
Abstract
One of the proposed mechanisms for the development of diabetic nephropathy (DN) is the increase of end products of advanced glycosylation (AGEs), which bind to its receptor (RAGE), favoring nephron cellular damage. An isoform of this receptor is soluble RAGE (sRAGE), which can antagonize AGE-altered intracellular signaling. It has known that green tea extract (GTE) increases the expression of sRAGE, but it is unknown whether this could improve kidney function. The objective of this study was to evaluate the effect of the administration of GTE on the concentrations of sRAGE, renal function, and metabolic profile in patients with type 2 diabetes mellitus (T2DM) and DN. A randomized, double-blinded, placebo-controlled clinical trial was carried out in 39 patients who received GTE (400 mg every 12 h) or placebo for 3 months. sRAGE levels, renal function, and metabolic parameters were determined before and after the intervention. In the GTE group, there were statistically significant increase on sRAGE (320.55 ± 157.63 pg/mL vs. 357.59 ± 144.99 pg/mL; P = .04) and glomerular filtration rate (GFR; 66.44 ± 15.17 mL/min/1.73 m2 vs. 71.70 ± 19.33 mL/min/1.73 m2; P = .04), and a statistically significant decrease in fasting serum glucose (7.62 ± 3.00 mmol/L vs. 5.86 ± 1.36 mmol/L; P ≤ .01) and triacylglycerols (1.91 ± 0.76 mmol/L vs. 1.58 ± 0.69; P = .02). Administration of GTE increases the serum concentration of sRAGE and the GFR and decreases the concentration of fasting serum glucose and triacylglycerols. The study was registered in
Introduction
Diabetic nephropathy (DN) is one of the main complications of type 2 diabetes mellitus (T2DM), characterized mainly by the decrease in glomerular filtration rate (GFR) and by the increase in protein secretion through the urine. 1 This complication generates an important public health problem that affects 10–16% of the world's adult population, with an increasing incidence. The transition from one stage of chronic kidney disease (CKD) to the next is associated with a clinical increase along with an increased financial burden. 2,3 Therefore, there is a need to prioritize services and manage the use of resources efficiently. 3
T2DM is characterized by high serum glucose levels, which contribute to the progression of kidney damage, in addition to various factors and biochemical mechanisms. 4
One of the best-known mechanisms leading to kidney damage is the increase of the end products of advanced glycosylation (AGEs) and the activation of its receptor (RAGE), which participate in metabolic and biochemical pathways in intracellular signaling, which lead to nephron cellular damage. 5 Various RAGE isoforms have recently been described, such as soluble RAGE (sRAGE), which are devoided of cytoplasmic domains, which bind to ligands that include AGEs and can antagonize altered intracellular signaling. 6
Currently, interventions to delay the progression of DN are limited, such as lifestyle changes, use of pharmacological therapy like drugs with nephroprotective effects such as angiotensin-converting enzyme inhibitors (ACEI) and angiotensin II AT1 receptor blockers (ARBs), as well as some phytopharmaceuticals. Once DN is diagnosed, the improvement in glycemic control is insufficient to delay kidney damage. 1
Due to its chemical composition, especially epigallocatechin-3-gallate (EGCG), green tea extract (GTE) has been attributed antioxidant, anti-inflammatory, and antiangiogenic effects, among others, 7 and they theoretically could delay the progression of DN. 8 Under this context, the objective of the present investigation was to evaluate the effect of the administration of GTE on the concentrations of sRAGE, renal function, and metabolic profile in patients with T2DM and DN.
Materials and Methods
Design subjects
A randomized, double-blind, placebo-controlled clinical trial was conducted in 39 patients with T2DM and DN grades 2 and 3, according to the Kidney Disease: Improving Global Outcomes 2017 guidelines. 9
The study site was the Vascular Mechanics Laboratory of the Institute of Experimental and Clinical Therapeutics, the Physiology Department of the University Center for Health Sciences, University of Guadalajara, Mexico.
After signing the informed consent letter, all patients underwent a complete medical history as well as a physical examination; blood samples were taken in the morning, after an 8-h fasting period at the start of the study, and after the intervention (week 12) for further analysis.
