
Abstract
The use of herbarium mixture has been empirical, and the properties are not yet known. The aim of this study was to evaluate the effect of oral administration of herbarium mixture (Guazuma ulmifolia [G. ulmifolia]/Tecoma stans [T. stans]) on metabolic profile in patients with type 2 diabetes mellitus (T2DM). A randomized, double-blind, placebo-controlled, clinical trial was carried out in 40 patients with T2DM. They were between 40 and 65 years of age, with body mass index (BMI) between 25.0 and 34.9 kg/m2 and HbA1c >7.0%. BMI, waist circumference, fasting glucose, HbA1c, lipids, kidney, and liver function were measured. The patients were randomly assigned to receive the herbarium mixture (G. ulmifolia/T. stans) 400 mg before each meal, or placebo for 90 days. Herbarium mixture group showed decreased waist circumference (99 ± 14 vs. 98 ± 15 cm; P = .019), fasting glucose (12.0 ± 5.7 vs. 10.3 ± 5.1 mM; P = .019), and HbA1c (9.9% ± 2.7% vs. 8.9% ± 2.5%, P = .002). In conclusion, the administration of herbarium mixture (G. ulmifolia/T. stans) improved the glycemic profile in patients with T2DM. ClinicalTrial registration: NCT03313856 ClinicalTrials.gov
BACKGROUND
Type 2
There are drugs available for T2DM to control glucose levels; however, only one-third of the patients achieve their goals, and even fewer maintain them over time. 3
Thus, many diabetic patients draw upon many strategies to improve their glucose levels. In Mexico, medicinal plants are widely used; almost 5000 species of plants exist and are used medicinally.
About 300 species have records of popular use in the treatment of T2DM in Mexico. However, limited data are available, but based on our field experience in diabetic patients, they practically always use plants with or without medical prescription. 4
According to the Zapotecs healer Indians in Mexico, species with astringent properties such as G. ulmifolia and therefore, high levels of tannins, were considered particularly useful medicinal plants for the treatment of gastrointestinal diseases. 5
G. ulmifolia belongs to the Sterculiaceae family with medical uses in vaginal infection, diabetes, and washing of wounds. 6
On the contrary, T. stans (Bignoniaceae) is another herbal medicine derivative that is also known and used for the control of glucose in people with T2DM. Encouraging results of hypoglycemic action have been observed. 7
In the murine 3T3-F442A preadipocyte cell line, G. ulmifolia exerts its antidiabetic effects by stimulating glucose uptake in both insulin-sensitive and insulin-resistant adipocytes without inducing adipogenesis, 8 and hydroalcoholic extracts of T. stans has been shown to reduce carbohydrate and lipid digestion and absorption, by an inhibitory effect on glucosidase and lipase enzymes, 9 with the possibility of a synergistic effect. Thus, this mixture represents a social heritage and the understanding of local folk medical systems here in Mexico. 10
In Mexico, there is a combination of G. ulmifolia and T. stans to lower glucose levels; however, the effect on plasma glucose concentrations in patients with T2DM is unknown.
The purpose of this study was to analyze the effect of oral administration of herbarium mixture of G. ulmifolia/T. stans on metabolic profile in patients with T2DM.
RESEARCH DESIGN AND METHODS
A randomized, double-blind, placebo-controlled clinical trial was carried out in 40 patients with T2DM, independently of their basal antidiabetic treatment. Patients were between 40 and 65 years of age, with body mass index (BMI) between 25.0 and 34.9 kg/m2, HbA1c >7%, blood pressure <130/85 mmHg, triglycerides <4.0 mM, creatinine <132.6 μM, and <5 years from the diagnosis of diabetes. Besides, they should not have a chronic or acute history of renal, hepatic, thyroid, or endocrine diseases at study entry. Patients with a history of hospitalizations or symptoms of decompensation associated with diabetes (hypoglycemia or hyperglycemia) in the 6 months before study entry were not admitted. All patients had maintained a stable weight for at least 3 months before the study onset. All patients took their previous drug regimen steadily for at least 3 months before study entry. The medication was allowed for the treatment of diabetes, but access to those containing derivatives of herbal products was restricted. All patients were selected from Guadalajara city, Mexico and they belonged to the same socioeconomic stratum.
