
Abstract
Symptom-alleviating therapies for osteoarthritis (OA) management are inadequate. Long-term application of first-line treatments, such as nonsteroidal anti-inflammatory drugs, is limited due to associated side effects. We believe that a combination of traditionally used botanical extracts, which have diverse active components that target multiple inflammatory pathways, may provide a safe and efficacious alternative to address the multifactorial nature of OA. Recently, cannabidiol (CBD), the major nonpsychoactive component of the hemp plant, has gained renewed global attention for its pharmacological actions. It has shown promise in reducing pain and inflammation in preclinical models of arthritis. In this study, widely employed inflammatory and noninflammatory animal pain models, such as the hot plate test, visceral pain model (writhing test), and carrageenan-induced rat paw edema model, were utilized to evaluate the antinociceptive and anti-inflammatory activity of CBD alone and in combination with standardized bioflavonoid compositions. CBD was tested at 5, 10, 20, and 40 mg/kg orally and at 5% topically. Administered alone, CBD produced dose-correlated, statistically significant pain inhibition in all the models. Enhanced performance in pain and inflammation reduction was observed when CBD was orally administered in complex with the bioflavonoid compositions. Data from this study show that for clinically meaningful efficacy against OA, CBD may have to be delivered in higher dosage or formulated with other medicinal plants with similar activities.
Introduction
Osteoarthritis (OA)
Cannabis has been used for many years as a medicinal plant for a wide variety of indications, including for pain relief. It contains hundreds of pharmacologically active, structurally similar phytocannabinoids. The predominant psychotropic component of Cannabis is Δ 9 -tetrahydrocannabinol (Δ 9 -THC), and the major nonpsychoactive component is CBD. Since hemp (Cannabis sativa plant) with less than 0.3% THC content was removed from the list of controlled substances in the 2018 USA Farm Bill (H.R.5485; Hemp Farming Act of 2018), CBD has gained renewed global attention for its nutritional benefits. Its pharmacological actions include anti-inflammatory and anti-nociceptive effects which are independent of cannabinoid receptors and hence without psychotropic side effects. Several in vitro and in vivo studies have shown the anti-inflammatory and antinociceptive activities of CBD, suggesting its potential clinical efficacy for osteoarthritic pain. One mechanism by which CBD relieves pain has been suggested to be its activation of transient receptor potential vanilloid type 1 (TRPV1) and transient receptor potential ankyrin 1 (TRPA1). These receptors play critical roles in OA pathology, and their activation, and subsequent desensitization, is thought to abate pain. CBD was found to be an agonist for these receptors in vitro, possibly explaining its analgesic activity. 3,4 In vivo, orally administered CBD suppressed the progression of collagen-induced arthritis by reducing inflammatory cytokine production, reducing cartilage degradation and joint inflammation. 5 A study showed that CBD blocked arthritis-associated pain locally when applied topically and systemically in an monoiodoacetate (MIA)-induced arthritis disease model in rats, 6 and similarly, in a complete Freund's adjuvant-induced monoarthritic knee joint rat model, transdermal CBD provided pain relief and reduced inflammatory cell infiltrates into the joint tissues, while bypassing its poor oral bioavailability. 7 Collectively, these activities of CBD are clear indications of its potential application in arthritis management alone or in combination with other medicinal plant compositions.
Previously, we reported that UP446, a bioflavonoid composition derived from the standardized extracts of Scutellaria baicalensis root and Acacia catechu heartwood, possesses activities suggestive of benefits in OA, including dual inhibition of proinflammatory cyclooxygenase and lipoxygenase pathways, 8 modulation of cyclooxygenase (COX)-2, tumor necrosis factor-α, interleukin (IL)-1β, IL-6, and nuclear factor-κB gene expression, 9 and inhibition of COX-2, 5-Lipooxygenase (LOX), and inducible-nitric oxide synthase protein expression in Lipopolysaccharide (LPS)-stimulated rat peritoneal macrophages. 10 Alleviation of OA-related pain symptoms has also been reported for UP446 from a series of human clinical trials. 11,12
Similarly, extracts of medicinal plants A. catechu heartwood and Morus alba root bark were formulated to yield a standardized bioflavonoid composition, known as UP1306. The bioflavonoid composition has been tested in vitro and in vivo and showed beneficial effects in OA such as antinociceptive and anti-inflammatory properties, 13 COX and LOX modulation, 13 inhibition of glycosaminoglycan release from cartilage explants, 14 cartilage sparing, 14 reduction of proinflammatory cytokines, and inhibition of matrix degrading enzymes. 15 In randomized and double-blind placebo-controlled clinical trials, UP1306 administered at 400 mg/day showed a significant reduction in urinary C-telopeptides of type II collagen (CTX-II), a degradation product of articular cartilage in arthritic patients, 16 after 12 weeks of supplementation, and reduced delayed-onset muscle soreness in healthy runners following 9 weeks of supplementation. 17
Given these facts, we hypothesized that the co-administration of CBD with bioflavonoids would be beneficial, leading to complementary mechanisms of action and lowered dosages needed for equal symptom relief from each material. In this study, we tested this hypothesis in animal models of pain and inflammation. Carrageenan-induced paw edema model, writhing test (abdominal constriction test), and a hot plate test model were used to evaluate the antinociceptive and anti-inflammatory activities of CBD alone and in combination with UP1306 and UP446.