Thirty-nine patients (20 GTE and 19 placebo) were included as shown in Figure 1, according to the following selection criteria: diagnosis of T2DM 10 and DN grade 2 and 3, age from 35 to 70 years, albumin/creatinine ratio: A1–A2, 9 HbA1c: ≥7% and ≤12%, and body mass index (BMI) 18.5–34.9 kg/m2. Three months before the intervention, the patients maintained a stable antidiabetic treatment and, if applicable, treatment with an ACEI, ARBs, statins, loop diuretics, and/or thiazide diuretic.
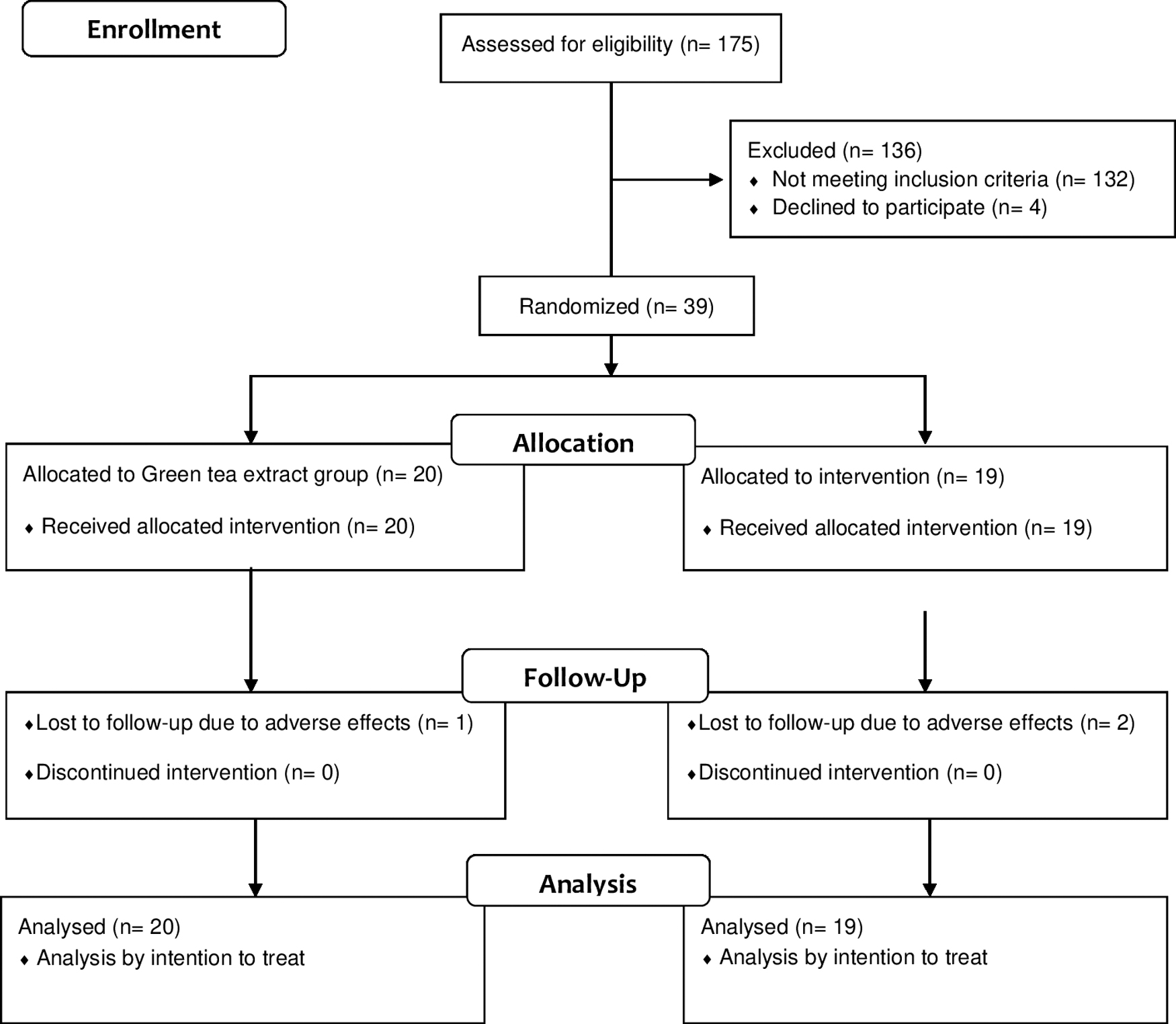
Consort diagram reflecting the flow of study participants.
