
Abstract
To investigate effectiveness and safety of a curcumin-based nutritional supplement in neovascular age-related macular degeneration (AMD). We conducted a controlled retrospective study, reviewing the medical records of patients referred to the Eye Center, Humanitas Hospital, Bergamo due to neovascular AMD and treated with antivascular endothelial growth factor (VEGF) intravitreal injections (IVIs) and oral administration of a curcumin-based nutritional supplement vehiculated by enterosoma-I®. We retrospectively collected data of 18 naive patients who received IVI and daily oral nutritional supplement and 24 naive age-matched controls with the same diagnosis undergoing only IVI. All patients underwent a loading-phase of one-per-month IVI for 3 months and then received IVI pro re nata. Median best-corrected visual acuity was significantly improved in treated patients compared with controls (P < .05), while there was no statistical difference in central macular thickness between groups (P > .05). The total number of injections (tIVI) was significantly (P < .05) reduced in the treated group compared with controls. The tIVI in treated group ranged from 3 to 5 with a median of 4 while control group received a tIVI that ranged between 6 and 7 with a median of 7. Treatment with curcumin-based nutritional supplement was safe and effective. Curcumin is a promising adjuvant of anti-VEGF treatment, improves functional outcomes, and prolongs duration.
Introduction
Age-related macular degeneration (AMD) is a leading cause of progressive loss of vision. 1 AMD is a multifactorial disorder with a strong genetic component influenced by environmental factors, including diet. 2 Age-Related Eye Diseases Study (AREDS) and AREDS2 clinical trials demonstrated the efficacy of a combined supplement containing high doses of antioxidants in reducing progression to advanced AMD. 3 Although controversial, fish and omega-3 fatty acid consumption was demonstrated to be associated with a reduced risk of developing AMD. 4
Neovascular AMD is a late form characterized by a choroidal neovascularization (CNV). Inhibition of vascular endothelial growth factor (VEGF) is effective in slowing down the angiogenic process. 1 Most common treatment regimens are three: monthly injections, 5,6 treat and extend, 7 and pro re nata (PRN). 8,9
In this study, we evaluated the effects of a nutritional supplement (Macula 360; Doc, Italy) composed of 150 mg of curcumin (curcuma longa l., rizoma), AREDS2 components, 4 mg astaxanthin (from haematococcus pluvialis flotow algae), and 20 mg resveratrol (from roots of polygonum cuspidatum siebold). The curcumin is a powerful antioxidant that has been used for 1000 years in traditional Chinese medicine and is now widely diffused worldwide with pleiotropic applications. 10 The use of curcumin in AMD was investigated on cellular models demonstrating decreased apoptosis of retinal pigmented epithelial cells and reduction of inflammatory markers. 11,12 So far, the use of curcumin has been limited by the poor bioavailability, and to overcome this issue, different types of carriers have been used. 13 Astaxanthin (AST) is a carotenoid with antioxidative and anti-inflammatory effect 14 that showed to be effective in the suppression of AMD CNV in vitro and in vivo 15 ; moreover studies showed AST to be beneficial in different ocular conditions, 16 including a controlled randomized trial that showed selective improvement of central retina function. 17 Resveratrol is a polyphenol phytoalexin with antiproliferative proprieties that demonstrated to enhance anti-VEGF effect when tested on an in vitro model of AMD. 18 To the best of our knowledge, this is the first study investigating effectiveness and safety of a curcumin-based nutritional supplement in neovascular AMD. To enhance bioavailability, the nutritional supplement was vehiculated with an innovative carrier (enterosoma-I®).
