
Abstract
The aim of this article was to review experimental and clinical studies regarding the use of omega-3 fatty acids on the prevention and control of chronic inflammatory diseases with autoimmune background through the gut microbiota modulation. For this, natural omega-3 sources are presented emphasizing the importance of a healthy diet for the body's homeostasis and the enzymatic processes that these fatty acids go through once inside the body. The pathogenesis of ulcerative colitis and rheumatoid arthritis are revisited under the light of the gut microbiota dysbiosis approach and how those fatty acids are able to prevent and control these two pathological conditions that are responsible for the global chronic burden and functional disability and life-threatening comorbidities if not treated properly. As a matter of reflection, as we are living a pandemic crisis owing to COVID-19 infection, we present the potential of omega-3 in preventing a poor prognosis once they contribute to balancing the immune system modulation the inflammatory process.
Introduction
Agrowing number of people are affected by chronic inflammatory diseases (CID) also classified as noncommunicable diseases (NCD) by the World Health Organization (WHO). The NCDs are characterized by high morbidity index and they are the consequence of genetic, physiological, environmental, and behavioral factors. Poverty and malnutrition are closely linked to NCDs and 75% of the NCD-related deaths happen in low- and middle-income countries and, according to the last WHO report, 74% of deaths globally were owing to some NCD in 2019.
The most classic and notable examples of NCDs are ischemic heart disease, stroke, and diabetes, but cancer and obesity are also important conditions related to chronic inflammation. People who are already bearing CID such as ulcerative colitis (UC) and rheumatoid arthritis (RA) are at high risk to develop them. 1,2
As recent studies have shown both CIDs are closely related to gut dysbiosis triggering low-grade systemic inflammation, also known as metabolic endotoxemia, and autoimmunity processes, our aim in this literature review was to gather information about the use of purified or food-stuffed omega-3 polyunsaturated fatty acids (n-3 PUFAs), including α-linolenic (ALA), eicosapentaenoic (EPA), and docosahexaenoic (DHA) acids on the prevention or adjuvant therapy of RA and/or UC, because UC patients are at high risk to develop RA, mainly caused also by gut dysbiosis and gut barrier impairment. 3 –5
The benefits of n-3 PUFAs-rich diets are correlated with the gut microbiota balance, which is correlated to metabolic disease prevention and health promotion for the consumers (Figure 1).

The role of the omega-3 PUFAs sources consumption in gut microbiota homeostasis, which are correlated with health improvement and metabolic diseases prevention. AA, arachidonic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; PUFAs, polyunsaturated fatty acids; SCFAs, short-chain fatty acids.
This review was conducted following the gastrointestinal tract natural flow, starting from the class of molecules (omega-3 fatty acids) intake (oral) to the direct effects of these acids on UC and/or RA by their anti-inflammatory properties (local effects on joints and or intestinal mucosae) or indirect effects on both chronic inflammatory conditions through gut microbiota modulation. Finally, we present a link on how microbiota imbalance acts as a trigger on both chronic inflammatory conditions beyond hereditariness and how omega-3 fatty acids ingestion could prevent the occurrence and/or a poor prognosis by keeping gut homeostasis.
Omega-3 Sources
Omega-3 (ω-3 or n-3) fatty acids are essential PUFAs (cannot be biosynthesized by the mammalian body, including humans and are exclusively obtained from dietary intake), chemically present 3 to 6 double bonds in their molecules, the first double bond of which is found in position 3 from methyl-end; thus, ALA, EPA, and DHA are physiologically the most important.
The primary sources of omega-3 PUFAs comprise crop leaf green vegetables, marine algae and microalgae, seeds and nuts, vegetable oils, fish and fish oils, as summarized in Table 1.
Sources of Omega-3 Polyunsaturated Fatty Acids and Their Contents
ALA, α-linolenic acid; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; PUFAs, polyunsaturated fatty acids.
The n-3 PUFAs are abundant in vegetables and fish origin sources. Thus, ALA is the highly found in vegetable foodstuff, vegetable oil (19–55%) followed by nuts and seeds (3–23%). 6 –13 Likewise, ALA, EPA, and DHA are highly found in microalgae species (42–60%, 13–31%, and 2–14%, respectively). 14 In addition, these three fatty acids are found in macroalgae species (EPA, 3–27% and DHA, 1–5%) and freshwater fishes (ALA, 1–4%; EPA, 0.4–3%; and DHA, 2–8%). 15 –17 EPA and DHA are found in marine fish and fish oil (3–6% and 13–33%; 6–13% and 4–18%, respectively). 11,18,19
The n-3 PUFAs quantities of all reviewed vegetables, nuts and seeds, vegetable oils, micro and macroalgae, freshwater and marine fishes and fish oil given in Table 1 are summarized in Figure 2.