Patients with other types of diabetes, as well as other causes of kidney, liver, thyroid, or heart disease, as well as consumption of antioxidant supplements, alcoholism, and active smoking, were excluded.
The patients were randomly assigned to receive 400 mg of decaffeinated GTE (Sunphenon 90D), which composed of the following: total polyphenols ≥90%, total catechins ≥80%, epigallocatechin-3-gallate (EGCG) ≥45%, and caffeine ≤1.0% (Taiyo International Inc., Minneapolis, MN, USA), or 400 mg of placebo (calcined magnesia) every 12 h orally, during 12 weeks.
All the patients were given a diary where they were instructed to report any adverse event during the intervention and the action taken to correct it. Adherence to treatment was evaluated through the patient's diary, capsule count at the end of the intervention, and supervisory telephone calls. Acceptable compliance was defined as the intake of at least 80% of the expected dose for the proposed intervention time.
This study adhered to the ethical guidelines established in the Declaration of Helsinki of 1975 and its last amendment in Fortaleza, Brazil (2013), and was approved by the ethics committee of the University Center for Health Sciences of the University of Guadalajara, Mexico, with the identification number CEI:/455/2018.
Randomization and blinding
Patients were randomly assigned to receive GTE or placebo using computer-validated software; double-blinded technique was used by masking the organoleptic characteristics of both the active drug and the placebo.
Sample size determination
The sample size was calculated according to the comparison of means in clinical trials formula, 11 with a statistical confidence level of 95%, a statistical power of 80%, considering the following three outcome variables: standard deviation (SD) of 1.67 mmol/L for fasting serum glucose, 12 1.3 pg/mg for the albumin/creatinine ratio, and 12.26 mL/min/1.72 m2 for GFR, 13 obtaining a total of 16 patients per group, with an additional 20% due to possible expected losses, obtaining a total of 19 patients per group.
Statistical analysis
Values were converted to the International System of Units and presented as mean ± SD. The Shapiro–Wilk test was used to evaluate the normal distribution. Intention-to-treat statistical analysis was carried out. Intragroup and intergroup differences were tested by the Wilcoxon signed-rank and Mann–Whitney U test, respectively. A P ≤ .05 was considered statistically significant. Statistical analysis was conducted using IBM SPSS® 18.0 for Windows.
Clinical determinations
Body weight was measured with a bioimpedance digital scale (TBF-215® Body Composition Analyzer; Tanita Corporation, Tokyo, Japan), patients wore light clothing, and the value was expressed in kilograms.
The BMI was calculated by the body weight expressed in kilograms divided by the height expressed in square meters and was obtained with a stadiometer, with the patient standing without shoes. The waist circumference was recorded in centimeters using a flexible tape (Executive® Thinline Tape Measure; Lufkin Industries, Sparks, MD, USA).
Venous blood samples were obtained after 8 h of fasting and centrifuged at 700 g (Beckman Coulter, Allegra X-22R, Brea, CA, USA) for 10 min. Serum and plasma were separated and stored at −80°C for further analysis. To determine fasting serum glucose, the glucose oxidase technique was used (Merck Mexico), with an intra- and interassay coefficient of variation of <3%.
Total cholesterol, triacylglycerols concentration, uric acid, aspartate transferase, alanine transferase, serum creatinine, urinary albumin, urinary creatinine, and albumin/creatinine ratio levels were measured by enzymatic colorimetric methods with automatic equipment (XL-100®; Erba Diagnostics, Mannheim GmbH, Mannheim, Germany), with an intra- and interassay coefficient of variation of <2%.