Materials and Methods
Test materials
CBD isolate (contains 101.04% CBD by weight) and full-spectrum CBD distillate (contains 3.19% THC, 68.69% CBD, 1.18% cannabigerol [CBG], and 0.84% cannabidivarine [CBDV] by weight) were purchased from Factory6, Inc. (American Fork, UT, USA) and certificates of analysis were provided by Botanacor Laboratories (Denver, CO, USA). CBD crude extract (contains 2.09% THC, 49.09% CBD, 0.54% CBG, 1.83% Cannabichromene [CBC], 0.2% Cannabinol [CBN], and 0.48% Cannabidiolic Acid [CBDA] by weight) was purchased from Commonwealth Extracts LLC (Louisville, KY, USA). CBD isolate, full spectrum and crude extract were purchased from state-approved vendors. Preparation of materials follows the disclosed companies' protocols. Dosage selection for this study was exploratory within the context of previously reported usage of CBD as in Malfait et al. 5 and Philpott et al. 6 UP446 (not less than 60% baicalin and 10% catechins) and UP1306 (not less than 2% mulberroside A and 15% catechins) were obtained from Unigen, Inc.
Animals
Sprague Dawley rats and CD-1 mice were purchased at the age of 8 weeks. Animals were acclimated for 1 week before being assigned to groups. Cage cards indicating project number, test article, dose level, group, and animal numbers for identification were used for each group. Bedding (soft cob) was changed twice per week. Animals were provided with fresh water and rodent chow ad libitum and housed in a temperature-controlled room (22.2°C) on a 12-h light/12-h dark cycle. All animal experiments were conducted according to the institutional guidelines congruent with guide for the care and use of laboratory animals.
Hot plate test
Repeated application of anti-inflammatory compounds or extracts topically at the site of thermal contact (noxious stimulus) may cause desensitization of the peripheral afferent pain receptors and produce a delay in response time. A longer change in reaction time could be interpreted as an antinociceptive effect of the applied compound. To evaluate this hypothesis, rats (N = 10/group) received CBD isolate formulated at 5% concentration topically on their right hind paw. This concentration was selected based on Goudarzi et al. 18 and Trnavský et al. 19 As the rate of absorption, the amount absorbed, and penetration depth affect the outcome of the topically applied preparation, we rubbed/massaged each paw at least 60 times using our index finger until the applied content appeared visually absorbed. This procedure was repeated thrice every 30 min before placing the animals onto a preheated hot plate set at 53°C. Paw withdrawal latency was calculated as the time elapsed from the initial placement of the rat onto the hotplate to withdrawal (or licking or shaking) of the hind paw in response to the thermal stimulus. The animal was immediately removed when this response was observed. For those who failed to display a response within 30 sec, they were removed from the hot plate to prevent tissue damage. Experimental design included Group I—vehicle only (negative control); Group II—ibuprofen (5%, positive control); and Group III—CBD (5%).
