
Abstract
The progression of SARS-CoV-2 (COVID-19) in humans heavily depends on the patient's overall health status, especially on its immunoregulatory capacity. Different plants and plant-derived preparations (infusions, encapsulated, etc.) have been used as immunoregulators, several of them with scientific support. Nevertheless, due to the composition complexity of such plant-derived preparations, the molecular and physiological mechanisms involved in their beneficial effects remain, in some cases, unclear. In this review article, the most reported plants used in traditional medicine to enhance immunoregulatory capacity are presented, and their effect on the innate immune response is discussed and correlated with their respective phytochemical profile. Understanding how the plant phytochemical profile relates to the observed impact on the innate and adaptative immune response is fundamental to designing plant-derived co-treatments to lessen the symptoms and favor the recovery of COVID-19 patients. In this regard, we propose a prospective guideline for using plants and plant-derived preparations as co-treatments for COVID-19 (and similar viral infections), which could be helpful in the context of the worldwide effort to end the current SARS-CoV-2 pandemic.
INTRODUCTION
The actual SARS-CoV-2 (COVID-19) pandemic has made evident the importance of a well-regulated immune system for preventing a severe inflammatory response and reducing the spread of infection in the general population. Due to all the new information that has been published regarding COVID-19, we are now able to understand the pathology and clinical evolution of the infection. In this regard, it is known that COVID-19 infection can be divided in three stages: (1) asymptomatic period (incubation), (2) nonsevere symptoms, and (3) severe symptomatology. 1 The severe stage is clearly characterized by an uncontrollable inflammation response due to tissue damage or a dysfunctional immune response. 2 This acute stage is also characterized by a reduction of B and T lymphocytes in peripheral blood, especially CD4+ and CD8+ lines; interestingly, viral load and inflammation factors increment in a similar pattern. 3,4
These inflammation factors, usually cytokines, upregulate the inflammation development along with activation and differentiation of cells, such as macrophages and NK cells, which will release proinflammatory cytokines.
The immunologic aspect of SARS-CoV-2 is unquestionable and similar to that of SARS-CoV-1, the later also characterized by the presence of several proinflammatory cytokines and transcription factors. 5 The complex pathogenesis of SARS-CoV-2 hampers the development of specific drug therapies. Although an efficient antiviral drug could be promptly available, COVID-19 will still be a multimedication treatment disease, especially to overcome tissue damage due to the acute inflammation response. The first attempts for SARS-CoV-1 vaccine development were hampered precisely by the magnified inflammatory response derived from the vaccination. 6
Unfortunately, SARS-CoV-2 will probably be from this point forward a recurrent and widespread disease in the world with dispersed outbreaks points. For this reason, it is necessary to develop treatment options for SARS-CoV-1, MERS-CoV, SARS-CoV-2, and related diseases with similar immune molecular pathology. In this context, plant-derived isolates may be an alternative for helping in the treatment of viral infections and immune-related diseases. 7 Plant-derived preparations usually have a plethora of effects in the organism, including immune-regulating activity. Focusing on the pharmacological application of these plant-based preparations can help deal with the current SARS-CoV-2 pandemic and future outbreaks.
Typically, plants isolates administered to animal models and humans can exert a modulated immune response activity, either stimulating or decreasing, depending on the metabolic state of the organism. In a basal state, they usually have an immune-stimulating effect. On the other hand, under an inflammation state, they generate a counter-response by decreasing the synthesis and liberation of proinflammatory factors. 8
Although plant-derived preparations have been used since the beginning of human history, most of their properties are known by observational learning. This is particularly true in countries such as Mexico, where the wide variety of endemic plants makes traditional medicine quite diverse. The importance of plant-based medicine also relies on the actual trend to use products generally perceived as “natural” by the general public. In Mexico, plant-based medicine is often more acceptable due to traditions and accessibility to all the population. 9
A comprehensive analysis at the clinical and molecular level of bioactive compounds in plant-derived preparations is indispensable for the safe use of traditional medicine. Despite the vast diversity of traditional medicine in countries such as Mexico and China, the attempts to describe their pharmacodynamics are still scarce. This understanding would allow a rational combination between traditional and modern medicine to achieve synergistic effects, which in the context of the current COVID-19 pandemic may be of particular relevance. 10
In this review, we present an analysis of the immune-regulating activity, from a physiological and biochemical perspective, of plants and plant-based preparations reported in literature to have confirmed or potentially used as treatments for bacterial and viral infections. Plants such as Salvia rosmarinus, Aloe vera, Taraxacum officinale, Allium sativum, Carica papaya, Verbascum genus, Echinacea genus, and Plantago genus have been included as examples to contextualize the physiological mechanism involved in their immune-regulating activity, in an attempt of giving a scientific vision to the use of traditional plant-based medicine. Finally, we propose a strategy for the usage of medicinal plant-derived preparations for complemented treatment and prevention of COVID-19.