The mean percentage of α-linolenic, eicosapentaenoic, and docosahexaenoic acids found in vegetable, algae, and fish origin sources. ALA, α-linolenic acid.
Green leaf vegetables, pods, nuts, fruits, microalgae, including their oils are natural sources of ALA. Therefore, the recommended daily intake of ALA is 1 and 2 g/day for women and men, respectively, and ∼1–4 g/day of EPA and DHA (abundant in microalgae, fish, and fish oil) are needed to maintain the gut microbiota balance and host health. 20 –23 In the organism, through the serial desaturation and elongation of biochemical reactions, ALA from the diet is converted to EPA and DHA, which are carried into the bloodstream, promoting several health benefits, including prevention, managing, and control of different types of diseases including autoimmune diseases. 24 –29
The bioconversion processes of ALA to long-chain PUFAs as EPA and very-long-chain fatty acids as DHA are given in Figure 3.
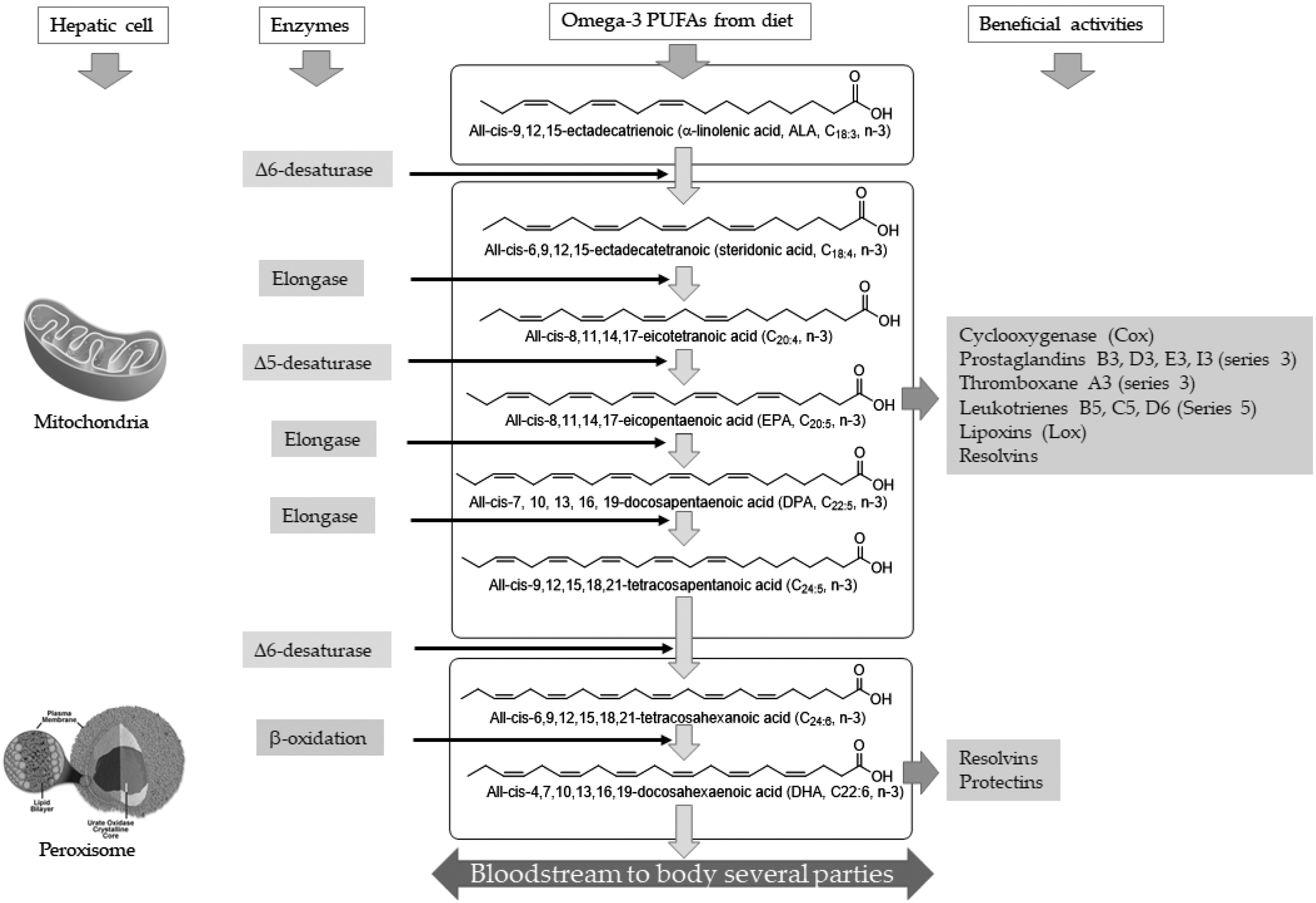
Biosynthesis pathway conversion of ALA to LC-PUFAs and VLCFAs in the human body. Among the LC-PUFAs, EPA and DHA to VLCFAs are the most important. These two acids are associated with human health promotion and preventing several diseases. The VLCFAs bioconversion process takes place in hepatic cell mitochondria and peroxisome. These acids enter the bloodstream, which are conducted to different body parts for health benefits, including prevention, control, and cure of various autoimmune diseases. LC-PUFAs, long-chain polyunsaturated fatty acids; VLCFAs, very long-chain fatty acids.