The percentage of A1c glycated hemoglobin (HbA1c) was measured by high-performance liquid chromatography Ion Exchange (Bio-Rad Laboratories, Inc., Hercules, CA, USA). All determinations had interest coefficients of variation <1% and 2%, respectively.
sRAGE determination
Serum sRAGE levels were determined using an enzyme-linked immunosorbent assay (ELISA); all procedures were performed according to the manufacturer's specifications (MyBioSource, Antibody, Protein, ELISA Kit), which is specific for the extracellular domain with a coefficient of variation within and between assay <4%. 14
Results
At baseline, no differences in demographic, metabolic, renal function, and sRAGE concentrations were observed between patients treated with GTE and placebo, as shown in Table 1. Fifty-three percent of the patients were male, the average time of evolution of T2DM was 13.8 ± 8.3 years, and of DN was 2.1 ± 1.2 years. 64.1% of the patients presented grade 2 DN and 35.8% grade 3 DN.
Baseline Clinical Characteristics of the Intervention Groups
P ≤ .05. There were no significant differences in characteristics at baseline between the groups (Mann–Whitney U test).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; DBP, diastolic blood pressure; DN, diabetic nephropathy; GFR, glomerular filtration rate; HbA1c, A1c glycated hemoglobin; SBP, systolic blood pressure; sRAGE, soluble receptor for advanced glycation end products; T2DM, diabetes mellitus type 2; TC, total cholesterol; TGC, triglycerides.
Table 2 shows the intragroup change in all analyzed variables studied after the intervention in both groups (GTE and placebo), as well as differences observed after the intervention between the two groups. Here, we highlight that the GTE group had a statistically significant decrease in serum concentrations of fasting serum glucose, triacylglycerols, and an increase in GFR. While in the group that received placebo, an increase in serum creatinine was observed.
Baseline and Final Clinical Characteristics of the Intervention Groups
P a between baseline and 12-week measurement intragroup (Wilcoxon rank test). P b deltas of the clinical characteristics of the intervention groups (Mann–Whitney's U test).
Asterisks highlight values with statistically significant difference.
When carrying out the stratified analysis according to the degree of nephropathy, a significant decrease in fasting serum glucose concentrations was only observed in patients with grade 2 DN in the GTE group (data not shown).
When analyzing the change in sRAGE concentrations after the intervention, there was a statistically significant increase in the GTE group (Fig. 2), not so in the placebo group.
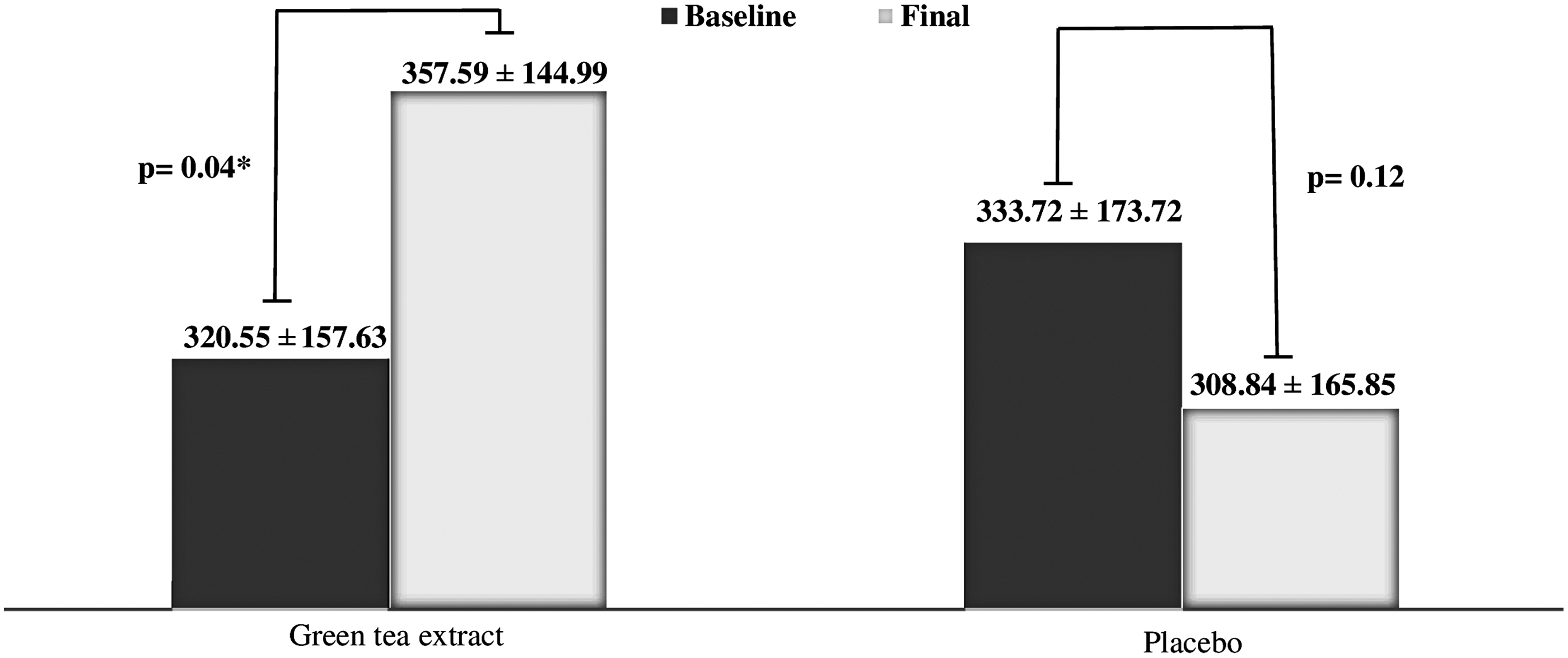
Baseline and final concentration of sRAGE. Test P ≤ .05. *P-value shown from Wilcoxon range. sRAGE, soluble receptor for advanced glycation end products.