METHODOLOGY
In this literature review, plants species/genus were selected by an escalated search in different databases. The initial keywords used were as follows: “therapeutic plants, immunoregulation, and anti-inflammatory.” The search motors used included the following: Elsevier, Mendeley, Scopus, Google Scholar, PubMed Central, and SpringerLink through Tecnologico de Monterrey library system. The plants' species/genus were selected based on their availability, cost, and published research available from the first obtained pool. The plants' species/genus effect on the cytokines and NF-κB was used as a third filter. Only the plants' species/genus with a concrete effect on related inflammatory cytokines and NF-κB were selected for the presented literature review.
A BRIEF INTRODUCTION TO INNATE IMMUNE RESPONSE DURING INFECTIONS
To understand how plant-derived preparations may have immune-regulatory activity, it is important to analyze the main elements constituting the immune system. Complex organisms have developed an intricate strategy to overcome any possible infection, either external or internal. This strategy is called, in general terms, immune response. The importance and complexity of the immune system have made of its study a complete and multidisciplinary field. The immune response can be divided as innate and adaptive.
Different organisms share innate immunity mechanisms, unlike adaptive immunity, shared only between vertebrates. Due to its broad spectrum of action and quick answer to pathogen exposition, the innate immune response is crucial for immediate and effective infection suppression. Myeloid and lymphoid cell types and nonhematopoietic cells, such as epithelial cells (from different tissues), participate in this intricate innate response. The participating cells have different signaling routes, which are triggered by the quick recognition of the pathogen. An inflammatory response in the innate immune activation is expected and needed for the signaling response, although a decompensation can lead to allergies or autoimmune diseases.
Thus, understanding the activation of the response at molecular levels is especially important for the appropriate management of inflammatory chronic and acute responses to infection. 11,12 Figure 1 presents a simplified diagram of the innate immune response activation and cytokine liberation cascade. Innate immune response is promptly activated by the pattern recognition receptors (PRRs) present in the membrane and endosome antigen-presenting cell (APC). Pathogens are detected as pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs), triggering an intricate network of activation and regulation of inflammatory-related genes. This gene activation process derives in the liberation of cytokines and chemokines as a cell response. Simultaneously, cytokines and chemokines regulate their own production and liberation.

Innate immune response activation and cytokine liberation cascade. Innate immune response promptly starts when the pathogen is recognized by the PRRs presented in the membrane and endosome of an APC. Different molecules from the pathogen can be recognized, such as proteins, carbohydrates, lipopolysaccharides (LPS), and nucleic acids. This recognition starts the cell response of the APC by the liberation of cytokines and chemokines, which at the same time play a role as regulative factors for their self and different cytokines and chemokines. The cell response in the target cell for cytokines and chemokines results in the activation, maturation, migration, or even growth inhibition of the cell line. An example of this is the differentiation of naive T cells into Th1, Th2, and Th17 cells. APC, antigen-presenting cell; PRRs, pattern recognition receptors.