Previous clinical studies reported the benefits of n-3 PUFAs (≥4 g), individual EPA (∼2 g) or mixed EPA (0.05–2 g), and DHA (0.03–1 g) daily ingestion or supplementation decreased the effects of UC and RA in human subjects significantly. 30 –36 High intake of n-3 PUFAs is associated with an abundance of short-chain fatty acids (SCFAs) gut microbiota producers and intestinal health improvement, reducing inflammatory diseases. 23,29,37,38 Conversely, the increase of beneficial gut microbiota directly reduces the occurrence of harmful microbiota characterized by the presence of lipopolysaccharides (LPS) in the cell surface of Gram-negative bacteria that act as an inflammatory trigger when interacting with cell surface receptors of the macrophage and neutrophils of host's immune system. 38
Furthermore, the abundance of EPA and DHA (n-3 PUFAs) with anti-inflammatory effects (resolvins, protectins, and maresins) competes with arachidonic acid (n-6 PUFAs), which is a pro-inflammatory precursor of prostaglandin (PG) and leukotriene (LT) synthesis at the cyclooxygenase (COX) and lipoxygenase (LOX) level, which modifies cell membrane phospholipid fatty acid pattern, disruption of lipid rafts for healthy physiology conditions by inhibition of the proinflammatory cytokines, as tumor necrosis factor-α (TNF-α), interleukins (ILs): IL-1, IL-6, IL-8, and IL-12, nuclear factor kappa B (NF-κB), COX-2, LOX, cytochrome P450, nitric oxide, G protein-coupled receptor 120, LTs, and peroxisome proliferator-activated receptor-γ regulation. 39
In addition, EPA and DHA are related to the decrease in the production of cytokines, T cell reactivity, PGE2 metabolites, thromboxane A2 (linked to platelet aggregation and vasoconstriction), leukotriene B4 (inflammation and potent inducer of leukocytes, lymphocytes, macrophages, endothelial cells chemotaxis, and adherence) and IL-6 and the increase of thromboxane A3 (weak platelet aggregation and vasoconstrictor), prostacyclin PGI3 and PGI2 (vasodilators and inhibitors of platelet aggregation), leukotriene B5 (low inflammation and chemotactic agent). 40 –44 Thus, EPA and DHA-rich diets or supplement intake have central role correlated with decreasing and preventing incidence of RA and UC effects on human subjects. 44 –50
UC and RA Pathogenesis: Then and Now
In the past, UC and RA were identified mainly through the observation of the symptoms, and both had in common the prerogative of genetic background and a chronic inflammation status at the committed sites, rectum/colon and joints, respectively. The symptoms of UC are abdominal pain, diarrhea, and hematochezia (passage of fresh blood through the anus) but not all cases of colitis present blood in stools, for example, microscopic colitis. Anemia, high erythrocyte sedimentation rate (ESR), or C-protein level may be present on blood tests; however, it is not a rule, the endoscopic biopsy confirming the clinical diagnosis. 51
The main affected sites in UC are the rectum and colon and it is characterized by an impaired intestinal lining owing to chronic inflammation and the presence of ulcerative lesions; if not treated, it can lead to dangerous conditions such as toxic megacolon or colorectal cancer. 52
Of interest, several studies published since the 1960s until now from different populations, that is, different genetic backgrounds, point to arthritis/polyarthritis as the most common extraintestinal manifestation of UC, corroborating a common etiology in both diseases (Table 2). Those observations showed that there were shared environmental factors, regardless of genetic inheritance, triggering the onset of UC and/or RA in genetically predisposed people, such as food habits. 53 –58
Most Frequent Extraintestinal Manifestation in Patients With Ulcerative Colitis on Different Populations
EIMs observed only in UC patients.