At the beginning and the end of the study, BMI, waist circumference, and metabolic profile (fasting glucose, HbA1c, lipids) were measured; and to verify that there was no clinical contraindication to receive the nutraceuticals or the appearance of side effects at the end of the intervention, creatinine, uric acid, aspartate transferase (AST), and alanine transferase (ALT) were determined. The laboratory test to determine serum glucose was the glucose-oxidase technique (Merck México), with an intra- and interassay coefficient of variation of <3%. For determination of HbA1c percentage, ion-exchange high-performance liquid chromatography was carried out (Bio-Rad Laboratories, Hercules, CA, USA) with an intra-assay coefficient of variation of 2.8% and 3.5% and interassay coefficient of variation of <3.0%. Creatinine, uric acid, lipid profile (TC, HDL, and TG), AST, and ALT were measured enzymatically (ERBA Mannheim XI 100) with an intra- and interassay coefficient of variation of <2%, low-density lipoprotein cholesterol (LDL-c) was estimated by the Friedewald formula (LDL-c = TC − HDL-c − TG/5), and very low-density lipoprotein cholesterol (VLDL-c) with the TG/5 equation. Insulin concentration was measured using the microparticle enzyme immunoassay method (ELISA AccuDiag™- DIAGMEX) with an intra- and interassay coefficient of variation of 3.3% and 3.8%, respectively.
All the tests were carried out at 08:00 am after 12-h overnight fast at the Institute of Experimental and Clinical Therapeutics, Department of Physiology, University Center of Health Science, University of Guadalajara, Mexico.
Selection criteria were evaluated, and a complete physical examination was performed. Height and weight were measured with subjects wearing lightweight clothing and no shoes. BMI was calculated with the weight (kg) divided by the height squared (m2). Blood pressure was evaluated using a fully automated device (OMROM HEM-781INT) after a resting period of 5 min with the individual sitting in a chair; systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate were recorded simultaneously. A venous blood sample was taken to measure serum glucose, creatinine, total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), LDL-c, and triglyceride (TG) concentrations. After 90 days of G. ulmifolia/T. stans or placebo administration, the same clinical and laboratory procedures were carried out.
GROUPS AND BLINDING PROCEDURES
Two study groups of 20 patients each and diagnosed with T2DM with or without nutraceutical intervention were formed; patients were randomly assigned to the corresponding group with the closed envelope technique. Each envelope contained a double-blind code with the intervention group and intervention number, and the patient selected an envelope. The groups were formed as follows: G. ulmifolia/T. stans group: G. ulmifolia (300 mg) plus T. stans (100 mg) = 400 mg per capsule; placebo group: calcined magnesia 400 mg per capsule. Both capsules were of the same organoleptic characteristics. The random allocation sequence was generated by an Excel program.
Intervention
The patients were randomly assigned to receive the herbarium mixture (G. ulmifolia/T. stans) or placebo (calcined magnesia), one capsule before each meal for 90 days. All patients received medical nutritional guidance according to the American Diabetes Association (carbohydrates consumed should be low glycemic load and come primarily from vegetables, the fat and proteins consumed should primarily come from plant sources) and maintain the same physical activity that was part of their daily routine to avoid interfering with the results. The herbarium mixture was obtained through vendor Quiminet and La Flor Azteca (
ETHICAL CONSIDERATIONS
All participants gave informed consent for participation in the study. The protocol was approved by the Ethics and Investigation Committees of University Center of Health Sciences of University of Guadalajara, with registry number DF/CB037/15 and met all requirements for investigations in human beings under the ethical standards of the responsible committee on human experimentation and with the Declaration of Helsinki of 1975, as revised in 2008.