Methods
Study design and participants
We conducted a retrospective study reviewing charts of adult patients referred to the Eye Center of the Humanitas Hospital Bergamo between May 2018 and December 2018 due to neovascular AMD and treated with intravitreal injection (IVI) of aflibercept. This study conformed to the Declaration of Helsinki and ethics approval was deemed not necessary by the Ethics Committee of Humanitas Gavazzeni, in accordance to the Italian law as our work did not involve particular changes in existing procedures in our clinical practice. We included patients at least 60 years old, diagnosed with primary CNV associated with AMD involving the foveal center undergoing scheduled IVI for the first time (naive). We excluded patients diagnosed with other eye comorbidities that could bias best-corrected visual acuity (BCVA), including diabetic retinopathy, glaucoma, and retinal vein occlusion. We excluded patients receiving other anti-VEGF compounds or without a complete follow-up (f/u). We identified a group of patients already receiving a curcumin supplement on a daily basis that in this study is indicated as “treated.” This group of patients started the supplement between 3 months and 1 week before the observed period.
Nutritional supplement
The nutritional supplement posology was 1 tablet per day after breakfast. The supplement was composed of 150 mg of curcumin (curcuma longa l., rizoma) dry extract with minimum 95% of curcuminoids, AREDS2 components, 4 mg astaxanthin (from haematococcus pluvialis flotow algae), and 20 mg resveratrol (from roots of polygonum cuspidatum siebold). The nutritional supplement was vehiculated in gastro-resistant capsules (enterosoma-I), and this patented technology is based on a gastro-resistant tablet whose core contains a combination of chitosan salified with N-acetylcysteine (NAC) and a polysorbate that work in synergy to reduce the intestinal and hepatic degradation of naturally derived active ingredients and enhance absorption by temporarily loosening intestinal tight junctions. 19
Outcome measures
The primary outcomes were the change in BCVA and in central macular thickness (CMT). The secondary outcome was to assess the number of injections needed in the PRN regimen.
Clinical assessment protocol
All patients underwent a comprehensive ophthalmic examination at the baseline and at each f/u visit. The f/u visits were scheduled on a monthly basis for 6 months. We collected data regarding age, sex, and ocular history. The ophthalmic examination protocol included BCVA assessment in Snellen fractions, applanation tonometry, slit lamp biomicroscopy, dilated fundus examination, and spectral domain optical coherence tomography (SD-OCT) imaging. At the baseline, the diagnosis was confirmed by fluorescein angiography.
SD-OCT scan protocol
We used the Spectralis SD-OCT with eye tracking (Heidelberg Engineering GmbH, Heidelberg, Germany). At each visit, the following scans were acquired in all eyes: a high-definition horizontal fovea-centered crossline B-scan at 30 and the horizontal macula raster consisting of 49 B-scans 120 μm spaced over an area of 20°·20°. The “Thickness Map” function was used to measure automatically the mean CMT, based on the mean retinal thickness within a circular area of 0.5-mm radius from the foveal center. Two masked observers (D.A. and R.R.) independently evaluated OCT images quantitatively and qualitatively. A third observer (M.R.R.) resolved any case of disagreement. Segmentation errors were manually corrected with built-in software when needed.
Treatment protocol
After informed consent, all patients had the IVI performed in our clinic. IVI of anti-VEGF (aflibercept) was carried out in the operating room by skilled surgeons or trainees under supervision. The treatment regimen was articulated in a loading-phase of 3 IVI:baseline, month 1, and 2. After that, IVI was provided as needed (PRN regimen) during the monthly f/u, and treatment decisions by ophthalmologists were consistent with the identification of fluid on SD-OCT scans. All patients included in the treated group were taking the curcumin-based nutritional supplement at baseline daily and during all the f/u.
Safety assessment
At each f/u visit we investigated frequency and severity of any adverse event
Statistical analysis
To carry out the statistical analysis, we used STATA/IC 16 software and converted all Snellen BCVA values into logarithm of the minimum angle of resolution (logMAR) units. All data were expressed as median–interquartile range. For the comparison of continuous variables at baseline and each f/u visit, we used the Mann–Whitney test. For the comparison of categorical variables, we used chi-squared test. The differences were considered statistically significant if P value was <.05.
Results
Patient disposition and characteristics
According to our inclusion criteria we retrospectively collected data of 18 patients who received IVI and the nutritional supplement and 24 age-matched controls with the same diagnosis undergoing only IVI. Baseline demographic characteristics and clinical findings of these patients are displayed in Table 1 and well balanced among the groups. The total dosage per person at the end of the observed period in the treated group was 184 capsules.
