lipid accumulation in the liver and improved serum lipid parameters. 18 In high-fat diet (HFD)-induced diabetic mice, DSW prevented weight gain and depleted plasma and hepatic TGs and cholesterol in a dose-dependent manner. 19 Moreover, our previous study revealed that DSW suppressed increases in the TC content in high glucose- or free fatty acid (FFA)/glucose-treated HepG2 hepatic cells by inducing transcription of LDL receptor and apolipoprotein A1 (apo A1). 20 For these reasons, DSW is emerging as an alternative treatment for dyslipidemia. This prompted us to investigate the effects of refined DSW (RDSW) on serum lipid profiles in Korean participants suffering from hypercholesterolemia.
Materials and Methods
Preparation of RDSW and placebo
The preparation RDSW and placebo are described in the Supplementary Data (Supplementary Tables S1 and S2).
Study design
This was a single-center, randomized, double-blind, placebo-controlled trial conducted between February and September 2018 at Ilsan Dongguk University Hospital, Korea (Trial registration number: KCT0003702,
Determination of the sample size
This study did not control the type I error because it was a clinical trial in the exploratory phase to evaluate the physiological impact of RDSW. The number of subjects was calculated based on a previous clinical trial evaluating the impact of RDSW. 21 According to this previous trial, the TC in the RDSW group was reduced by ∼32.2 mg/dL, which was significantly lower than that in the placebo group. In addition, the standard deviation was conservatively assumed to be the largest value of 33.4. Using these values, the number of subjects required to obtain a minimum power of 95% at a significance level of 5% was 31 per group and the number of subjects considering the dropout rate of 20% was 39 per group. Therefore, a total of 78 subjects were registered in this study.
Subjects
Male and female Korean adults aged 19–80 years with hypercholesterolemia (TC = 200–299 mg/dL) were voluntarily recruited through advertisements on posters, in local newspapers, and banners in Dongguk hospital. Blood samples were collected from the subjects to screen for their eligibility. Exclusion criteria included a hyperlipidemia high-risk group requiring drug administration, hypertension, pregnant or nursing women, and heavy drinkers or smokers. Those who had hypersensitivity to the components of test foods or clinically significant histories were excluded. In addition, individuals were excluded if they had a history that might influence the assessment of test foods such as hepatobiliary, cardiovascular, endocrine, respiratory, gastrointestinal, oncologic, musculoskeletal, psychiatric, or central nervous system conditions. Subjects were included if they had already taken drugs or supplements that affect blood lipid levels. However, subjects were excluded if they had stopped taking drugs that affect blood lipid levels, had taken new drugs, or had changed their doses within the 2 weeks before starting the study. They were also excluded if they had started taking supplements that may affect blood lipid levels within the 2 weeks before the initiation of the study. All eligible subjects agreed to follow the study protocol, voluntarily signed informed consent, and were randomly assigned to groups that received either an RDSW or placebo treatment for 8 weeks. Subjects were requested to maintain their usual diet and physical activity during the trial.
Randomization and blinding
The randomization was performed by a researcher who did not interact with the subjects. The researcher used the R software (R Foundation, Vienna, Austria) to perform random assignments independently through block randomization with a block size of 4, and the results of the assignment were kept sealed until the end of the study. Random assignments were managed by the sponsor who was not involved in the study.
The subjects were assigned screening numbers in the order in which they provided consent. Next, a registration number was assigned by checking the agreement and eligibility. As this trial was conducted in a double-blinded manner, it was not known which group has been allocated according to the registration number. The RDSW and placebo formulations were identical in appearance and characteristics so that no difference was observed between them with the naked eye. The test products were labeled with the registration number according to the random assignment, and both subjects and researchers were blinded to each person's assignment until the study was completed.
Clinical laboratory analysis
Fasting blood samples were collected from the subjects at weeks 0, 4 and 8. Complete blood cell counts were conducted and the WBC, red blood cell (RBC), hemoglobin, hematocrit, and platelet were determined using a Sysmex XN 9000 hematology analyzer (Sysmex, Inc., Kobe, Japan). In addition, biochemical markers, such as total protein, albumin, total bilirubin, blood urea nitrogen (BUN), creatinine, aspartate transaminase, alanine transaminase, alkaline phosphatase, glucose, and high-sensitivity C-reactive protein (hs-CRP) were measured using COBAS 8000 (Roche Diagnostics, Basel, Switzerland). Blood lipid profiles including TC, TG, LDL-c, HDL-c, FFA, apo A1, apolipoprotein B (apo B), and lipoprotein(a) [Lp(a)] were analyzed using COBAS 8000 and Roche Modular Analytics E170 (EEE) (Roche Diagnostics). Urine analysis was conducted using a UriScan Pro II (YD Diagnostics Corp., Seoul, Korea) that determined the color, specific gravity (S.G), pH, protein, glucose, ketone, bilirubin, occult blood, urobilinogen, and nitrite of the urine. Additional microscopic evaluation was also performed to trace the presence of RBC and WBC in the urine.