Statistics
The sample size was calculated through a formula for clinical trials with a statistical confidence of 95%, the statistical power of 80%, standard deviation (SD) for HbA1c 1.3%, and an expected difference of at least 1.7% SD of HbA1c between groups, obtaining a total of 20 patients in each group that included 20% of the expected loss in the follow-up period. Data were reported as mean and SD for quantitative variables and frequencies for qualitative variables. The inferential analysis was performed with the chi-squared test. The Wilcoxon signed-rank test was used to compare intragroup differences and the Mann–Whitney U-test was used to compare between-group results. Data were analyzed with SPSS-20.0 software (SPSS, Inc., Chicago, IL, USA) and a value of P ≤ .05 was considered statistically significant.
RESULTS
The consort diagram and follow-up information are given in Figure 1. In the placebo group, 10% of patients were without pharmacological treatment, 60% were taking oral antidiabetic agents, and 30% were on insulin. In the G. ulmifolia/T. stans group, 20% were without treatment, 40% were taking oral antidiabetic agents, and 40% were on insulin. Women constituted 80% of the placebo group versus 70% of the G. ulmifolia/T. stans group, and men accounted for 20% versus 30%, respectively; no statistically significant differences were found when the chi-squared test was used (P = .716). No significant differences were observed in the clinical characteristics or demographics between the two groups in the baseline preintervention.

Consort diagram reflecting the flow of study participants.
In the placebo group, significant changes were found between values after intervention for total cholesterol (4.9 ± 0.8 vs. 5.4 ± 0.8 mM, P = .050). No changes were observed in weight (75.9 ± 15.2 vs. 75.2 ± 19.3 kg, P = .440); waist circumference (101 ± 10 vs. 100 ± 13 cm, P = .359); SBP (120 ± 11 vs. 122 ± 12 mmHg, P = .735); DBP (77 ± 7 vs. 76 ± 7 mmHg, P = 1.000); glucose (10.5 ± 3.6 vs. 9.8 ± 2.7 mM, P = .327); and HbA1c (9.0% ± 1.5% vs. 8.7% ± 1.3%, P = .612). There were no changes in the rest of the clinical and laboratorial parameters.
In the G. ulmifolia/T. stans group significant changes were found in values after the nutraceutical intervention in waist circumference (99 ± 14 vs. 98 ± 15 cm, P = .019); fasting glucose (12.0 ± 5.7 vs. 10.3 ± 5.1 mM; P = .019); HbA1c (9.9% ± 2.7% vs. 8.9% ± 2.5%, P = .002); AST (28 ± 18 vs. 19 ± 11 IU/L, P = .012); and ALT (33 ± 22 vs. 22 ± 15 IU/L, P = .021), as given in Table 1. No changes were observed in weight (75.8 ± 18.9 vs. 73.1 ± 22.2 kg, P = .213). There were no changes in any other measurements.
Comparison of Metabolic Profile in the G. ulmifolia/T. stans Combination Group
P: Mann–Whitney U-test.
HDL, high-density lipoprotein; LDL, low-density lipoprotein; VLDL, very low-density lipoprotein; AST, aspartate aminotransferase; ALT, alanine aminotransferases.
When comparing the change (Δ) between the placebo and G. ulmifolia/T. stans groups, some significant differences were observed in glucose (1.2 ± 2.4 vs. −2.3 ± 3.7 mM, P = .010, Fig. 2) and HbA1c (−0.05% ± 0.8% vs. −1.2% ± 1.1%, P = .020, Fig. 3), respectively.