Writhing test
The antinociceptive effects of CBD isolate, full spectrum and CBD-containing crude extract were evaluated in CD-1 mice. Mice were gavaged with the disclosed test materials an hour before intraperitoneal injection of 0.7% acetic acid at 10 mL/kg using 26-gauge needles and syringes. Test materials were dissolved in propylene glycol (PG) and administered orally at 100 mg/kg. The vehicle-treated mice received PG only. The experiment was carried out at room temperature and mice were acclimated before the procedure. Six animals were allocated for each treatment group. Following the challenge, each animal was placed back into its own individual section of the observation chamber and the number of constrictions of the abdominal muscle was counted over a period of 30 min. 20
Carrageenan-induced rat paw edema model
Inflammation was induced by intraplantar injection of 0.1 mL λ-carrageenan suspended in saline (Sigma, St. Louis, MO, USA) into the plantar surface of the left hind paw. Rats were sedated with isoflurane at the time of injection. Rats were acclimated in a procedure room before measurements. Mechanical allodynia was evaluated using a Randall–Selitto test, or paw pressure test, on the central plantar surface of the right hind paw. After application of the pressure stimulus, sharp withdrawal of the paw was considered a positive response and recorded by an electronic Von Frey Anesthesiometer (2390 series Electrovonfrey; IITC, Woodland Hills, CA, USA). 21 These measurements were taken before carrageenan inoculation (T0), and after 1, 2, 4, and 6 h. Paw edema was measured with the use of a Plethysmometer (IITC; Model 520) at time 0 (before carrageenan), 1, 2, 4, and 6 h after carrageenan injection. Animals (N = 5/group) were orally gavaged with a positive control ibuprofen (lot no. ZG0097; Spectrum Chemical MFG, Gardena, CA, USA) at 100 mg/kg. For the combination study, rats were treated with UP1306 at 120 mg/kg + CBD at 30 mg/kg; UP446 at 135 mg/kg + CBD at 15 mg/kg; and UP1306 at 85 mg/kg + UP446 at 50 mg/kg + CBD at 15 mg/kg. All doses were administered 1 h after carrageenan inoculation. CBD was tested for efficacy alone at oral doses of 5, 10, 20, and 40 mg/kg.
Statistical analysis
Data were analyzed using SigmaPlot (Version 11.0; Systat Software, Inc., San Jose, CA, USA). The results are represented as mean ± standard deviation. Statistical significance among groups was calculated by means of single-factor analysis of variance (ANOVA) and by t-test. P ≤ .05 (P ≤ .05) was considered statistically significant. When the normality test failed, for nonparametric analysis, data were subjected to Mann–Whitney sum ranks for t-test and Kruskal–Wallis one-way ANOVA on ranks for ANOVA.
Results
Topical antinociceptive activity of CBD
The antinociceptive activity of CBD was tested on a hot plate set to 53°C. Withdrawal reflex to a thermal stimulus is one of the natural protective mechanisms expressed by animals in times of danger. Rats were observed for pain signaling reactions of the hind paw, including lifting, biting, fluttering, and jumping. The time from placing the animal onto the hot plate until their reaction time was considered their pain resistance threshold or paw withdrawal latency. Due to the solubility characteristics of the compounds, two types of vehicles, Vehicle 1 = dimethyl sulfoxide (DMSO) + PG + Aloe (2%) and Vehicle 2 = DMSO + PG, were used. Percent changes and P values for statistical significance were determined using respective vehicles for each test material. As illustrated in Figure 1, rats with CBD isolate applied topically showed 38.4% increase in paw withdrawal latency compared to vehicle. This increase in antinociceptive activity observed was higher than what was observed for 5% ibuprofen (i.e., 22.4% increase in paw latency with a P value equal to .018 compared to the vehicle group). The observed increase in antinociceptive activity in the topical CBD group was statistically significant when compared to the vehicle control.