Statistical analysis
Continuous data were presented using descriptive statistics and analyzed by independent two sample t-tests. Moreover, categorical data were described based on frequency and percentage (%) using the chi-squared test and Fisher's exact test. To analyze the blood and urinary parameters, an independent two-sample t-test and Wilcoxon's rank sum test were performed for comparative analyses between the groups. Other additional analyses used repeated-measures analysis of variance and analysis of covariance with age as the covariate. A paired t-test and Wilcoxon's signed rank test were used to compare pre and post results within groups. Statistical analysis was performed using the SPSS version 20.0 statistical software package (SPSS, Inc., Chicago, IL, USA). A value of P < .05 was considered statistically significant.
Results
Baseline characteristics of the subjects
A total of 78 eligible subjects consented to participate in this study. Among them, 39 were randomly assigned to the RDSW group and 39 to the placebo group. During the study, two subjects from the RDSW group and two subjects from the placebo group withdrew consent for personal reasons. In addition, we lost touch with one subject from the placebo group. Therefore, 37 of the 39 subjects who were assigned to receive RDSW (94.87%) and 36 of the 39 subjects who were assigned to receive placebo (92.31%) completed the study. Among the 73 subjects, the percentage of those who were administered >75% of the RDSW or placebo provided was similar between the two groups (36 of 37 subjects [97.58%] in the RDSW group and 35 of 36 subjects [97.29%] in the placebo group). Therefore, the primary and secondary efficacy analysis included 36 patients in the RDSW group and 35 in the placebo group (Fig. 1). Except for the body weights, there were no significant differences in the baseline characteristics between the two groups (Table 1).

Study flow chart of patient progress through the randomized clinical trial from enrollment to analysis. RDSW, refined deep seawater.
Baseline Demographic and Clinical Characteristics of Study Participants
Data are given as means ± standard deviations.
P-value: obtained from independent two-sample t-test.
P-value: obtained from chi-squared test.
P-value: obtained from Wilcoxon's rank sum test.
P-value: obtained from Fisher's exact test.
ALT, alanine transaminase; Apo, apolipoprotein; AST, aspartate transaminase; BP, blood pressure; HDL, high-density lipoprotein; hs-CRP, high-sensitive C-reactive protein; LDL, low-density lipoprotein; RDSW, refined deep seawater; TC, total cholesterol.
RDSW improved lipid profiles and did not affect systemic inflammation
Both the RDSW and placebo groups showed a significantly lower TC (P < .05) at the 8th week compared with the baseline, but there was no significant difference between the groups. Of importance, at the 8th week, the LDL-c was significantly reduced from the baseline (P < .05) in the RDSW group, but not in the placebo group. However, there was no significant difference between the groups. Furthermore, although Lp(a) decreased consistently in both groups throughout the study, the change was significant (P < .05) in the RDSW group, but not in the placebo group. The HDL-c did not differ significantly over time within the groups or between the groups. The RDSW group did not show any difference in the apo A1, whereas the apo A1 in the placebo was found to be significantly lower at week 8 compared with baseline. However, there were no significant differences in the other lipid parameters or in the inflammation marker, hs-CRP (Fig. 2).