Type 1 arthritis: commitment of < 5 joints/it can be asymmetrical; type 2 arthritis: commitment of 5 or more joints symmetrically (RA).
EIMs, extraintestinal manifestations; IBD, inflammatory bowel disease; RA, rheumatoid arthritis; UC, ulcerative colitis.
Another CID with an autoimmune background is RA. Its symptoms are primarily swollen and painful joints, especially the smaller ones such as those from fingers, hands, feet, wrists, and temporomandibular; however, it is also common in the bigger ones like knees, hips, and shoulders. Another characteristic of RA is morning stiffness when joints' swelling is greater before getting up with motion impairment and tends to be ameliorated throughout the day. If not adequately treated, the host's autoimmune response tends to promote extracellular matrix degradation and osteoclasts' activity leading to cartilage, ligaments, tendons and bones weakening, and destruction leading to functional impairment. 59
A recent study demonstrated that this is a distinct pathophysiologic phenomenon characterized by fibrin clots associated with neutrophils deposited along the synovial lining, and it was found to be associated with DAS28 score and duration of ≥1 h of morning stiffness. 60
Beyond joint inflammation, RA can also present some extra-articular consequences such as subcutaneous or lung rheumatoid nodules, interstitial lung disease, dry eye syndrome (keratoconjunctivitis sicca), vasculitis, and consequently a higher risk of cardiovascular diseases, hematologic abnormalities (ESR, C-protein level, anemia, and plasma viscosity improvement), and consequently a higher risk of stroke. 59
In this way, RA has to be considered a syndrome caused by genetic, epigenetic, and environmental factors. This multifactorial behavior allows opportunities for searching what environmental factor could be changed or modulated to prevent epigenetic processes (DNA methylation or histones acetylation) or to control the disease activity leading to a remission state. The genetic background is mainly related to DNA loci associated with immune mechanisms, shared with other CIDs, generating autoantibodies (rheumatoid factor, anti-cyclic citrullinated peptide, among others); however, they are absent in 30–50% of patients at diagnosis, known as seronegative RA patients. 61,62
Environmentally speaking, once the low socioeconomic status is also considered a risk factor, the nutritional quality of food intake could also be considered a risk factor. A poor nutritional status with a lack of fibers, vegetables and fruits, considered prebiotics, could favor a gut dysbiosis promoting epithelial barrier impairment, inflammatory processes, and metabolic endotoxemia. 63
OMEGA-3 on UC and RA
UC is a CID characterized by a gut disorder of the large gut, which is marked by the destruction of the bowel mucosa and intractable ulcers. 63 –65 In contrast, RA is an autoimmune disease and systemic inflammatory disorder characterized by chronic synovitis and cellular infiltration, often leading to bone joint erosion, cartilage destruction, and disability, if not treated. 66,67
Thus, these two dysbiosis-related inflammatory conditions could be managed by n-3 PUFAs, including EPA and DHA administration in diet or supplementations. 40,47,49,68,69 The beneficial effects of n-3 PUFAs diet and supplementation on UC and RA subjects are given in Table 3.
Effect of Omega
↓, significant decrease; ↑, significant increase; ↔, unchanged; COX-2, cyclooxygenase 2; FFA, free fatty acid; ICR mice, albino mice originating in SWISS from the Institute of Cancer Research (USA); IL, interleukin; MAG, monoglyceride; NSAID, nonsteroidal anti-inflammatory drug; TNF-α, tumor necrosis factor-α.
Several studies have reported the positive effects of n-3 PUFAs, including EPA and DHA, on controlling and decreasing the activity of various CID, especially UC and RA (Table 4). The results of some studies demonstrated lowering UC and RA effects on animal models and human subjects with the administration of n-3 PUFAs (EPA + DHA), seafood, fish, and fish oil on a short-term (1–4 weeks) to measure the disease activity and in a long-term (6 months to 26 years) as lifestyle educational diet. 35,48,73,81,82 Therefore, it is the most important to highlight that decreasing of UC and RA activity may be associated with the balance of gut microbiota, especially Bacteroidetes-to-Firmicutes ratio, Actinobacteria, Proteobacteria species, and SCFAs producers, which are related to host health. 23,26,29,64,72,83,84
Effects of Omega
HFD, high-fat diet; T2DM, type 2 diabetes mellitus.
