
Abstract
Neem (Azadirachta indica) exhibits multiple therapeutic benefits in preclinical studies, but clinical studies are lacking. This clinical study investigated the efficacy and safety of an aqueous A. indica leaf and twig extract (NEEM) on metabolic parameters in subjects with metabolic syndrome (MetS). Subjects were randomized to receive (1) placebo or (2) 125 mg, (3) 250 mg, or (4) 500 mg of NEEM twice daily (n = 20/group) for 12 weeks. Fasting blood sugar (FBS) and insulin, postprandial blood sugar (PPBS), insulin resistance (IR), hemoglobin A1c (HbA1c), endothelial function, circulating markers of inflammation and oxidative stress, lipid profiles, and platelet aggregation were measured at weeks 0, 4, 8, and 12. NEEM supplementation dose dependently improved the trajectories for FBS, PPBS, IR, and HbA1c over time, as well as endothelial function and most markers of inflammation and oxidative stress. Therefore, NEEM may be considered a promising therapeutic to attenuate the hyperglycemia and associated cardiometabolic derangements in people with MetS. Clinical trial registration no.: CTRI/2019/03/018034 [registered on: March 12, 2019].
Introduction
Metabolic syndrome (MetS) is a common clustering of coincident cardiometabolic derangements, including elevated blood pressure, sugar, and lipids, associated with increased risk for cardiovascular diseases (CVD) and type 2 diabetes (T2D). 1 People with MetS have a fivefold and twofold increased risk for T2D and CVD, respectively, including three to four times increased risk of myocardial infarction. 2,3 The International Diabetes Federation (IDF) has established criteria to define MetS (Table 1). 4
The Criteria for the International Diabetes Federation (2006) for Metabolic Syndrome
If BMI is >30 kg/m2, central obesity can be assumed, and waist circumference does not need to be measured.
BMI, body mass index; HDL-C, high-density lipoprotein-cholesterol; T2DM, type 2 diabetes mellitus.
The incidence of MetS is interlinked with the prevalence of T2D, CVD, and obesity. About 8.8% of adults (20–79 years of age) in the global population (425 million) was estimated to suffer from diabetes mellitus (DM), and about 4 million elderly people (>60 years old) die per year due to DM. 5 Relative risk for CVD morbidity and mortality ranges from 1 to 3 in men with DM and from 2 to 5 in women with DM compared to those without DM. 6,7
A strong association between MetS and oxidative stress and inflammation exists. 8 The pathogenesis of endothelial dysfunction is interlinked with each component of MetS. 9 Excess cholesterol substantially alters endothelial function by decreasing the relaxation of arterial vessels. 10 –12 High cholesterol levels aggravate coronary artery disease across all levels of blood pressure. 13 Therapeutic approaches to manage MetS involve lifestyle modification (e.g., diet) and treatment(s) for specific components such as reducing blood sugar levels. Traditional alternative therapeutic approaches, if effective, are attractive due to accessibility and possibly lower potential for adverse side effects.
Neem (Azadirachta indica) has been widely used for medicinal purposes since antiquity. Different neem extracts have exhibited numerous pharmacological activities, including hypoglycemic, antioxidant, anti-inflammatory, antidiabetic, and hypolipidemic activities, 14 –21 but no human clinical study has been reported. These authors have previously conducted a clinical trial in patients with T2D already receiving standard metformin therapy in which daily dietary supplementation with a proprietary aqueous neem leaf and twig extract (NEEM) lead to greater reductions in blood sugar levels and insulin resistance, 22 which prompted this clinical trial to investigate the therapeutic potential of NEEM in subjects' MetS.
Materials and Methods
This 12-week prospective, randomized, double-blind, placebo-controlled trial was conducted between March 2019 to September 2019 at the Department of Clinical Pharmacology and Therapeutics, Nizam's Institute of Medical Sciences (NIMS), Hyderabad, India.