Recognition of PAMPs and DAMPs
Infections trigger the innate immune response by different means, depending on the area of infection and nature of the pathogen itself. The innate immune response is quickly activated by the recognition of PAMPs or DAMPs by PRRs. The pathogenic origin and biochemical nature of the PAMPs and DAMPs are linked to the PRRs response. Recognized PAMPs and DAMPs are often proteins, carbohydrates, lipopolysaccharides (LPS), and nucleic acid molecules. Five types of PRRs have been identified: (1) C-type lectin receptors, (2) Toll-like receptors, retinoic acid-inducible gene 1-like receptors, (4) nucleotide oligomerization and binding domain-like receptors, and (5) pyrin-HIN domain receptors. 13
PRRs have a tight specificity to PAMPs and DAMPs to avoid an excess response, which could affect un-infected cells. This undesired response magnification is responsible for severe stages of chronic infections and immune-related diseases. Figure 1 briefly describes the initiation of the innate immune response and its development in different pathways. Membrane and endosomal PRRs in APC (such as macrophages, lymphocytes, and dendritic cells) recognize the PAMPs and DAMPs activating the APC and synthesis of cytokines and chemokines. At the same time, these molecules upregulate the synthesis of the same or different cytokines and chemokines, which also activate a cell response. 14
Importance of TNF-α, IFN-γ, and NF-κB
Pleiotropic cytokines TNF-α and IFN-γ are prominent regulators of the immune response. Both are immediately secreted by activated cells, especially macrophages, and in collaboration with other cytokines and chemokines (induced by them), they direct the signaling and cell response (Fig. 1). TNF-α is recognized as a proinflammatory mediator responsible for activating and recruiting the immediate defense mechanisms, having a particular effect on macrophages. TNF-α promotes the activation and recruitment of macrophages to the infection site; macrophages synthesize and liberate proinflammatory cytokines and lyse pathogens locally by the production of nitric oxide (NO). 15
TNF-α effects are synergistically upregulated by IFN-γ paring. IFN-γ is produced by several activated APCs and NK cells (previously activated by the APCs cytokines/chemokines). IFN-γ is a proinflammatory cytokine central to immune cell response due to its activity in the activation, growth, maturation, and differentiation of several participating cells. IL-12 and IL-18 have a synergic effect on the upregulation of IFN-γ in T cells. 16 IFN-γ enhances antigen presentation, promoting cell activation, differentiation of naive T cells to Th1 cells, and expression of MHC I and II. IFN-γ also upregulates the expression of reactive oxygen species and NO-producing enzymes. 17 IL-4 and IL-10 downregulate the IFN-γ production restraining long-term effects produced by this proinflammatory cytokine.
For this reason, IL-4 and IL-10 are depicted as anti-inflammatory cytokines; they also participate in the differentiation of naive T cells to Th2 cells. 16 Alongside TNF-α and IFN-γ, NF-κB is a critical player in the innate immune response. NF-κB refers to a family of transcription factors that regulated different related genes. 18 NF-κB pathway is activated by the cytokines generated from the APC activation, mainly TNF-α; at the same time, NF-κB induces the activation of proinflammatory cytokines (IL-1, IL-2, IL-6, IL-8, IL-12, and TNF-α). NF-κB is also responsible for the upregulation of chemokines, adhesion molecules, cell cycle regulators, and antiapoptotic factors. 18,19
Although the effects of NF-κB and proinflammatory cytokines, in the long run, can have unwanted consequences, their activation in the early stages of the infection can assure the proper control of the infection and the development of regulating pathways to return the response to basal levels. Impairing of proinflammatory cytokine responses in animal models produces an insufficient innate immune activity. 17,19,20 Several medical conditions in humans affect the overall immune response. These conditions can be direct, for instance, human immunodeficiency virus (HIV) infection or autoimmune diseases, or indirectly, such as obesity, diabetes, and cardiovascular-related diseases.