OMEGA-3 on CID and Gut Microbiota
The gut is a complex tract through which food and its metabolites pass during the lifetime. Furthermore, it is the home to ∼100 trillion dynamic microorganisms with 35,000 strains of bacteria, of which 107–108 cells/mL are located in the small intestine, and 1010–1011 cells/mL are present in the large intestine. 83,85,86 This microbiota is constituted mainly by anaerobic strains with ∼98% formed by Bacteroidetes Phyla (9–42%, Porpyromonas and Provotella), Firmicutes (30–52%, Ruminococcus, Clostridium, and Eubacteria), and Actinobacteria (1–13%, Bifidobacterium), whereas another 2% is composed of Lactobacilli (2%), Streptococci (2%), and Enterobacteria (1%) Phyla. 29,87 –90
Furthermore, this gut microbiota composition varies among human subjects, and it may be determined by ethnic/tribal/racial, geographical location, dietary habits, and environmental conditions. 92 –95 Thus, a high diversity composition of Bacteroidetes/Firmicutes, Actinobacteria, Proteobacteria, and Verrucomicrobia strains are correlated with healthy human subjects. 29,93 –95
However, adverse conditions such as inflammatory chronic disease environment are correlated with different kinds of cancer, inflammatory bowel disease, diabetes, neurodegenerative syndromes, cardiovascular disease, multiple sclerosis, obesity, central nervous system syndromes (stress, anxiety, and depression), and others, resulting in gut microbiota imbalanced system caused by the diet profile. 29,90,93 –98
In addition, several studies have shown that long-term intake of n-3 PUFA-rich foodstuffs are correlated with several diseases prevention or health improvement, avoiding the prevalence of gut dysbiosis on animal models and human subjects. 29,96,99 –101 The first benefit of n-3 PUFAs-rich foodstuffs is linked to gut microbiota harmony balance, creating an efficient barrier, which manages the harvesting energy in the body and controls several associated diseases. 29,103 –107 Thus, the benefit of an n-3 PUFA-rich diet, including ALA, EPA, and DHA, is related to decreasing or managing CID, and the balance of gut microbiota on animal models is given in Table 4.
The increased Bacteroidetes-to-Firmicutes ratio, including Actinobacteria and Proteobacteria strains, was demonstrated with feeding n-3 PUFAs (ALA, EPA + DHA), maternal, flaxseed, fish, and algae oils in high-fat diet and n-6/n-3 proportion (1/2) on animal models (Table 2). The results showed the decreased effects of obesity, type 2 diabetes mellitus, inflammatory bowel diseases (IBDs), body weight, nonalcoholic steatohepatitis, adipose tissue, and insulin resistance. 109,112 –116
In addition, the balance of the Bacteroidetes-to-Firmicutes ratio is the most important, linked to the increasing SCFA (acetate, propionate, and butyrate acids) production in the gut, which is the leading biofuel used by several colonocytes that promote the healthy environmental hemostasis among the systems in the body, protecting against pathogenic agents' entrance and, consequently, various CID. 23,26,29,83,84,91,106,117 –122
On the contrary, the unchanged body weight was reported in n-3 PUFAs (EPA = 40% plus DHA = 27%) administrated to healthy models for 2 weeks, which may be explained by the short study time. Likewise, with human subject studies, the same results were reported as found in animal models (Table 5).
Effects of Omega
Gut Microbiota Autoimmunity Axis