Subject enrollment
Subjects were recruited from the NIMS outpatient department and informed consent was acquired before enrollment into the study. Figure 1 depicts the visit schedule of the study subjects.
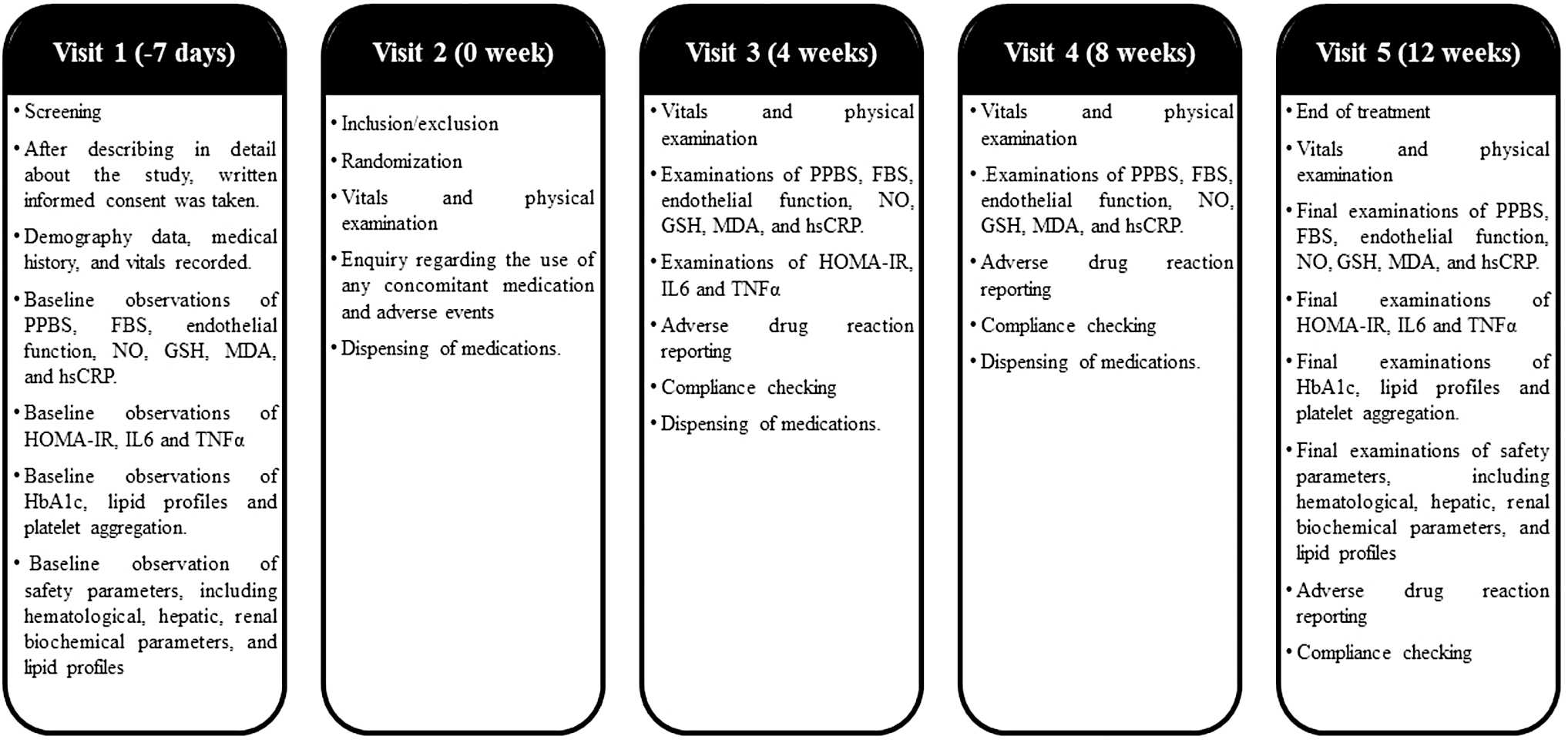
Treatment protocol.