Discussion
In the present study, we found several relevant effects associated with the daily administration of 400 mg every 12 h of GTE for 12 weeks. We identified a significant increase in serum concentrations of sRAGE. In vivo studies suggest that the AGE-RAGE pathway is one of the most important mechanisms in the progression of the inflammatory response that induces target organ damage. 15
Recently, the soluble form of RAGE (sRAGE) that is circulating in plasma has been identified and studied. It is known that two mechanisms promote its expression, the alternative splicing of the RAGE gene observed in murine models 16 and, through the integrin and metalloproteinase 10 (ADAM10) protein, generating the detachment of the transmembrane domain and the cytosolic tail, forming sRAGE. It has been suggested by different publications that circulating sRAGE acts as a decoy receptor for AGEs and inhibits the AGE-RAGE pathway. 17
To support this theory, one study showed that GTE efficiently stimulates the secretion of circulating sRAGE through the elimination of the transmembrane domain and the cytosolic tail of RAGE, through ADAM10, blocking the intracellular signaling associated to the AGE-RAGE pathway. 18
In a double-blinded clinical trial, 51 T2DM patients who were randomly allocated to one of four groups according to oral GTE 300, 600, or 900 mg/day, after 2 months of supplement, demonstrated that the GTE from a low, medium, and high dose efficiently stimulates the secretion of sRAGE through the removal of the RAGE ectodomain, through ADAM10. 12
Recently, Quezada-Fernández et al. 19 in their study to evaluate the effect of GTE administration in patients with T2DM found no changes in the concentrations of sRAGE; however, a possible explanation for their results was the low dose administered (400 mg/day). Based on this information and our results, we conclude that the optimal GTE dose to modify sRAGE concentrations ranges from 800 to 900 mg daily for a minimum of 12 weeks.
Another interesting finding in our study was the increase in GFR in the group with GTE. We know that GFR is classically used to assess individual kidney function, as well as to classify the stage of CKD in patients with T2DM. Additionally, the measurement of GFR is a crucial prognostic factor and essential for the adjustment of pharmacological prescriptions, particularly in healthy elderly subjects and kidney damage patients with other etiologies not related to diabetes. 20
In our study, GFR was used as one of the main outcome variables to evaluate the effect of GTE administration on kidney function in patients with T2DM, assuming three of the potential mechanisms of action attributed to green tea (GT) polyphenols, among which we highlight the role of sRAGE, glycemic control, and its antioxidant effect.