Baseline Demographics and Clinical Findings
BCVA, best-corrected visual acuity; IQR, interquartile range; OD, oculus dexter; OS, oculus sinister.
Best-corrected visual acuity
The comparison between BCVA at baseline did not show a statistically significant difference in BCVA in treated patients compared with controls (P > .05).
The comparison between BCVA at each f/u showed a statistically significant difference in BCVA in treated patients compared with controls (P < .05 for all). In treated and control group, the median BCVA (logMAR) was, 0.61 [0.30–1.30] and 0.85 [0.30–1.30] at the baseline, 0.40 [0.28–0.77] and 0.85 [0.40–1.30] at 1 month, 0.46 [0.20–1] and 0.85 [0.40–1.30] at 2 months, 0.46 [0.18–0.70] and 1 [0.50–1.30] at 3 months, 0.40 [0.15–0.70] and 1 [0.50–1.50] at 4 months, 0.30 [0.15–0.64] and 1.3 [0.52–1.47] at 5 months, and 0.40 [0.28–0.46] and 1 [0.46–1.5] at 6 months, respectively (Fig. 1).
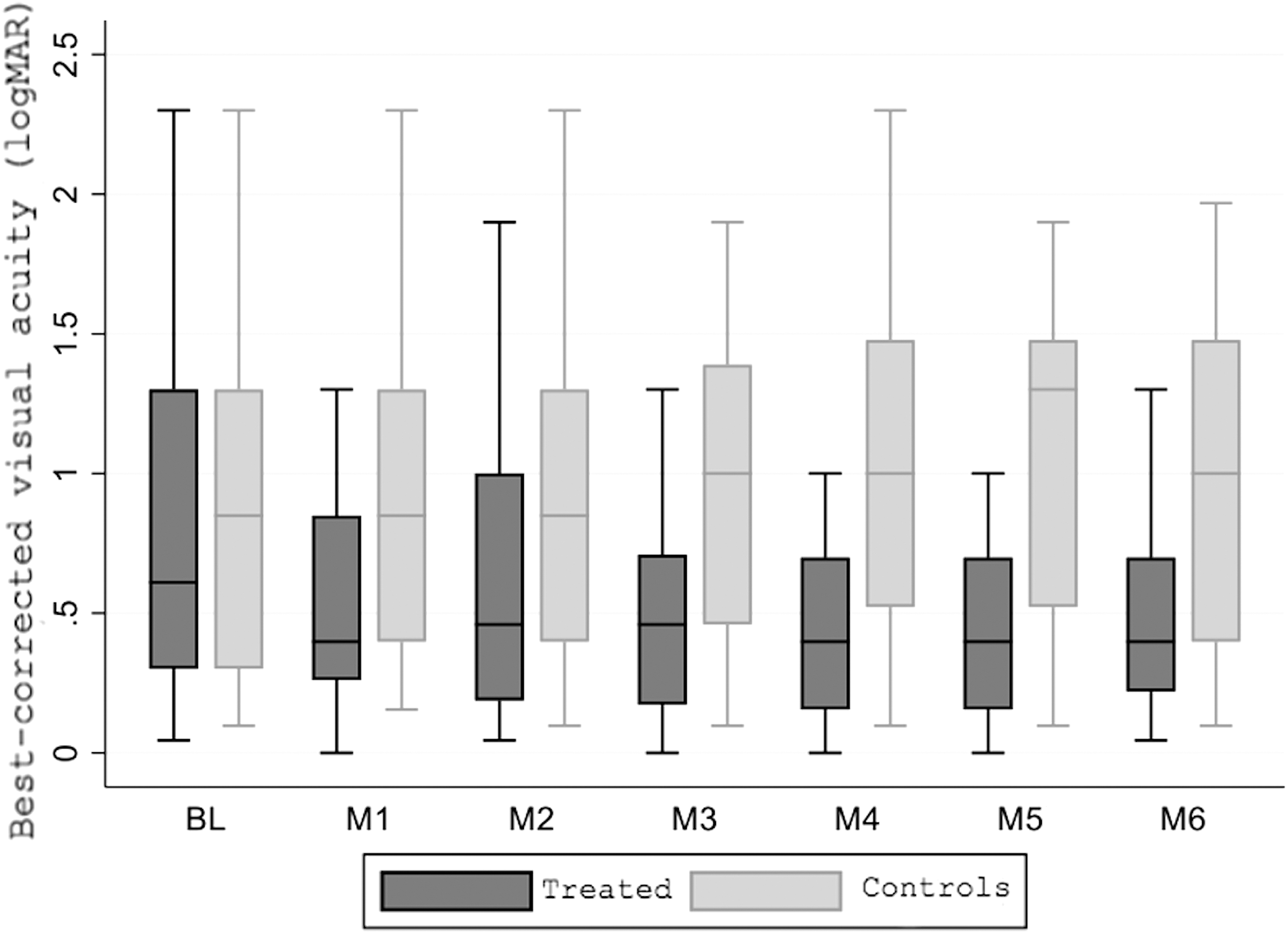
BCVA at BL and at 1-month f/u (M1), 2-month f/u (M2), 3-month f/u (M3), 4-month f/u (M4), 5-month f/u (M5), 6-month f/u (M6). BCVA, best corrected visual acuity; BL, baseline; f/u, follow-up.
Central macular thickness
The comparison between CMT at the baseline and at each f/u did not show a statistically significant difference in treated patients compared with controls (P > .05 for all). In treated and control groups, the median CMT was 402 [319–490] μm and 466 [327–571] μm and at the baseline, 408 [320–555] μm and 307 [228–408] μm at 