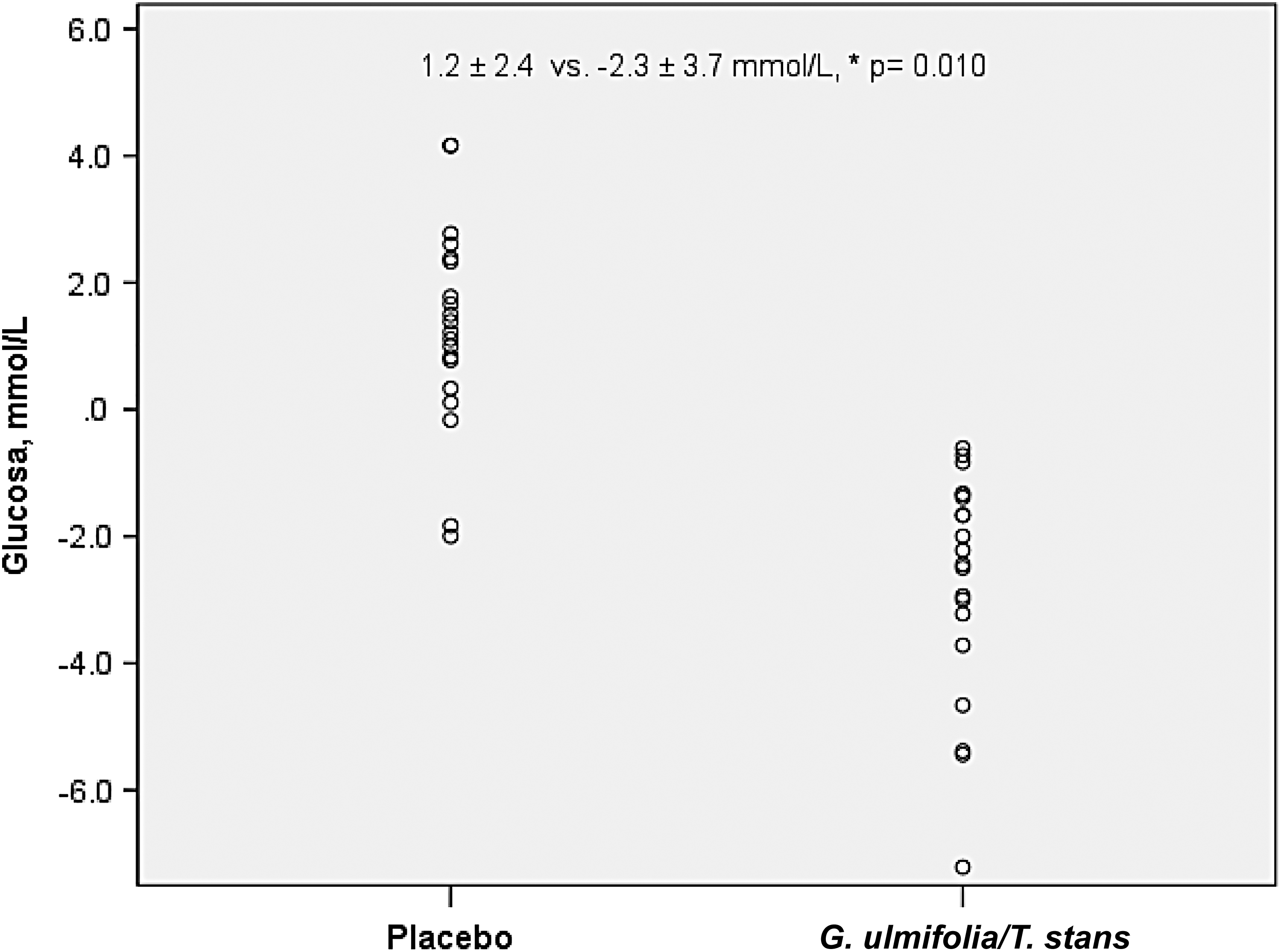
Delta comparison of glucose levels between groups. *P = .010 with the Mann–Whitney U-test. G. ulmifolia/T. stans, Guazuma ulmifolia/Tecoma stans.