Inclusion criteria
Men and women between 30 and 65 years of age diagnosed with endothelial dysfunction, defined as ≤6% change in reflection index (RI) on post salbutamol challenge test, and MetS, according to IDF criteria (Table 1), not receiving any prescription medicine in the past 6 months were eligible for inclusion in the study.
Exclusion criteria
Subjects with abnormal hematological or biochemical parameters, uncontrolled hypertension (systolic blood pressure >180 mmHg and diastolic blood pressure >100 mmHg), excess serum triglycerides (TG) (>500 mg/dL), impaired hepatic or renal function (aspartate aminotransferase [AST] and alanine aminotransferase [ALT] elevated >3 × the upper limit of the normal range; serum creatinine >1.5 mg/dL), history of malignancy or stroke, and history of smoking or chronic alcoholism, and under active treatment, or taking other herbal supplements were excluded from this study.
Ethical consideration
The study was conducted following the Declaration of Helsinki (2013) and Guidelines for Clinical Trials on Pharmaceutical Products in India—GCP Guidelines issued by the Central Drugs Standard Control Organization, Ministry of Health, and Government of India. IRB approval was received from NIMS Institutional Ethics Committee. This clinical study has been registered in the clinical trial registry—India (clinical trial registration no.: CTRI/2019/03/018034 [registered on: March 12, 2019]).
Investigational products
Capsules containing the standardized aqueous neem leaf and twig extract (PhytoBGS®) and matching placebo capsules were manufactured and donated by Natreon, Inc., New Brunswick, NJ, USA. Placebo capsules comprised excipients only (i.e., microcrystalline cellulose, croscarmellose sodium, silicon dioxide, and magnesium stearate).
Bioactive composition of PhytoBGS
Many bioactive compounds have been isolated from neem, including nimbin, nimbolide, azadirachtin, azadiradione, nimbidiol, quercetin, and nimbidin. 14 Bioactives in PhytoBGS, quantified by HPLC-photometric diode array, include flavonoids, consisting of quercetin-3-O-glucoside, quercetin-3-O-rutinoside, apigenin rutinoside, and rutin derivatives, and is standardized to ≥5% myo-inositol monophosphate quantified by HPLC-evaporative light scattering detector.
Randomization
Eligible subjects were randomly assigned to one of the four treatment groups in a 1:1:1:1 ratio using unstratified blocks of the same length by computer-based predetermined randomization (Prism 8, GraphPad).
Blinding
All investigational products were manufactured as opaque gelatin capsules of the same size, shape, texture, and weight, packaged in matching tamper-proof containers. The bottles were distributed to subjects as per randomization assignment by the research pharmacist. Unblinding occurred after all subjects completed the study.
Study groups
Placebo: Two placebo capsules BID
NEEM125: 1 capsule NEEM (125 mg) +1 placebo capsule twice daily (BID) (250 mg/day)
NEEM250: 1 capsule NEEM (250 mg) +1 placebo capsule BID (500 mg/day)
NEEM500: 2 capsules NEEM 250 mg BID (1000 mg/day)
Subjects were instructed to take capsules with water (∼250 mL) after food.
Efficacy variables
Efficacy variables measured included reductions in fasting blood sugar (FBS) and postprandial blood sugar (PPBS) ≥10 mg/dL, hemoglobin A1c (HbA1c) ≥1%, and RI >6%, and changes in markers of oxidative stress (nitric oxide [NO], reduced glutathione [GSH], and malondialdehyde [MDA]), inflammation (high sensitivity C-reactive protein [hsCRP], interleukin 6 [IL-6], and tumor necrosis factor α [TNF-α]), lipid profile (total cholesterol [TC], low-density lipoprotein-cholesterol [LDL-C], very LDL-C [VLDL-C], high-density lipoprotein-cholesterol [HDL-C], and TG), insulin resistance (homeostatic model assessment of insulin resistance [HOMA-IR]), and platelet aggregation at weeks 0, 4, 8, and/or 12 using standard laboratory techniques.