The indirect scenario defines a chronic inflammation state where an abnormal inflammatory response is constant, usually complemented with a loss of activity of the immune participating cells. Patients with diabetes or obesity have a higher risk of infection, and even mental stressful conditions can compromise the immune system. 21 –23 Clinical evidence of upper respiratory infections indicates that the disease development in psychologically stressed patients tends to aggravate, particularly in influenza infections. 24 It is important to consider the overall state of the immune response in patients from the indirect scenario; this consideration is usually unseen until the patient is in severe stages. In the actual SARS-CoV-2 pandemic, the mortality is highly related to the presence of risk factors, such as diabetes, obesity and cardiovascular disease. 25
IMMUNOREGULATIVE THERAPEUTIC AGENTS
Therapeutic agents that have an effect on the immune response should be carefully studied and implemented since such effects are interrelated with several systems, organs, and tissues. Usually, autoimmune diseases are the most prone to be treated with therapeutic agents directly affecting the immune system. Rheumatoid arthritis is generally treated with cell and cytokine blockers to evade its atypical immune response. 26
Cancer treatments also rely on therapeutic agents capable of enhancing the immune response responsible for the restriction of cancer cells. Some examples include the Bacillus Calmette–Guérin (BCG) vaccine, which is used as an adjuvant in the treatment of different types of cancer. Such vaccine would be considered immunotherapy due to its nonspecific immune response enhancing. 27 Glatiramer acetate is a recognized immunomodulatory agent used as an adjuvant in the treatment of multiple sclerosis. The mechanism of action of glatiramer acetate is not fully understood, although it is known that it promotes the change of Th1 cell differentiation to Th2 cell, reducing Th1-related inflammation; it also has a reducing effect in Th17 proinflammatory cytokines. 28
Specific immune therapeutic agents are scarce and expensive, but their use should be controlled and adjusted depending on the clinical response of the patient. In addition, at the moment, there is no specific agent oriented to enhance the innate immune response as treatment or prevention of infectious diseases, especially in vulnerable patients with chronic conditions. The search and development of molecules with a potential enhancing immune effect with a low toxicity window is an opportunity area that can be approached with plant-based traditional medicine, taking advantage of their relatively low cost, popular acceptance, and availability.
Effect of medicinal plant derivatives in the innate immune response
In traditional medicine, plant preparations with an immunoregulatory activity have been used in the treatment of diverse types of infections. 7,8 Common examples are skin and respiratory infections, including viral, bacterial, parasitical, and fungal. Influenza, tuberculosis, and malaria are diseases constantly studied and an important research area includes the search of natural compounds as an optional treatment. Plant-derived treatments, which have an immunoregulatory property, regularly act at cytokine, chemokine, hormonal, and neurotransmitter regulatory level. 29 Such preparations could be used as immunoregulation treatments against viral, bacterial, or fungal infections.
To better visualize the documented effect of plant-derived extracts and compounds in cytokines and proinflammatory factors (NF-κB), Figure 2 is presented. The selection of the reviewed plants is based in the scientific confirmation of their public domain known immunological effect. Quality and quantity of published studies in several models backing their effects, worldwide occurrence, and availability were also selection factors. In Figure 2, the plant-based preparations and extracts are arranged according to their reported overall response over the expression of cytokines and NF-κB. Blue marks indicate an upregulation of the cytokine/factor, whereas red marks indicate a decrease.

Effects of different plant preparations on the expression and activity of cytokines and NF-κB. Reviewed effects of the plant extracts/derivatives are summarized. Principal involved cytokines and transcription factors are presented. Columns marked with a “+” sign show cytokines and NF-κB (listed in the column to the left) with increased expression/activity. Columns marked with a “−” sign show cytokines and NF-κB (listed in the column to the right) with decreased expression/activity. The darker the square color tone, the higher the impact in the response. Species of genus Echinacea, Plantago, and Verbascum are specified.
Furthermore, the higher the intensity of the color the higher the relevance of the cytokine factor on the initiation and regulation of the innate immune response. In this context, IFN-γ, TNF-α, and NF-κB are considered the most relevant cytokines/factors as they are involved in different immune response-related pathways. As can be seen in Figure 2, certain plant preparations have demonstrated significant immunoregulatory activity, enhancing the immune response in a basal state, while downregulating during chronic inflammation conditions. Once naïve T cells are differentiated in Th1 and Th2, they can also release cytokines and factors that mutually regulate each other.