The gut microbiome is built from the very first day of birth. The composition may change according to the mode of delivery; when naturally delivered, the newborn will acquire bacteria mainly from the mother's vaginal tract and when through C-section, mainly from the mother's skin surface. Another variant is, if the baby was breastfed, the quality of its immunoglobulin and neutrophils in the colostrum/milk. Later, in childhood, other factors may interfere in the gut microbiome, such as environment, diet, and rate of infections the child could develop, and also the genetics interferes with the gut microbiome. 124
Recent studies have shown that gut dysbiosis could be an early event, previous to the clinical onset of CIDs such as UC and RA, triggering the autoimmunity on genetically predisposed people. A balanced gut microbiome is the coexistence of beneficial (commensal and symbiotic) and harmful (pathogenic) microorganisms being supported by the ingestion of food considered prebiotics, whereas the consumption of high-fat and refined carbohydrate, and low-fiber and resistance nutrients diet or the crescent use of antibiotics could promote an imbalance into this highly complex system of bacterial community. 3,29,125,126
In fact, a decreased bacterial diversity in gut microbiota was found in new-onset untreated RA and psoriatic arthritis patients, which resembles the same dysbiosis also found in IBDs. Indeed, a predominance of Prevotella copri is correlated with the reduction of the other beneficial Bacteroidetes strains. In addition, when P. copri is transplanted to an in vivo model of chemically induced colitis, it can spread and dominate the gut microbiome, increasing the sensitivity to the chemical. 127 –129
An imbalanced gut microbiota promotes local inflammatory processes activating the local innate immunity, such as macrophages and dendritic cells that under the action of cytokines are differentiated into antigen-presenting cells (APCs), disrupting the epithelial barrier, promoting intestinal permeability, and favoring the influx of bacterial DNA and/or LPS to the bloodstream. 5,130
This local process may allow the failure of tolerance mechanisms by epitope spreading caused by a change of proteins structure owing to citrullination, molecular mimicry when some pathogens share the same sequence or structure also found on the host's organism, bystanders activation caused by bacteria stimulation of Toll-like receptors on APCs leading to a production of proinflammatory cytokines and tissue damage, and under prolonged infection, causing constant activation of T cells, overproduction of antibodies, and immune complexes. 124
Once in the bloodstream or the lymphatic vessels, activated immune cells or bacterial antigens (LPS and or DNA) are directed to the joints, and local cytokines activate resident dendritic cells, B cells, T cells, and natural killer (NK) cells, leading to activation of a complement system enhancing synovial inflammation. 130 Corroborating the gut dysbiosis/loss of immune tolerance hypothesis, Kempsell et al. 131 were able to identify several bacterial ribosomal RNA in arthritis synovial tissue and controls; however, some strains were unique to arthritic synovial tissue indicating living bacteria in the joints. The link between the genetic background and environmental factors leading to gut dysbiosis and collaborating with UC and RA pathogenesis is given in Figure 4.
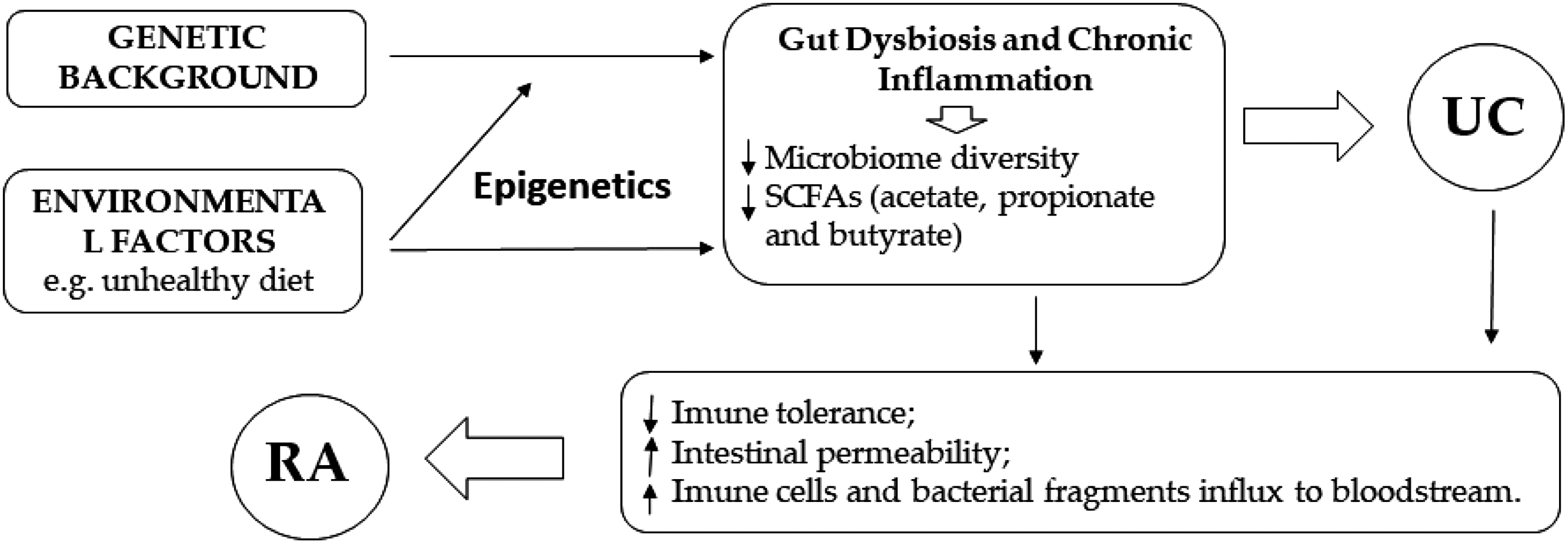
Theoretical scheme of the link between UC and RA pathogenesis having in common the gut dysbiosis. RA, rheumatoid arthritis; SCAFs, short-chain fatty acids; UC, ulcerative colitis.