Assessment of endothelial function
Endothelial function was measured at weeks 0, 4, 8, and 12 using the salbutamol challenge test utilizing digital volume plethysmography. 23,24
Safety evaluation
Complete physical examination was performed and safety parameters, including blood, liver, and kidney biochemical parameters, were measured at weeks 0 and 12. Subjects were instructed to report any adverse reaction associated with the investigational products.
Statistical analyses
Quantitative data are expressed as means ± standard deviations (SD). All statistical analyses were performed using IBM SPSS version 23. All efficacy measures were compared by repeated measure analysis of covariance (RM-ANCOVA) keeping the baseline values as covariates. The within-group statistical analysis was performed using paired ‘t’ test. Differences between the means were considered statistically significant at p < 0.05. The effect size was determined using partial eta-square (ηp 2 ) with 0.01 considered to be small, 0.06 to be medium, and <0.14 to be large.
Results
Eighty eligible subjects were enrolled in the study from the 94 candidates screened. All enrolled subjects completed the 12-week intervention. Figure 2 shows the CONSORT diagram. Subjects' demographics are shown in Table 2. Baseline characteristics did not differ significantly between groups (Table 2).
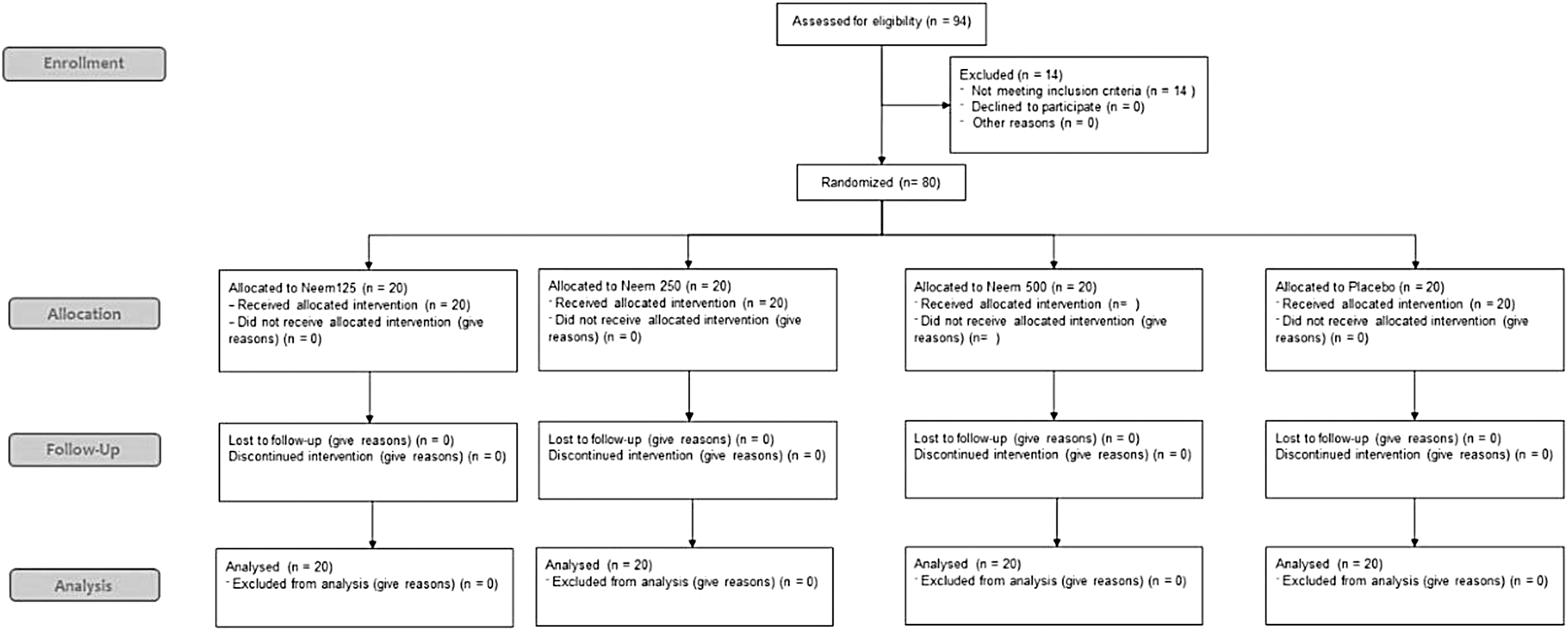
CONSORT diagram.