As summarized in Figure 2, A. vera upregulate and downregulate most of the cytokines reviewed, although A. vera effect over transcription factor NF-κB is only upregulated, as well as IL-8. Considering the role of cytokines and NF-κB (Fig. 2), A. vera has a significant effect on the overall response, which can translate into an immunoregulative function. 30,31 The models evaluated for A. vera derivatives included in vivo (rats and mice) with different inflammation models (bacterial and irradiation induced) and in vitro (LPS induced). 32 –35 The regulative effects were attributed to the high content of polysaccharides, as acemannan and aloeride, and some glycoproteins. 31,35 –37
Echinacea genus shares a similar pattern as A. vera, but the list of active compounds from Echinacea is more extensive in comparison. Echinacea extracts have an enhancing effect on the immune response by boosting the synthesis and liberation of proinflammatory cytokines affecting cell response directly. Furthermore, in induced inflammation, models are capable of decreasing the synthesis of proinflammatory cytokines (Fig. 2) through modulatory mechanisms. 38 –40 Echinacea effects have been tested in different cell lines, usually LPS induced.
Randolph et al, 41 tested E. purpurea extract in human trials showing a mild reduction of cytokines IL-1β, TNFa, IL-8, and COX-2, no serious adverse effect was found in the trial. 41 Along with the evaluations in Echinacea-induced immune response, toxicity assays have been performed. These assays usually show low toxicity, and in clinical trials, minor adverse effects are observed. 42,43 Patients who continuously use Echinacea complements do not show meaningful secondary effects associated with the long-term use. 44 These characteristics can be valuable for long-term treatments of immune-related chronic diseases.
Plantago genus preparations also show a dual effect, although its effect tends to the reduction of cytokines and factor synthesis. Nevertheless, Plantago major extracts enhance the production of the principal cytokines, TNF-α and IFN-y, which at the same time can directly affect the synthesis of different cytokines (Fig. 1). 45,46 In-vivo and in-vitro (lipopolysaccharide-induced) models were used for Plantago-derived preparations. 47 –49
Garlic (A. sativum) also shows an immunoregulatory effect, with some of the extracts showing a reducing effect in Th2 response differentiation. Figure 2 shows an equitable effect in the enhancing and decreasing of different cytokines. Considering the reviewed studies, NF-κB is not particularly influenced by A. sativum preparations. For A. sativum, in vivo (rats and mice) and in vitro models have been used; cells used in in vitro models were used directly or stimulated (Con-A or LPS). 50 –52 Fresh garlic was tested in a clinical trial, where they found that consumption of 2 g of fresh garlic elevates IFN type I, IFN-α, enhancing its reported antiviral properties. 53
Rosemary (S. rosmarinus) is commonly used as an anti-inflammatory remedy. Most of their preparations can reduce different cytokines, especially TNF-α and even NF-κB pathways (Fig. 2), showing an important anti-inflammatory effect in different in vitro models, usually LPS induced. 54 –58 Carnosol and carbon dioxide-supercritical extracts affect IL-4 and IL-10, and consequently, they may exert a regulatory response by directing Th1 cell differentiation instead of Th2. 59,60
Dandelion (T. officinale) preparations mostly have an enhancing effect over different cytokines. This enhancing effect is remarkably evident in the upregulation of TNF-α, and increasing NO production. 61,62 IL-10 was elevated in mice models, and all the in vitro models were LPS induced. 63 Dandelion has an antiviral activity over HIV-1 and H1N1; this effect, particularly in influenza, can be, in part, explained to its immunoregulatory activity. 64,65
The activity of leaves, seeds, and pulp of C. papaya has been studied, showing anti-inflammatory effect with a significant reduction of TNF-α, IFN-γ, and IL-6 levels in in vivo (rats and mice) and in vitro models, usually LPS induced (Fig. 2). 66 –70 The transcription induction of NF-κB factors after the inflammation response is reduced or inhibited by C. papaya preparations, having as consequence an anti-inflammatory effect. 66 C. papaya seed and leaf methanolic extracts were studied in a Listeria monocytogenes-infected male mice. Interestingly, the preparation elevated the levels of IL-12, which is an NK-stimulating cytokine. 70
Regarding the Verbascum genus-derived extracts and compounds, they have shown an overall anti-inflammatory response, phenylethanoid glycoside verbascoside being the main responsible for this effect. Verbascum preparations reduce IFN-γ and IL-6 cytokines and downregulate NF-κB in different in vitro models, explaining the overall anti-inflammatory effect. 71 –74 The methanolic extract from V. xanthophoeniceum aerial parts showed a higher response among the verbascoside preparations. This preparation decreased the IFN-γ, IL-6, and IL-10 levels. 73 The effect over IL-6 and IL-10 points to a reduction not only of the Th1 differentiation but Th2 as well.