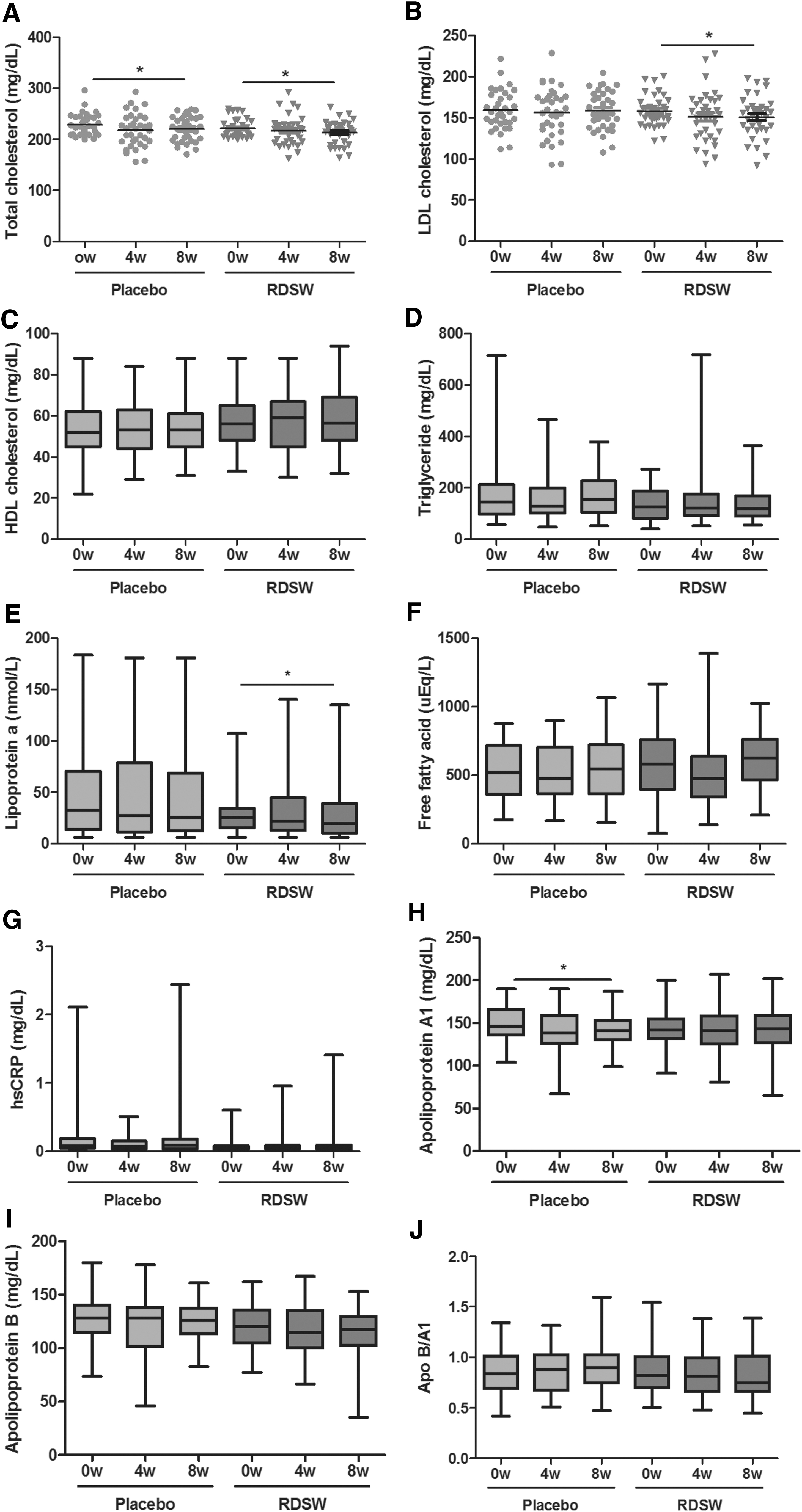
Effects of RDSW or placebo administration on lipid profile and inflammation. The change of
Effects of RDSW were more prominent in the subgroups with high TC and LDL-c levels
To further understand the impact of RDSW on the hypercholesterolemic patients, we conducted stratified analyses according to the disease severity based on the TC and LDL-c levels at baseline. For this, all subjects were subdivided into moderately high TC (baseline level = 200–239 mg/dL) and high TC (baseline level ≥240 mg/dL) subgroups as well as moderately high LDL-c (baseline level = 100–130 mg/dL) and high LDL-c (baseline level >130 mg/dL) subgroups. Our results showed a significantly lower TC level in the moderately high TC subgroup of the RDSW group, but not of the placebo group, at the 8th week compared with baseline. However, the TC levels in the high TC subgroup of both the placebo and the RDSW groups at baseline were reduced significantly at the 8th week. No significant differences in the LDL-c levels during the study were found in the moderately high LDL-c subgroups of both the placebo and RDSW groups. However, significantly lower LDL-c levels were evident in the high LDL-c subgroup of the RDSW group, but not of the placebo group, at 8th week compared with the baseline (Fig. 3).