Another dysbiosis-prone site is the mouth, specifically Porphyromonas gingivalis, the leading cause of periodontal disease. This strain is well studied and correlated with RA and the citrullination mechanism generating post-translation protein modifications through bacterial enzymatic activity and later producing anticitrullinated protein/peptides antibodies. 132 Besides the citrullination process, P. gingivalis could also promote an aggressive type of RA in an animal model by induction of NETosis (when neutrophil aggregate emits thin evaginations of their cell membrane forming a kind of network to contain pathogens and which also promotes platelet entrapment), osteoclastogenesis, and Th17 proinflammatory response. 133
The idea to modulate the gut microbiota for prevention or as adjuvant therapy in CIDs such as UC and RA is not new. Fasting studies in RA patients followed by a vegetarian diet, which is rich in prebiotics, demonstrated that the change of diet could improve the outcome of the disease, having a long-term effect both clinically and statistically. 134
Prebiotics are considered food products or by-products that promote the growth and maintenance of a healthy and diverse gut microbiome capable of producing higher levels of SCFAs metabolites, especially butyrate, which has the capacity of inhibiting inflammatory pathways by suppressing NF-κB activity and the expression of IL-1, IL-12, and TNF-α (proinflammatory cytokines), inducing mucin synthesis and in this way protecting the intestinal mucosa, and decreasing the bacterial influx from the intestinal lumen to the bloodstream by improving the tight junctions on intestine epithelial cells. 29,44,132 –138
One of the prebiotics we highlight is omega-3 fatty acids, well-studied by several researchers in several experimental and clinical studies. Results have shown their gut microbiota modulation property favoring butyrate producers and anti-inflammatory properties for being precursors of EPA and DHA-derived eicosanoids, resolvins, and protectins, driving the inflammatory process to its control and resolution and avoiding tissue damage. 29,138
It is proposed that switching the immune cell membrane composition of a higher proportion of arachidonic acid, caused by high intake of omega-6 foodstuffs, into a higher EPA and DHA proportion, owing to an intake of omega-3 foodstuffs, may favor the production of less potent eicosanoids, by COX- and LOX-mediated enzymatic reactions, generating an anti-inflammatory profile driving to control and resolution of the inflammatory process in the gut, in the case of UC or in the joints, in the case of RA. Indeed, it was already observed that consumption of omega-3 ameliorates the rates of RA remissions and improves the maintenance of remission on IBD patients (Fig. 5). 44,45,52,96,139
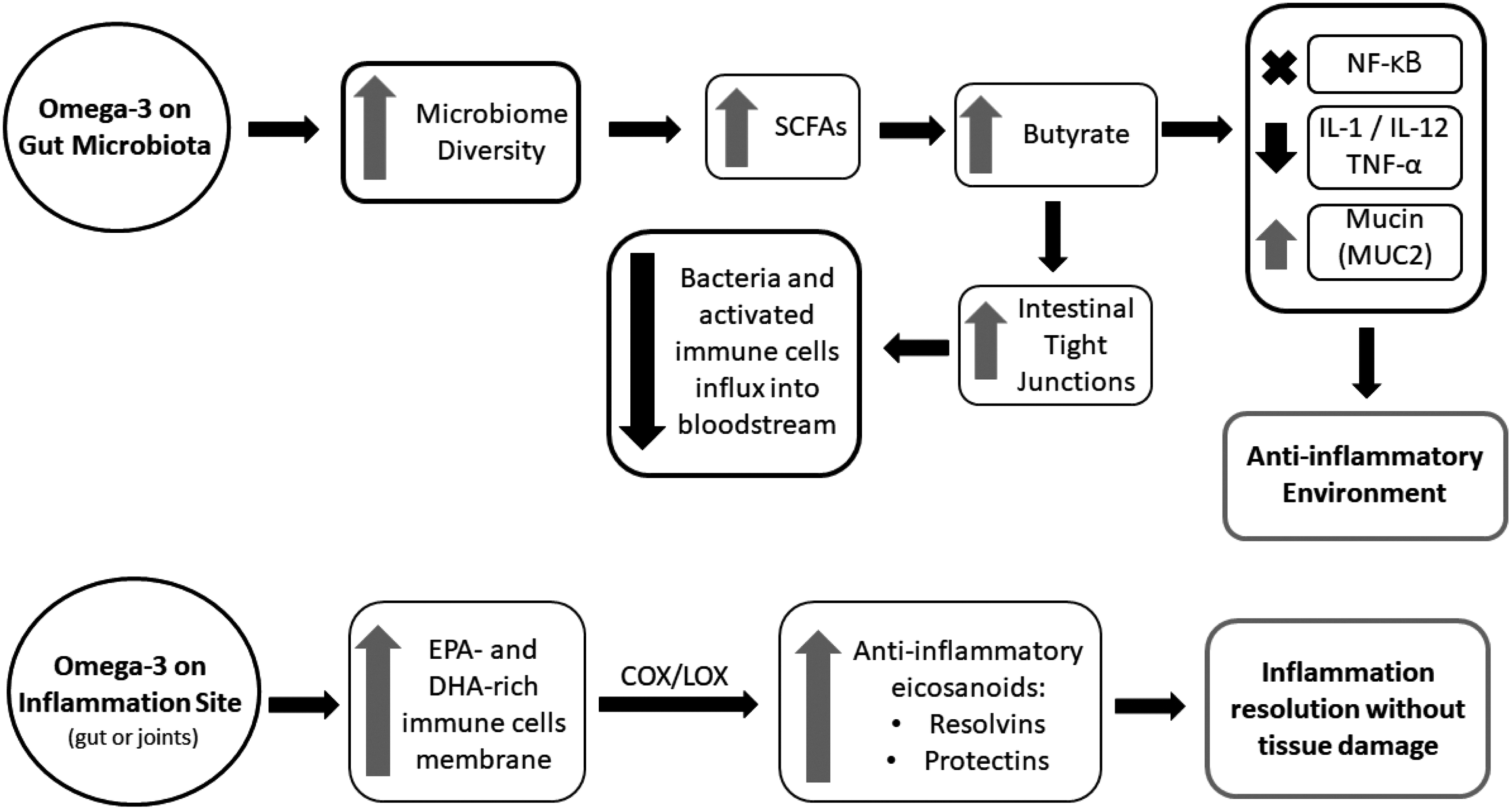
Summary on how omega-3 fatty acids can act improving gut health and switching the organism to an anti-inflammatory profile by modulation the gut microbiome and/or by immune cells membrane composition. COX, cyclooxygenase; IL, interleukin; LOX, lipoxygenase; NF-κB, nuclear factor-kappa B; TNF-α, tumor necrosis factor alpha.