1 months, 278 [234–371] μm and 393 [311–511] μm at 2 months, 281 [219–343] μm and 382 [253–528] μm at 3 months, 293 [232–383] μm and 353 [288–460] μm at 4 months, 289 [225–351] μm and 356 [279–484] μm at 5 months, and 294 [243–436] μm and 301 [217–420] μm at 6 months, respectively (Fig. 2).

CMT at BL and at 1-month f/u (M1), 2-month f/u (M2), 3-month f/u (M3), 4-month f/u (M4), 5-month f/u (M5), 6-month f/u (M6). CMT, central macular thickness.
Number of injections needed in PRN regimen
Starting from month 3 (M3) patients received IVI based on PRN protocol. Month by month and total number of IVI received are reported in Tables 2 and Table 3. There was a significant (P < .05) reduction in the number of injections needed by the treated group in month 3.4 and 5. No significant (P > .05) difference was observed at month 6. The total number of injections (tIVI) was significantly (P < .05) reduced in the treated group compared with controls. The tIVI in the treated group ranged from 3 to 5 with a median of 4 while control group received a tIVI that ranged between 6 and 7 with a median of 7.
Number and Percentage of Patients Receiving Intravitreal Injections
IVI, intravitreal injection.
Total Number of Intravitreal Injections Received
Safety assessment
No patient experienced adverse effect during the f/u period.
Discussion
Our study evaluated anatomical and functional results of a novel curcumin-based nutritional supplementation in patients with nAMD undergoing IVI of anti-VEGF.