Effects of RDSW or placebo administration in subgroups stratified by TC or LDL-c level. The changes in TC in
Adverse events
Only a few cases of adverse events were reported by the patients with four from the placebo group (11.43%) and three from the RDSW group (8.33%). In the placebo group, one patient experienced enteritis and another experienced steatocystoma. In the RDSW group, one volunteer caught cold and another suffered from headache, irrelevant to this study. One subject from the RDSW group and two volunteers from the placebo group reported diarrhea relevant to this study, but they recovered without any treatment (Supplementary Table S3).
There were no significant change in the blood pressure and pulse rate at the 8th week compared with baseline (Supplementary Table S4). In addition, the placebo and RDSW groups did not show any significant intra- or intergroup differences between week 0 and the 8th week in the complete blood count (CBC) (Table 2) and biochemical parameters except for BUN (Table 3). Compared with the baseline, at week 8, the change in BUN in the RDSW group was significantly higher vs the placebo group (P < .01).
Effects of Refined Deep Seawater or Placebo Administration on Complete Blood Count
Data are given as means ± standard deviations.
P-value obtained from independent two-sample t-test.
P-value obtained from Wilcoxon's rank sum test.
Hb, hemoglobin; Hct, hematocrit; RBC, red blood cell; WBC, white blood cell.
Effects of Refined Deep Seawater or Placebo Administration on Blood Biochemistry Compared with the Placebo
Data are given as means ± standard deviations.
P-value obtained from independent two-sample t-test.
P-value obtained from Wilcoxon's rank sum test.
BUN, blood urea nitrogen; ALP, alkaline phosphatase.
Discussion
This study primarily evaluated the changes in the lipid profiles in patients with TC 200–299 who were assigned to the RDSW group or placebo group during 8 weeks. Although hypercholesterolemia is defined as >239 mg/dL of TC in serum, subjects with slightly elevated TC between 200 and 239 mg/dL are considered as borderline high or representative of subclinical hypercholesterolemia. Therefore, they were also included in this study to evaluate the effect of RSDW in subclinical hypercholesterolemia.
In a previous study on RDSW, which was conducted in Taiwan, the subjects drank 1050 mL of DSW that had a strength of 1430 ppm. 21 The dosing was performed daily for a period of 6 weeks that resulted in a significant decrease in the level of TC and LDL. Compared with this trial, subjects in our study drank 880 mL of DSW with strength of 2387 ppm daily for 8 weeks. Furthermore, accumulating evidence indicates that the mortality rates in patients suffering from CVDs are negatively correlated with water hardness 22 and the strength of water has a positive effect on the clinical parameters including lipid levels. 21 Therefore, it is conceivable that the 8-week treatment period in our study is adequate for RDSW to have an effect on various parameters of patients because the treatment period was longer and the strength of water was higher than previous study. 21
A significant reduction in the TC and LDL-c was shown at week 8 compared with the baseline in the RDSW group. Of note, in the RDSW group, the decline in both TC and LDL-c was consistent throughout the study, whereas in the placebo group, these two parameters decreased until week 4 and then increased up to the week 8. This is in agreement with a previous trial evaluating the effect of consumption of RDSW on hypercholesterolemic patients for 6 weeks where both parameters decreased proportionally to the progression of treatment. 21
Because this study was a clinical trial using food, stratification analysis was also attempted according to the disease severity at baseline. Our results showed that at week 8, TC level was significantly reduced from the baseline in both the subgroups of the RDSW group. In particular, such decline of TC in the high TC subgroup was ∼4 times higher than that in the moderately high TC subgroup. Moreover, a significantly lower level of LDL-c was observed in the high LDL-c subgroup of the RDSW group, but not of the placebo group, at the 8th week compared with that at baseline. Taking all in consideration, it is conceivable that RDSW has a greater beneficial effect on both the TC and LDL-c high groups than the moderately high groups.