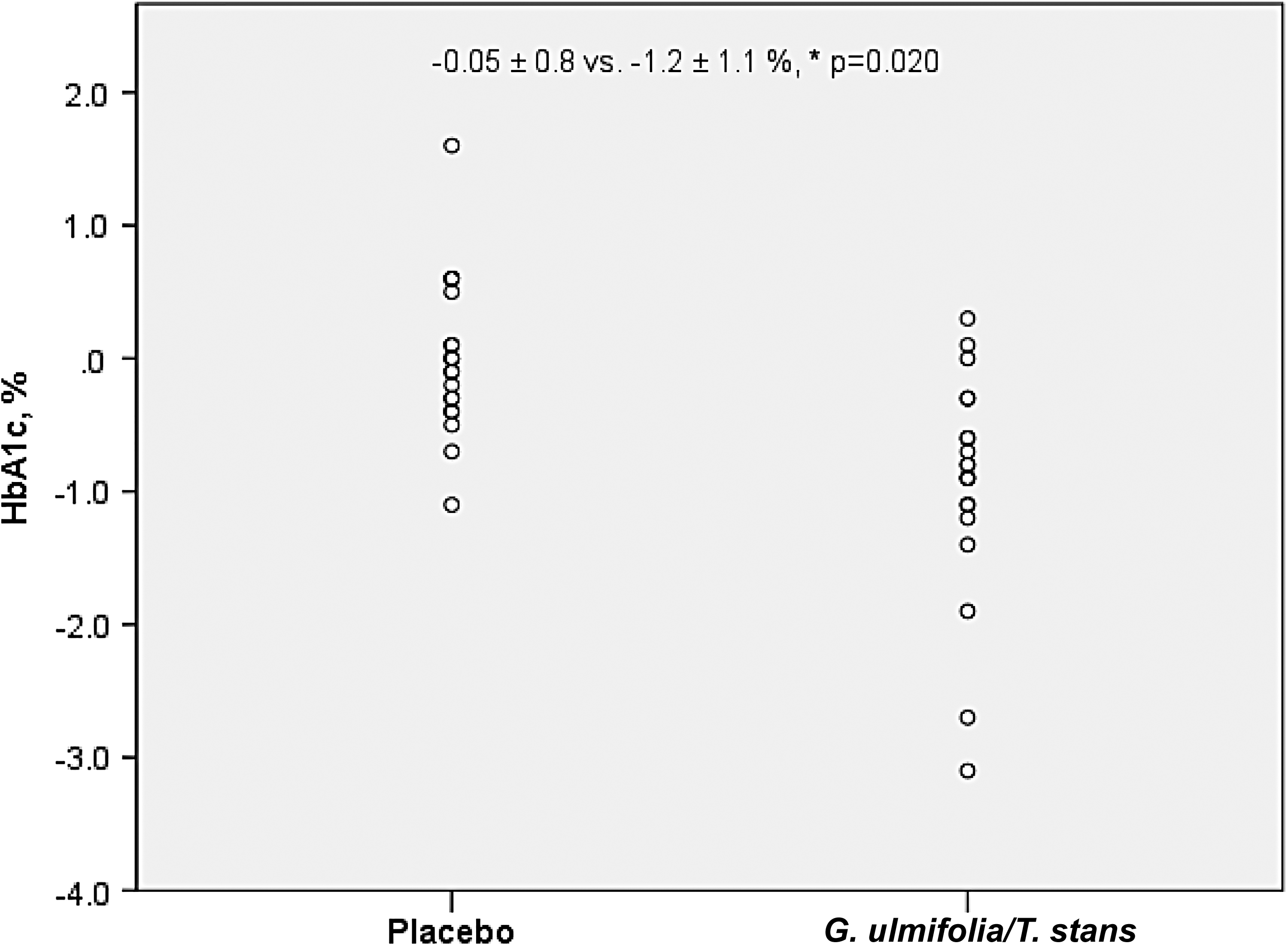
Delta comparison of HbA1c percentage between groups. *P = .020 with the Mann–Whitney U-test.
In both groups, no serious adverse events were reported after the intervention period of 90 days.
DISCUSSION
In this study, although at the end of the intervention, the patients in the G. ulmifolia/T. stans group did not achieve the goal of glycemic control, there was a statistically significant decrease in HbA1c, this reduction in the percentage of glycosylated HbA1c was >1%, which represents an important finding, as we have observed both in the UKPDS as in the DCCT, a reduction ≥1% represents the possibility of delaying the progression of both micro and macrovascular complications ∼30–35%. 11,12 Likewise, the change in fasting glucose concentration is clinically significant, and it could mostly be related to the decrease in IR present in the adipocyte.