Curcumin is a natural compound of Curcuma Longa L., and despite its multiple proprieties, real-life application has been limited by poor oral bioavailability. Pharmacokinetic studies showed that curcumin undergoes poor intestinal absorption, efficient first-pass metabolism, and rapid excretion. 20 As an example, a study by Yang et al. showed that 10 mg/kg of curcumin given intravenously in rats gave a maximum serum curcumin level of 0.36 μg/mL, whereas a 50-fold higher curcumin dose administered orally gave only 0.06 μg/mL maximum serum level in rats. 21
Different formulations of curcumin have been proposed to improve bioavailability, including dispersion in a lecithin formulation (Meriva; Indena,Italy), 22 curcumin liquid droplet micromicellar formulation, 23 a combination of curcumin formulation (CurcuWIN, Dry Powder20%) with a polyvinylpyrrolidone-hydrophilic carrier (Diabec,AlfaIntes, Italy). 24 In this study we tested an innovative carrier (enterosoma-I), which consists of a gastro-resistant tablet containing in the inner core, chitosan (CH), a polymer capable of interacting with enteric tight junctions and P-glycoprotein 1 enhancing intestinal absorption. 25 This carrier demonstrated promising in vitro results when used to vehiculate another compound with modest bioavailability: berberine chloride. 26
In patients treated with curcuma-based nutritional supplement vehiculated by enterosoma-I, BCVA was significantly improved (Fig. 1), while there was no significant difference in CMT (Fig. 2). This result is coherent with the latest study showing no direct relationship between these two parameters in AMD. 27 Interestingly, treated cohort received a significantly lower number of IVI during the PRN regimen. In particular, the treated group received a median of tIVI of 4 (3–5), while controls received a median of tIVI of 7 (6–7).
It is important to highlight that inflammation is crucial in the pathophysiology of nAMD, and more precisely parainflammation, which is an adaptive response of the immune system to low levels of tissue stress. 28 A characteristic of parainflammation is the activation of microglia, in nAMD multiple triggers dysregulate this homeostatic system leading to chronic inflammation. This chronic inflammation can be summarized as a strong interaction of feed-forward signaling loops that boost angiogenic and inflammatory cytokines, including VEGF and tumor necrosis factor alpha. 29 In this scenario, we tested the effectiveness of curcumin, which has demonstrated in preclinical studies to downregulate inflammatory cytokines and modulate angiogenesis. In particular curcumin is able to target the nuclear factor kappa B pathway inhibiting inflammation, apoptosis, and reactive oxygen species production. 30 Moreover, the curcumin exerts an antiangiogenic effect through the activation of peroxisome proliferator-activated receptor-γ (PPAR-γ) that results in inhibition of VEGF-induced choroidal angiogenesis in vitro, and CNV in animal models. 31 Thus, we speculate that our results are due to the capacity of curcumin to tackle inflammation and angiogenesis, introducing it as an effective and safe adjuvant treatment in AMD. The high number of injections needed for nAMD is a huge obstacle to compliance, being that affected people have usually other comorbidities, patients can be overwhelmed by time and resources spent for health care ending up in dropping out. 32 In fact, labeled anti-VEGF has a high cost for public and private health systems. 33 Furthermore, evidence shows that in nAMD, there is continued need for frequent IVI, which leads to tachyphylaxis and resistance to anti-VEGF. 34 –36
This curcuma-based nutritional supplement led to a lower number of injections (Tables 2 and 3) with a statistically significant improvement in BCVA (Fig. 1), and without statistically significant difference in anatomical outcomes (Fig. 2), its use could potentially be a solution to increase compliance, delay anti-VEGF resistance, and reduce costs.
Drawbacks
This study has few drawbacks. First, in the treated group one patient at month 5 and two different patients at month 6, and in the control group one patient at month 6 were not able to come for the f/u. Second, the restricted number of population involved limits the power of the study. Third, the retrospective design limits the validity of the results. Lastly, the nutritional supplement, besides curcumin, contains also other compounds that may be responsible for the results, further studies are needed to validate our hypothesis.
In conclusion, there is rising evidence of the potential of curcumin in blocking inflammatory and angiogenic processes of the eye. On behalf of our results, we speculate the curcumin can enhance anti-VEGF treatment boosting efficacy and prolonging duration potentially leading to increased compliance and reduced costs.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Footnotes
Acknowledgment
The authors acknowledge Mrs. Alison Rhodes for revising the English language in the article.
Author Contributions
D.A. substantial contributions to conception and design, data collection and analysis, drafting, and revision. R.R. data collection and analysis, and drafting. M.A. critical revision for important intellectual content. G.R. critical revision for important intellectual content. A.M. data collection and analysis. A.B. data collection and analysis. M.R.R. substantial contributions to conception and design, revision, and final approval.
Author Disclosure Statement
No competing financial interests exist
Funding Information
No funding was received for this article.