A number of studies have been conducted to understand the mechanisms by which RDSW improves cholesterol profiles. Administration of RDSW for 6 weeks in HFD-fed hamsters increased the gene expression of LDL-c receptor and cholesterol-7a-hydroxylase, playing a vital role in cholesterol metabolism. Moreover, consumption of RDSW also enhanced the fecal output of cholesterol and bile acid, 22 contributing to a decreased cholesterol burden. These findings are also consistent with a previous study where treatment of HFD-fed rats with RDSW for 6 weeks increased the fecal excretion of cholesterol and also upregulated the expression of genes associated with lipolysis and fatty acid oxidation. These genes include AMP-activated protein kinase, peroxisome proliferator-activated receptor α, carnitine palmitoyltransferase (CPT)-1, and acyl-CoA oxidase (ACO) in the liver and adipose TG lipase, hormone-sensitive lipase, CPT-1, and ACO in the adipose tissues. 23
Our RDSW formulation is enriched with minerals such as sodium, Mg, and Ca, among which Mg is the most abundant. Mg can reduce cholesterol concentrations and prevents atherosclerosis and CVDs. In a previous study, administration of saturated fat enriched diet-fed rabbits with Mg inhibited cholesterol accumulation in the artery walls and increased fecal output of lipids. 24 Mg has also been shown to control enzymatic activities and transcriptional expression of genes related to lipid metabolism, reducing hepatic lipid accumulation. 25 Moreover, as divalent cations, both Mg and Ca can form insoluble compounds with fatty acids or bile acids in the intestine, thus preventing the absorption of the dietary fat. Such an event ultimately promotes intake of LDL-c in the liver and impedes formation of very LDL-c. 26,27
Previous studies have also reported that the mortality rates from CVD are negatively correlated with water hardness. 28 DSW with a water hardness of 1430 ppm was found to be more beneficial than DSW with a water hardness of 1410 ppm. 21 The RDSW used in this study has a strength of 2387 ppm, so it can be deduced that it has a beneficial effect on CVD.
The HDL-c did not differ significantly between groups or over time in this study. In this respect, DSW is distinguished from dyslipidemic drugs, which decreases LDL-c and HDL-c at the same time. 29 The TC:HDL-c ratio and LDL-c:HDL-c ratio are regarded as indicators of risk factors for ischemic heart disease. 30 After intervention, the LDL-c:HDL-c ratio was decreased in both the placebo and RDSW groups, although not in a significant manner. Although the ratio of HDL-c to TC was significantly increased in the RDSW group at the 8th week compared with the baseline, there was no significant difference between the groups. Therefore, when using RDSW to treat dyslipidemia, cholesterol levels should be targeted rather than TG.
An increase in apo A1 is associated with an improvement in the cardiovascular function. 31 In our study, significant reduction in the level of apo A1 was observed in the placebo group but it was unchanged in the RDSW group at week 8 compared with baseline. Apo B is present in all lipoproteins associated with atherosclerosis, including LDL-c and therefore, a reduction in its level has beneficial impact on the cardiovascular system. 32 In this study, a decline in this protein was evident from the baseline to 8th week in both groups, although such changes were found to be insignificant. Moreover, the apo B:apo A1 ratio, which is used to predict atherosclerosis, 33 showed a decreasing trend in the RDSW group from baseline to week 8. Therefore, it is conceivable that RDSW has some beneficial impact on the apolipoproteins. On the contrary, Lp(a), consisted of an LDL-c like core containing apo B, is generally considered to be a risk factor for CVD because of its prothrombotic effects. 34 In our study, Lp(a) was significantly decreased in the RDSW group throughout the study, indicating that the RDSW has anti-atherogenic effect.
No significant changes in hematology, blood chemistry, or urine parameters were observed during the study except for BUN. However, such difference of BUN is not clinically significant because the BUN in the RDSW group was found to be within the normal range throughout the trial. Therefore, RDSW does not affect the liver and kidney function.
This study excluded risk groups with dyslipidemia, including diabetes and peripheral vascular diseases, and it screened the subjects based solely on TC levels that might include subjects within normal range of HDL-c, LDL-c, or TG. Therefore, it is difficult to apply the results of this study to all patients with dyslipidemia in clinical practice.
In conclusion, subjects with hypercholesterolemia who took RDSW for 8 weeks showed significantly lower LDL-c and Lp(a) than the placebo group while maintaining the HDL-c level. These results can be used to facilitate development of DSW as a personalized cholesterol-lowering functional food.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported financially by the National R&D project of “Development of new application technology for deep seawater industry” supported by the Ministry of Oceans and Fisheries of the Republic of Korea. The funding sponsor had no role in the study design, data collection, interpretation and analysis, writing of the article, or decision to publish the results.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.