Demographic Data of the Randomized Subjects
Glycemic regulation
FBS modestly increased over the 12-week intervention in the placebo group (Table 3), whereas this increase was attenuated in NEEM125 and FBS was modestly decreased in NEEM250 and more so in NEEM500, suggesting dose-dependent effects. Thus, the trajectory of FBS over time, and significantly decreased in NEEM250 and NEEM500, was decreased in all treatment groups and significantly decreased in NEEM250 and NEEM500, compared to the placebo group (Table 3). Fasting insulin increased over 17% in the placebo group after 12 weeks, but again, this increase was prevented in NEEM125 (+1.4%) and decreased dose dependently in NEEM250 (−2.7%) and NEEM500 (−6.5%) (data not shown), HOMA-IR measurements mirrored these results, increasing over 24% in the placebo group and only ∼4% in NEEM125, but decreasing ∼5–6% in NEEM250 and ∼12% in NEEM500 (Table 4). Thus, HOMA-IR was significantly decreased in all treatment groups compared to the placebo group (Table 4).
Effect on Fasting Blood Sugar (mg/dL)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
Effect on Homeostatic Model Assessment of Insulin Resistance
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
PPBS was modestly increased over 12 weeks in both the placebo group and NEEM125, but was not changed in NEEM250, and was modestly decreased in NEEM500 (Table 5). Therefore, trajectories for PPBS over time were significantly decreased in NEEM 250 and NEEM500 versus the placebo group (Table 4). HbA1c, which broadly reflects glycemic control over the previous 12 weeks, followed similar patterns to other outcomes of glycemic control with HbA1c significantly decreased in NEEM500 and NEEM250 compared to the placebo group (Table 6). Overall, daily NEEM supplementation appeared to dose dependently reduce insulin resistance to improve indices of glycemic control over time, although absolute and percentage changes were modest in this population over the relatively short duration of intervention.
Effect on Postprandial Blood Sugar (mg/dL)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
Effect on Hemoglobin A1c (%)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
Vascular function
Insulin resistance-induced glycemic intolerance, inflammation, and oxidative stress contribute to vascular dysfunction and increase risk of CVDs. The percentage RI improved over time in all treatment groups but remained relatively stable in the placebo group thus, the trajectory over time in the RI was significantly decreased in all treatment groups compared to the placebo group (Table 7). Furthermore, this trajectory over time appeared somewhat dose dependent with stepwise greater improvements with increasing daily dosing. Endothelial NO is essential to vascular function and homeostasis, but NO bioavailability at the level of vascular endothelium is compromised by oxidative stress and inflammation. Despite improvements in the reflection index with NEEM, NO was only significantly increased in NEEM500 versus the placebo group after 12 weeks (Table 8). Overall, daily NEEM supplementation positively influenced vascular function dose dependently.