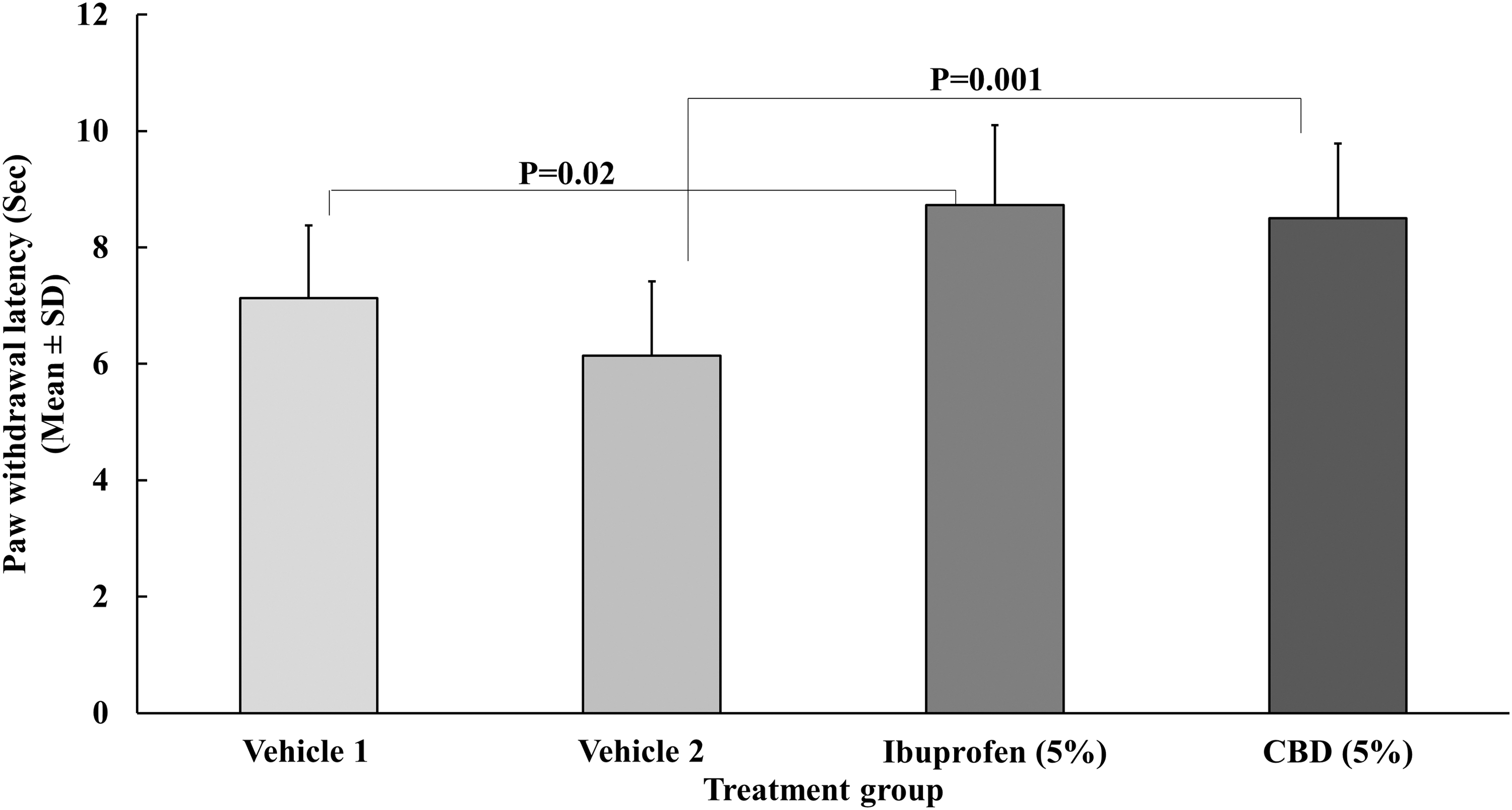
Antinociceptive activity of CBD applied topically at 5% concentration to the right hind paw of rats. Rats (N = 10/group) were placed on a preheated hot plate set at 53°C. The paw withdrawal latency was calculated as the time elapsed from the initial placement of the rat onto the hotplate to the withdrawal (or licking or shaking) of the hind paw in response to the thermal stimulus. Due to the solubility characteristics of the compounds, two types of vehicles, Vehicle 1 = DMSO + PG + Aloe (2%) and Vehicle 2 = DMSO + PG, were used. Percent changes and P values for statistical significance were determined using respective vehicles for each test material. CBD, cannabidiol; DMSO, dimethyl sulfoxide; PG, propylene glycol; SD, standard deviation.
Antinociceptive activity of CBD
Intraperitoneal injection of acetic acid (0.7%, 10 mL/kg) resulted in 55 ± 18.1 abdominal contractions for the vehicle control group within a duration of 30 min. Mice treated with single oral doses of CBD isolate, full-spectrum CBD distillate, and CBD crude extract showed varied degrees of reduction in the number of abdominal muscle constrictions exhibited compared to vehicle-treated animals (Fig. 2). The decrease in pain sensitivity seemed to correspond to the content of THC. The full-spectrum CBD distillate, containing 3.19% THC and 68.69% CBD by weight, showed the highest inhibition in pain sensitivity with 96.1% inhibition. The CBD crude extract, containing 2.09% THC and 49.09% CBD by weight, displayed a 34.2% inhibition of nociception. The CBD isolate, containing only CBD at 101.04% by weight and no THC content, showed a 28.8% inhibition of visceral pain sensitivity compared to the vehicle-treated control. The ibuprofen-treated mice showed 55.5% inhibition of nociception when compared to the vehicle control. Antinociceptive results from the full-spectrum CBD distillate and ibuprofen were statistically significant. A decrease in abdominal writhing is indicative of analgesia, which each treatment group experienced to some degree.