AGEs are known to be the products of nonenzymatic glycation because of long-term elevated glucose levels. The AGE-RAGE interaction plays an important role in the development of chronic complications of diabetes such as DN. Activation of positive feedback from the AGE-RAGE axis is believed to increase target organ damage through the intracellular production of reactive oxygen species, which activate the nuclear factor κB (NF-κB), consequently triggering the inflammatory response and activating even other signaling pathways such as p21Ras and the mitogen-activated protein p38, (p38 MAPK) crucial for the development of chronic complications, such as damage to glomerular mesangial cells as well as tubular epithelial cells of the kidney. 21 –24
Supported in this previous information, it is likely that by increasing the concentrations of sRAGE, the axis of positive feedback AGE-RAGE was blocked and consequently decreased the altered intracellular signaling, particularly in glomerular and renal tubular cells; however, this hypothesis is yet to be confirmed.
Another possible explanation for the increase in GFR could be due to the decrease in serum creatinine concentrations observed in this study, probably dependent on better glycemic control. Regarding the reduction of fasting serum glucose concentrations, our results add to the potential role of GT as a glycemic regulator reported by other authors.
In a published meta-analysis by Liu et al., 25 of 27 studies involving 1898 subjects, it was evaluated that the effect of consuming GTE (367.3 ± 175.5 mg/day and a median duration of 9 weeks), compared with placebo/water, on the concentrations of fasting serum glucose, was shown to reduce fasting serum glucose concentrations slightly (−0.14 mmol/L; 95% confidence interval, −4.67 to −0.35; P = .02).
In our clinical trial, the effect on the reduction in fasting serum glucose concentrations was greater than those reported in this meta-analysis, possibly attributed to the longer administration time, as well as the consumed dose and the concentrated galenic form of GT.
Some action mechanisms have been attributed to the consumption of GT in the reduction of fasting serum glucose. Waltner-Law et al. 26 argued that GT exerts insulin-mimetic effects and promotes phosphorylation of insulin signaling proteins, such as the insulin receptor substrate type-1 (IRS-1) and the insulin receptor that decrease the expression of genes that control gluconeogenesis, such as the PEPCK and G6Pase genes. It is also known that the glucose transporter 4 (GLUT 4) in adipose tissue plays a fundamental role in the development of T2DM, observing a decrease in the expression of this transporter, according to the evolution time of this pathology. 27
A trial carried out by Wu et al. 28 showed that GTE supplementation reversed the shortfall of GLUT 4, thus increasing insulin sensitivity. We can assume that there is sufficient evidence that demonstrates that the consumption of GT in its different forms and doses, through various action mechanisms, favors a reduction in glucose concentrations, as we observed in our study.
Regarding the reduction in triacylglycerols, our study agrees with that reported by various authors, among which are the findings, published in a clinical trial, in which it was shown that there was a significant reduction in triacylglycerols with the administration of 500 mg of GTE three times a day, for 16 weeks. 29
Taking into account the possible mechanisms through which GT participates in the decrease of triacylglycerols, catechins are known to modulate lipid homeostasis, Dinh et al. 8 observed that lipid expression in adipocytes was suppressed after 24 h of incubation with GT catechins, without any side effect on cell viability during cell differentiation, and Sugiura et al. 30 reported that GT catechins reduce the accumulation of lipids by inhibiting the synthesis and upregulation of acid β-oxidation. This shows that there are elements to assume that GT can affect triacylglycerol concentrations, regardless of body weight reduction, or other lifestyle interventions, as observed in our study.
In terms of tolerability and adverse events, in this study, the GTE was well tolerated and no patient reported serious adverse effects or had abnormal liver or kidney function tests. However, although the literature indicates possible adverse reactions at the liver level related to GT 31 such as hepatotoxicity, probably associated with pharmacological or dose-dependent interactions, 32 so we suggest that before the administration of the GTE is decided, liver function should be evaluated.
To the best of our knowledge, this is the first study that shows that the administration of GTE at a dose of 400 mg twice a day for 12 weeks increases concentrations of sRAGE, GFR, and improves the metabolic profile in patients with T2DM, and consequently, this could delay the progression of DN; however, this requires a greater accumulation of scientific evidence to confirm our hypothesis.
Footnotes
Acknowledgment
The authors wish to thank the personnel of the Vascular Mechanics Laboratory for their collaboration in the compilation and data analysis.
Author Disclosure Statement
All authors disclose any actual or potential commercial associations that might create a conflict of interest in connection with this article, and no competing financial interests exist.
Funding Information
No funding was received from agencies or institutions.