These results are consistent with a report by Alonso-Castro and Salazar-Olivo, who described the antidiabetic mechanisms of G. ulmifolia in 3T3-F442A preadipocytes with insulin-sensitive and insulin-resistant adipocytes, in which a 40% increase in glucose uptake in sensitive adipocytes was reported and 24% of adipocytes were resistant to insulin without inducing adipogenesis. 8 In that same sense, Alarcon-Aguilar et al. in a study on rabbits reported a 22% decrease in serum glucose after the administration of G. ulmifolia; in the same study, the antidiabetic effect of T. stans induced a decrease in serum glucose of 17.5% compared with placebo, and both interventions were followed by a hyperglycemia-induced glucose tolerance curve by subcutaneous route. 9
Ramírez et al., in an in vitro study, reported the inhibition of α-glucosidase by 23% after treatment with G. ulmifolia and 32% in the group to which T. stans was applied. 13 According to previous studies, both the improvement in IR in peripheral tissues and adipose tissue and the inhibition of α-glucosidases could be the mechanisms of action that are involved in the decrease in serum glucose and therefore in the percentage of HbA1c after the administration of these two phytopharmaceuticals. Besides, Eddouks et al. reported that both G. ulmifolia and T. stans can separately decrease fasting glucose by increasing phosphatidylinositol (PI3K) kinase 3 and insulin receptor substrate 1 (IRS-1) activity. PI3K and IRS are key pathways in fat cells that, under conditions without IR, can stimulate the expression, translocation, and release of GLUT4 necessary to introduce extracellular glucose into the intracellular space and proceed to metabolism. Both PI3K and IRS are decreased in patients with DM2 with IR, and it has been reported that the phytopharmaceuticals used in this study could increase the stimulation of PI3K and IRS and thus decrease the glucose levels. 14
In addition, G. ulmifolia/T. stans independently have been shown to improve insulin sensitivity through the stimulation of gamma receptors that are activated by peroxisome proliferators (PPARY). When PPAR is stimulated, insulin sensitivity is enhanced by the activation of a nuclear factor that regulates the transcription of genes involved in glucose and lipid metabolism and thus decreases serum glucoseconcentration. 13
We also observed a decrease in the serum concentration of AST and ALT in the G. ulmifolia/T. stans group despite these measurements remained within normal parameters. The effect of the G. ulmifolia/T. stans combination on the liver is unknown, but it has been reported that some of the mechanisms of action of phytopharmaceuticals may be through the PPAR stimulation in the liver, and it is possible that this effect could contribute to the decrease in the concentration of serum levels of transaminases. In addition, the use of antidiabetic plants to decrease serum glucose stimulates the GLUT-2 insulin-independent glucose transporter and could exert an effect on the liver, beta cells of the pancreas, kidney, and small intestine, although the effect that GLUT-2 could exert on the serum concentration of transaminases is unknown. 10,13
Although the effect of G. ulmifolia and T. stans on IR in hepatic tissue is unknown, they could have an effect similar to that already reported in adipose tissue. There are reports of studies performed on streptozotocin-induced diabetic mice with other medicinal plants such as Anoectochilus roxburghii, a plant of Chinese origin that was shown to induce a decrease not only in serum glucose but also in AST, ALT, and oxidative stress. 15 Some other studies also report the hepatoprotective effect of medicinal plants. 16 –18
A statistically significant difference was observed in the G. ulmifolia/T. stans group in waist circumference after the nutraceutical intervention period. This reduction in waist circumference could be added to the possible effect of PPARs and GLUT-2 transporters, because according to reports in the literature also there could be changes in glucose and hepatic enzymes with the accumulation of ectopic lipids that have been associated with alterations in the storage of glycogen, which is a hallmark in metabolic diseases and nonalcoholic fatty liver. 19
In conclusions, the administration of herbarium mixture G. ulmifolia/T. stans improved the glycemic profile in patients with T2DM.
This clinical trial opens the possibility of using the combination of G. ulmifolia/T. stans as a useful agent to decrease glucose and HbA1c consequently in patients with T2DM and supports the traditional use of these phytopharmaceuticals for the treatment of T2DM. It is necessary to continue this kind of clinical trials with larger samples sizes for longer periods to know their effectiveness and long-term safety.
Footnotes
AUTHOR DISCLOSURE STATEMENT
All authors disclose there are no actual or potential commercial associations that might create a conflict of interest in connection with this article.
FUNDING INFORMATION
This study was supported by the University of Guadalajara, México.