Antinociception effect of single oral dose cannabis extracts. Mice (N = 6/group) were given the respective treatments at 100 mg/kg an hour before intraperitoneal injection of 0.7% acetic acid. Data are reported as mean ± SE of the observed abdominal constriction for 30 min postinjection. *P ≤ .05; **P ≤ .001. SE, standard error.
Antinociceptive and anti-inflammatory activities of CBD
Antinociceptive and anti-inflammatory activity of CBD was tested in rats with carrageenan-induced paw edema. Upon intraplantar injection of carrageenan to the hind paw, cardinal signs of inflammation, such as swelling and hyperalgesia, were evident in all the rats. A single oral dose of CBD per animal produced dose-correlated inhibition of pain sensitivity and inflammation (Table 1). Compared to the vehicle group, the percent reductions in pain sensitivity for each group, as measured by paw withdrawal in response to stimulus, were as follows: 0.9–14.5% for 5 mg/kg CBD, 14.6–17.1% for 10 mg/kg CBD, 18.4–23.8% for 20 mg/kg CBD, and 22.3–45.6% for 40 mg/kg CBD. The percent reductions in inflammation for each group, as measured by the extent of paw edema, were as follows: 17.3–21.5% for 5 mg/kg CBD, 17.1–23.9% for 10 mg/kg CBD, 6.6–33.9% for 20 mg/kg CBD, and 30.3–46.1% for 40 mg/kg CBD at 1–5 h after treatment. Except in the case of the 5 mg/kg CBD at 1 h and 5 h after the carrageenan, all the percent reductions were statistically significant. The highest inhibition was observed for the rats treated with 40 mg/kg CBD isolate. At this dose, the inhibition of pain sensitivity and inflammation was comparable to the efficacy observed for the ibuprofen positive control at 100 mg/kg throughout the time points monitored, except 1 h after treatment, when the paw edema inhibition was higher for the CBD group (i.e., 30.5% ibuprofen and 46.1% CBD).
Dose-Correlated Inhibition of Pain and Inflammation as a Result of Single Oral Cannabidiol Isolate
Inflammation was induced by intraplantar injection of 100 μL carrageenan suspended in saline into the plantar surface of left hind paw. Animals (N = 5/group) were orally gavaged with a positive control ibuprofen at 100 mg/kg. CBD was tested for its efficacy administered at oral doses of 5, 10, 20, and 40 mg/kg administered an hour after carrageenan. Changes in pain sensitivity and paw edema were compared from baseline (T0) at 1 h (or 2 h after carrageenan), 3 h (or 4 h after carrageenan), and 5 h (or 6 h after carrageenan) after treatment. * P ≤ .05; † P ≤ .0001; N = 5/group. Values in parenthesis are % changes of vehicle that is antipain and anti-inflammatory activity of respective treatment group.
CBD, cannabidiol; SD, standard deviation.
Antinociceptive and anti-inflammatory activities of bioflavonoids in combination with CBD
The addition of UP446 and/or UP1306 to CBD increased the antinociceptive and anti-inflammatory activities of CBD. In the carrageenan-induced arthritis model, CBD administered alone at 40 mg/kg resulted in 42.7%, 45.6%, and 22.3% inhibition in pain sensitivity, as measured by paw withdrawal response to a stimulus, at 1, 3, and 5 h after treatment, respectively. The combination of CBD at 20% (30 mg/kg) with UP1306 at 80% (120 mg/kg) by weight produced 46.2%, 43.0%, and 20.7% reduction in pain sensitivity with statistical significance at 1, 3, and 5 h after treatment, respectively. When rats were treated with a combination of CBD at 10% (15 mg/kg), UP446 at 33% (50 mg/kg), and UP1306 at 57% (85 mg/kg) at a total dose of 150 mg/kg, they experienced 41.6%, 39.7%, and 17.5% reduction in pain sensitivity at 1, 3, and 5 h after treatment, respectively, when compared to vehicle (Fig. 3). These data showed that when CBD at 10–20% by weight was blended with either UP446 or UP1306 or a combination of the two, the result was enhanced antinociceptive activity.