Effect on Reflection Index (%)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
Effect on Nitric Oxide (μM/L)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
Inflammation and oxidative stress
Inflammation and oxidative stress play causal roles in insulin resistance and glucose intolerance. CRP, a marker of chronic, low-grade systemic inflammation associated with obesity and insulin resistance, modestly decreased over time in NEEM500 and NEEM250, but modestly increased over time in the placebo group and NEEM125, although slightly less in the latter (Table 9). The trajectory over time in hsCRP was significantly decreased dose dependently in NEEM500 and NEEM250 compared to placebo. Although absolute changes in the proinflammatory cytokines, IL-6 and TNF-α (Table 10), were minor or modest, the trajectory over time was significantly decreased in all treatment groups, except in NEEM125 for IL-6, compared to the placebo group (Table 11). The anti-inflammatory effects of NEEM on IL-6 appeared to be dose dependent with greater reductions observed at higher daily dosing.
Effect on High-Sensitivity C-Reactive Protein (mg/L)
Values presented as mean ± SD.
Differences were considered significant at P < .05.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Effect on Tumor Necrosis Factor α (pg/ml)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post−hoc analysis.
Differences were considered significant at P < .05.
Effect on Interleukin 6 (pg/ml)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
MDA, a marker of lipid peroxidation and oxidative stress, slightly increased in the placebo group after 12 weeks, but slightly to modestly decreased in all the treatment groups; therefore, the trajectory over time for MDA was significantly decreased in all treatment groups compared to the placebo group (Table 12). This effect appeared to be dose dependent with greater reductions observed at higher daily dosing. GSH, the body's main endogenous antioxidant, is often decreased in conditions characterized by increased oxidative stress. Although levels of GSH did not change much during the 12-week intervention, trajectory over time manifest to reveal a significant increase in NEEM500 and NEEM250 compared to the placebo group (Table 13). Overall, daily supplementation with NEEM dose dependently improved the trajectories of measured inflammatory and oxidative stress markers over time in this population, such that more substantial improvements may be observed with longer treatment duration or in those with higher baseline levels.
Effect on Malondialdehyde (μM/L)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
Effect on Reduced Glutathione (μmol/L)
Values presented as mean ± SD.
P values were obtained using ANCOVA followed by Bonferroni's post hoc analysis.
Differences were considered significant at P < .05.
Platelet aggregation, lipid profile, and safety evaluation
Daily NEEM supplementation did not significantly affect platelet aggregation or lipid profiles (i.e., TC, LDL-C, VLDL-C, HDL-C, and TG) (data not shown). All safety parameters assessed remained within normal limits (Supplementary Data). Two patients in NEEM125 and one in NEEM250 reported mild gastrointestinal disturbance, but none of the subjects in any group discontinued the study due to an adverse event.
Discussion
This study has provided evidence that the standardized aqueous extract of A. indica leaves and twigs (NEEM) decreases oxidative stress, inflammation, and insulin resistance to improve glucose tolerance and vascular function over time in an insulin-resistant population. Insulin resistance and glucose intolerance are hallmarks of MetS and HOMA-IR is an established calculation to assess the presence and extent of insulin resistance. 25 HOMA-IR progressively worsened over 12 weeks in the placebo group, whereas diminishing insulin resistance was attenuated with the lowest dose of NEEM and decreased with increasing daily doses. Increases observed for FBS, PPBS, and HbA1c in the placebo group would have been greater without sufficient capacity to compensate with augmented insulin secretion, which is ultimately compromised over time with extended duration of insulin resistance to precipitate diabetes. Thus, it is critical to improve insulin sensitivity in populations with insulin resistance to prevent progression to diabetes.
Reduced antioxidant status and a heightened proinflammatory environment contribute to increased oxidative stress and reduced vascular endothelial NO production and bioavailability, 26,27 which, in part, explain reduced NO levels and impaired vascular function, thereby increasing CVD risk, in patients with MetS. 28 MDA is a by-product of lipid peroxidation and marker of oxidative stress, whereas GSH, the body's primary endogenous antioxidant, discourages lipid peroxidation by reducing oxidative stress, but can be diminished in the face of chronic oxidative stress characteristic of MetS. Also, proinflammatory cytokines (IL-6 and TNF-α) and hsCRP are significantly elevated in obesity, MetS, and type 2 diabetes mellitus, all conditions characterized by reduced glucose tolerance. 29 Treatment with NEEM for 12 weeks generally improved the trajectories for markers of vascular function, inflammation, and oxidative stress, but extended treatment duration may be needed to observe more pronounced long-term improvements in similar populations.