Conclusions
The CID social and economic burden is a concerning issue once its prevalence keeps increasing throughout the decades, lowering the quality of life, and overloading government budgets and health systems. 140 Malnutrition, that is, lack of vegetables, fruits, and fibers intake and high consumption of meat and high-fat diets, drives to gut microbiota dysbiosis and a subclinical inflammatory status, not initially detectable on routine exams but in the long-term leading to several chronic diseases, including UC and RA, among them. 141 Omega-3 fatty acids have been widely tested in clinical and experimental studies, and its anti-inflammatory action has always been corroborated in various diseases, including the aim of our review, UC and RA, through inflammatory factors suppression or modulation of the gut microbiota as previously described.
Besides the benefits of preventing or as an adjuvant treatment for UC, RA, and many other chronic pathogenic conditions, researchers are already calling attention to the benefits that omega-3 fatty acid supplementation could provide on COVID-19 treatment and recovery once the leading cause of death is related to an inflammatory cytokine storm/cascade in the lungs causing respiratory failure because most comorbidities are associated with NCDs, CIDs, and autoimmune diseases. However, an official treatment recommendation just may be made after randomized and controlled clinical trials. 142 –144
Finally, it is considered most important to have a healthy diet based on functional foods or, if it is not possible, carrying out a nutrient supplementation under prescription, which can contribute to gut microbiota balance and, as a consequence, on a controlled immune system, especially under a double pandemic scenario humanity is facing: the inflammatory chronic disease pandemic and the COVID-19 pandemic at the same time. 145 Further preclinical and clinical trials are demanded in this field of research, engaging a multidisciplinary team with a holistic view of pathological processes.
Footnotes
ACKNOWLEDGMENTS
The authors thank the Graduate Program in Biotechnology and Biodiversity and the Graduate Program in Health and Development in the Central-West Region, Federal University of Mato Grosso do Sul-UFMS, for support. The authors also thank the Coordination for the Improvement of Higher Education Personel (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—CAPES) and the National Council for Scientific and Technological Development (Conselho Nacional de Desenvolvimento Científico e Tecnológico—CNPq) for research grants.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This research was funded by the Federal University of Mato Grosso do Sul (UFMS) and Coordination for the Improvement of Higher Education Personel (CAPES)—Portaria 2016/2018. This study was financed in part by the CAPES—finance code 001.