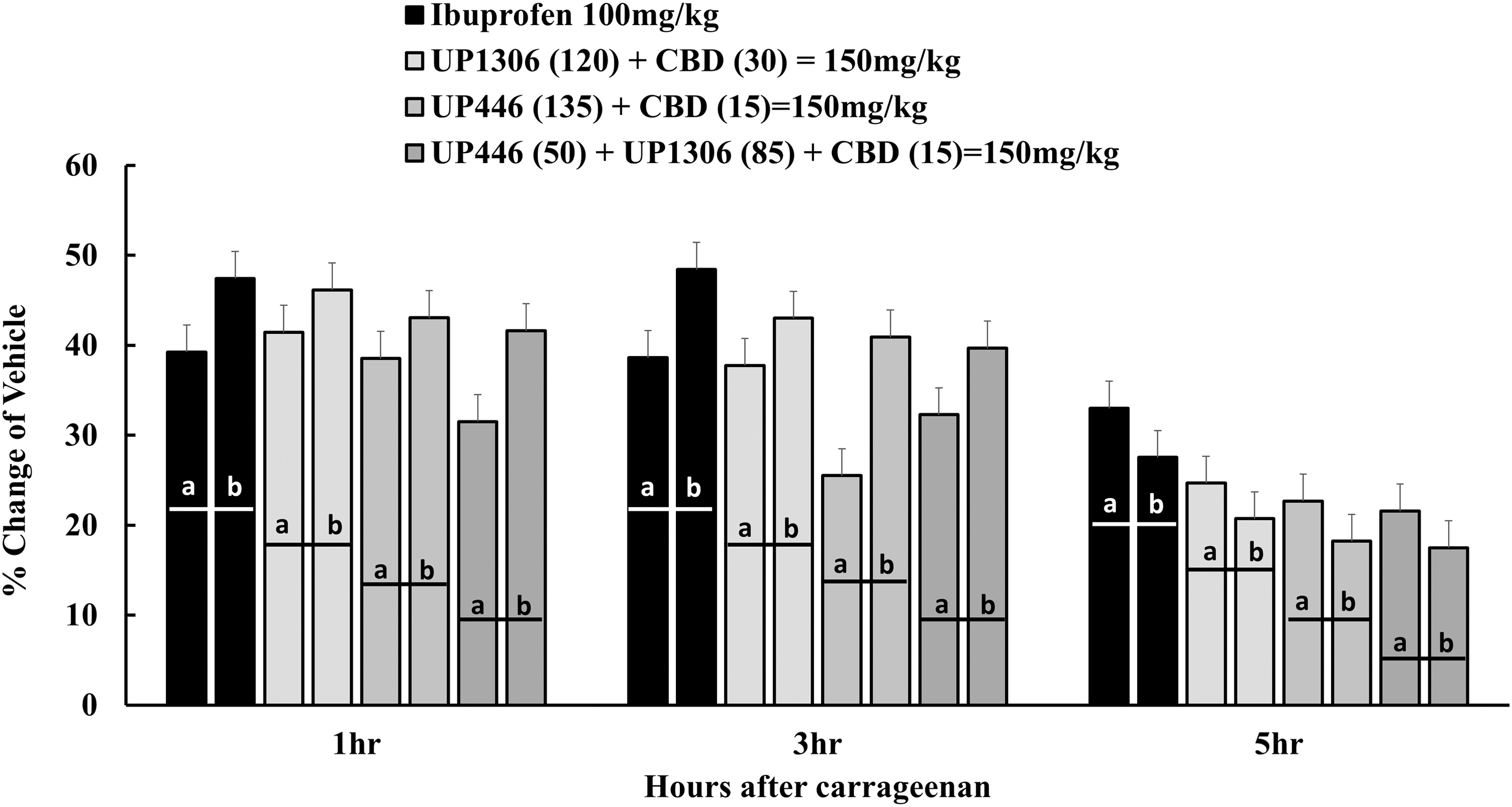
Anti-inflammatory and antinociceptive activity of CBD and/or CBD in combination with bioflavonoids in carrageenan-induced rat paw edema model. Inflammation was induced by intraplantar injection of 100 μL carrageenan suspended in saline into the plantar surface of left hind paw. Animals (N = 5/group) were orally gavaged with a positive control ibuprofen at 100 mg/kg. Rats were treated with UP1306 at 120 mg/kg + CBD at 30 mg/kg; UP446 at 135 mg/kg + CBD at 15 mg/kg; and UP1306 at 85 mg/kg + UP446 at 50 mg/kg + CBD at 15 mg/kg. All the doses were administered 1 h after carrageenan inoculation. Changes in pain sensitivity and paw edema were compared from baseline (T0) at 1 h (or 2 h after carrageenan), 3 h (or 4 h after carrageenan), and 5 h (or 6 h after carrageenan) after treatment. Percent inhibition in pain sensitivity and paw edema was statistically significant at each time point for all the treatment groups. a, b indicates a-anti-inflammation and b-antipain pair in order for the same treatment group.