The results of this clinical study build on previous studies in experimentally induced glucose intolerant animals. Oral administration of a hydroethanolic neem leaf extract enhanced tissue antioxidant levels and counteracted the increases in blood glucose, cholesterol, and TG, oxidative stress, and inflammation in streptozotocin (STZ)-induced diabetic rats. 16 An aqueous neem leaf extract was shown to normalize blood glucose, insulin, and lipid levels, as well as levels of insulin signaling molecules within skeletal muscle of high-fat diet-induced diabetic rats. 17 Hyperglycemia and oxidative stress lead to the formation of advanced glycation end-products (AGEs), which contribute to tissue damage and dysfunction with aging and various chronic disease states, including T2D. In STZ-induced diabetic rats, oral administration of a chloroform extract of neem leaves decreased oxidative stress and AGE formation to prevent kidney damage. 30 In another study, aqueous extracts of both neem leaves and bark, as well as neem seed oil, were all shown to lower FBS and lipid levels in alloxan-induced diabetic rats without any adverse effect suggestive of toxicity. 21 Other preclinical studies have demonstrated the anti-inflammatory effects of various neem leaf extracts to reduce proinflammatory mediators in different models characterized by increased inflammation. 31 –35 Thus, the results observed herein build on the preclinical evidence supporting the therapeutic effects of biologically active compounds derived from neem leaves in the context of cardiometabolic derangements associated with oxidative stress, inflammation, and insulin resistance. Future clinical research is warranted to investigate optimized effective dosing for different neem leaf extracts in the varying context of such conditions. For example, in our previous study investigating the safety and efficacy of NEEM in patients with T2D on stable metformin therapy, more substantial improvements in the same indices of glycemic control (i.e., FBS, PPBS, HOMA-IR, and HbA1c), vascular function, inflammation, and oxidative stress were observed with daily NEEM supplementation for 12 weeks, 22 revealing greater therapeutic potential in that population.
The main limitations of this study, as with our prior clinical study, 22 are the small sample size and short treatment duration. Future clinical trials investigating NEEM treatment for longer duration are warranted.
An important consideration with neem is safety as some neem products, such as neem seed oil, are known to contain azadirachtin and nimbolide, which can exhibit toxicity. The neem leaf and twig extract used in this study was extracted with water under mild conditions to minimize extraction of azadirachtin and nimbolide as verified by HPLC analysis. Furthermore, the observation of no remarkable impact on the various safety parameters evaluated in this study (hematological, hepatic, and renal biochemical parameters) supports the safety of NEEM intake at the investigated daily dosing of 250–1000 mg.
In conclusion, daily supplementation with a proprietary standardized aqueous extract of neem leaves and twigs (PhytoBGS) for 12 weeks significantly improved trajectories of glycemic control, endothelial dysfunction, inflammation, and oxidative stress over time in subjects with MetS, which may be anticipated to suppress the progression of glucose intolerance. A long-term study in prediabetic subjects is underway with the goal of reducing progression toward T2D.
Footnotes
Acknowledgments
The authors thank Natreon, Inc., New Brunswick, NJ, USA, for providing capsules of the investigational products and placebo, kits for biomarker measurements, and relevant literature. We thank Dr. Y.S.N. Raju, Professor of General Medicine, NIMS, and Dr. Sravanthi Illendulla (Ayurvedic physician) for their clinical support, and Mr. Ravi Bhatt (Outliers Statistical Consulting Services) for review of statistical analyses.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors thank Natreon, Inc., New Brunswick, NJ, USA, for providing capsules of the investigational products and placebo, kits for biomarker measurements, and relevant literature.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.