Similarly, CBD administered at 40 mg/kg resulted in 46.2%, 44.7%, and 30.3% inhibition in paw edema, indicative of inflammation, at 1, 3, and 5 h after treatment, respectively. The addition of CBD at 20% (30 mg/kg) with UP1306 at 80% (120 mg/kg) produced 41.4%, 37.8%, and 24.7% reduction in paw edema with statistical significance at 1, 3, and 5 h after treatment, respectively. Rats treated with a combination of CBD at 10% (15 mg/kg), UP446 at 33% (50 mg/kg), and UP1306 at 57% (85 mg/kg) at a total dose of 150 mg/kg showed 31.5%, 32.3%, and 21.6% reductions in inflammation at 1, 3, and 5 h after treatment, respectively, when compared to vehicle (Fig. 3). The combination of CBD with UP1306 alone or UP446 and UP1306 together led to a lower requirement for CBD in the composition to result in similar nociceptive and inflammatory alleviation.
Discussion
OA pain and disease progression are inadequately managed in many patients because of the multifactorial nature of the disease. 22 When arthritic patients seek help for debilitating pain, they are left with limited options to curb the course of disease progression and relieve the pain. At that point in the course of OA pathology, it is a full-blown disease that involves all joint structures such as the bone, articular cartilage, and synovium. With unknown etiology, OA is believed to be multifactorial in nature, and successful intervention requires a multifaceted approach to target multiple pathways. 23 In practice, NSAIDs are the primary symptomatic therapies, although their long-term usage is limited due to severe side effects. 2 As a result, it is not uncommon for patients to look for safe and efficacious alternatives from natural sources. A mixture of two to three medicinal plants with diverse natural bioactives may provide a favorable outcome. In this study, we presented data supporting this approach wherein the combination of CBD, the major nonpsychoactive component of the hemp plant, with known standardized bioflavonoid compositions (UP446 and UP1306) enhanced the anti-inflammatory and antinociceptive activities of CBD, suggesting efficacy of the plant combination against symptoms associated with OA. Individually, Scutellaria, Morus, and Acacia plants have historical usage for pain and inflammation. Although there is only very limited clinical data on the effect of CBD on arthritic pain, reports from patients show that a significant number use Cannabis for relief from OA-associated pain. 24 The same is true for the bioflavonoid compositions UP1306 and UP446. In a series of randomized double-blind clinical trials, UP446, containing not less than 60% baicalin and 10% catechins, administered at 250–500 mg/day, produced statistically significant improvements in stiffness, discomfort, and activity of daily living with some clinical endpoints as early as 3 days after consumption. 11,12 Similarly, UP1306, containing not less than 15% catechins and 2% mulberroside A, caused a statistically significant reduction in CTX-II (the primary marker for cartilage degradation) in arthritic patients and mitigated delayed onset of muscular soreness in healthy athletes when given at a daily dosage of 400 mg/day. 14,15
Co-administering these standardized bioflavonoids with CBD creates a medicinal complex with diverse mechanisms of action, which is effective in mitigating OA and its associated symptoms. Each medicinal plant targets known pathways of OA progression which, unchecked, could lead to pain and cartilage destruction. There have been reports showing the antinociceptive and anti-inflammatory effects of CBD in Collagen Induced arthritis (CIA)-induced arthritis in mice, MIA-induced arthritis in rats and adjuvant-induced arthritis in rats, all suggesting its potential application in OA. 5 –7 Some have suggested its efficacy could be associated with its effect as an agonist to TRPV1 and TRPA1. With potency equivalent to capsaicin, CBD also inhibits the reuptake and hydrolysis of anandamide, a neurotransmitter that is involved in pain inhibition. 3,4 UP446 monitors other segments of OA disease pathology through its dual COX-LOX inhibition, antioxidation and immune modulation activities. 8 –10 Through its activity in suppressing oxygenases, UP446 also potentially increases anandamide levels by inhibiting its degradation. A prominent endocannabinoid, anandamide, can be significantly metabolized by cyclooxygenases and lipoxygenases. Inhibition of these enzymes may help prevent the immediate inactivation of anandamide, leading to prolonged signaling, 25 and it has been shown that inhibiting anandamide degradation attenuates the development of collagen-induced arthritis and related thermal hyperalgesia in mice. 26 Finally, the hallmark of OA, cartilage degradation, may be spared by the actions of the bioflavonoids in UP1306, a composition that has been shown to be effective in sparing cartilage from degradation. 14,15
Widely used inflammatory and noninflammatory animal pain models such as the hot plate test, visceral pain (writhing test), and carrageenan-induced rat paw edema models have been utilized to evaluate the antinociceptive and anti-inflammatory activity of CBD alone and in combination with the bioflavonoid compositions UP1306 and UP446. Consistent with previous studies, 6,7 this study showed statistically significant antinociception activity when CBD was applied topically. Older patients who experience chronic pain are at greater risk of side effects from enteral and parenteral routes of intervention. 27 These adverse events could be avoided by employing a topical application route. Applying CBD and its formulations directly to the affected areas, such as in cases of muscular strain, sprain, OA, rheumatoid arthritis, and other musculoskeletal conditions, could result in a high concentration of active compounds at the intended target areas, yielding fast and robust pain relief, while minimizing systemic exposure. 28,29 Statistically significant inhibition of pain sensitivity was documented for UP1306 and UP446 through oral administration. 8,13 Since pain is one of the cardinal signs of inflammation, similar antinociceptive outcomes are anticipated following transdermal local application of these standardized compositions given together with CBD.
Data from the abdominal constriction assay revealed that the THC content of the hemp extracts likely aided in producing antinociception activity. Higher THC content corresponded to greater desensitization of pain. Acetic acid-induced visceral pain in mice has long been used for screening of narcotics and NSAID-like compounds for their antinociceptive effects. 30 The abdominal constrictions elicited by the mice consisted of contractions of the abdominal muscles that progressed posteriorly and ended with simultaneous flexor extension of both hind limbs with arching of the back. Upon intraperitoneal administration of the phlogistic agent, the behavioral response lasted for 30 min. 20 Given the immediacy of the behavioral response produced, the effect of CBD in attenuating visceral pain in this model could be the result of direct peripheral nerve desensitization. The visceral pain response was significantly inhibited by a single oral administration of Cannabis extract with various concentrations of actives, including CBD and THC.
Thus study was not without limitations. To observe statistically significant inhibition of pain sensitivity and paw edema at each time point (including 1, 3, and 5 h after administration) in the carrageenan-induced rat paw edema model, UP446 or UP1306 was administered at a dose of 150 mg/kg. As a result, we selected the 150 mg/kg dosage for the combination study. UP446 at 135 or 50 mg/kg; UP1306 at 120 or 85 mg/kg; and CBD at 15 or 30 mg/kg were not tested separately. The direct anti-inflammatory and antinociceptive effect of CBD at 30 or 15 mg/kg cannot be estimated from the 150 mg/kg UP1306 + CBD or UP446 + CBD animals. Regardless, the co-administration of UP446 or UP1306 with CBD enhanced the anti-inflammatory and antinociceptive activity of either UP446 and UP1306 or CBD, suggesting the possibility of reduced daily dosage required for either of the supplement groups.
In our study, the poor oral bioavailability of CBD seemed to be reflected. 31 To observe clinically meaningful and statistically significant antinociceptive and anti-inflammatory activity following acute oral delivery, CBD must be administered at higher dosages. In this study, administered orally at 40 mg/kg, CBD was considered effective as ibuprofen at 100 mg/kg in reducing discomfort and swelling. While further long-term studies are required to evaluate the complementary effects of CBD and the bioflavonoid compositions, UP446 and UP1306, we believe that the combination of CBD at 10–20% by weight with a reasonable total daily dosage of bioflavonoids from UP1306 and/or UP446 could provide an added benefit to control discomfort and inflammation from OA.
Footnotes
Acknowledgment
The authors would like to express their best gratitude to Wenwen Ma, Regan Miles, and Unigen team for their incalculable support for the completion of this research.
Author Disclosure Statement
All authors are current Unigen employees; therefore, they have competing financial interests.
Funding Information
The authors would like to extend their utmost gratitude to Bill Lee, the owner of Econet/Unigen, Inc., who supported the entire project described in this article.