Plant-based preparations can have multiples effects at different levels and their chemical nature is extremely important for understanding the pharmacodynamics of the bioactive compounds. It is also important to consider that usually the effect of the bioactive compound can be enhanced in a synergistic manner.
Phytochemistry and related species
To predict potential synergistic effects between plant-based preparations with other traditional or modern treatments, it is relevant to identify the main compounds and compound families of bioactives with immunoregulative activity. Figure 3 shows the more significant compounds with reported immunoregulative effect in the plant species and genus reviewed so far.

Examples of the predominant phytochemical groups between the reviewed plants.
Echinacea anti-inflammatory properties are attributed in general to alkamides, keto-alkenes, and caffeic acid derivatives. At the same time, polysaccharides and glycoproteins present the immune-stimulant response. 75 Due to this combination, usually, Echinacea extracts have a more intense and modulating effect in comparison to individual compounds. 75 Caffeic acid and derivatives are usually reported in different plant families, especially in the Asteraceae. Cichoric acid, a caffeic acid derivative, is reported to directly influence the immunological activity of the Echinacea genus.
Cichoric acid is found in plants such as Bidens tripartite L., Cichorium endivia L., and Cichorium intybus. L. B. tripartite is reported to have anti-inflammatory properties in paw edema models, alongside antibacterial and antifungal activities. 76 Bidens pilosa is also an Asteraceae plant that traditionally is used as an immunostimulant. B. pilosa is reported to enhance IFN-γ and cytokine production along with stimulation of white blood cell population. 9 B. Pilosa contains caffeic acid and derivatives such as caffeoylquinic acid, likely the mentioned compounds are responsible for the immune-related response. 77
Cichoric genus, as the name suggests, also contains caffeic acid derivatives, especially cichoric acid. C. intybus, common chicory, is widely used for traditional medicine in several cultures. C. intybus has anti-allergic, anti-inflammatory, and immunostimulatory activity, being this last attributed to its fructooligosaccharide and inulin content. This activity could be similar to the attributed to Echinacea polysaccharides and glycoproteins. 78 Lactuca genus, from the Asteraceae family, also contains caffeic acid derivatives. Eclipta prostrata also belongs to the Asteraceae family and is reported to contain chlorogenic acid, which also is a caffeic acid derivative. 79 Nonspecific cell immune response is elevated with the ethanolic and aqueous extract from E. prostrate. 80
The polysaccharide fraction of E. prostrata is reported to have an immunological activity and it is even considered for anticomplementary therapy. 81,82 T. officinale also belongs to the Asteraceae family; this species has been reviewed in this article. Calendula officinalis and Arnica montana belong to the Asteraceae family as well, and their preparations are used in traditional medicine as anti-inflammatory and immunomodulatory agents, although there is not enough scientific data to validate their activity. 83,84
Rosemary essential oils contain phenolic compounds such as phenolic diterpenes, flavonoids, and phenolic acids. 85 From the diterpenes, carnosol and carnosic acid are the compounds usually reported as active anti-inflammatory compounds. Rosmarinic acid biosynthesis is derived from the phenylpropanoid family, although there are not enough reports relating rosemary caffeic acid and chlorogenic acid to an immunomodulatory response, probably due to its lower total composition. 58
Plantago genus is from the Plantaginaceae family; the main compounds reported are similar to those of the Asteraceae family, reporting polysaccharides and caffeic acid derivatives. Plantago genus reports also include flavonoids, alkaloids, and iridoid glycosides. Verbascoside, a phenylethanoid glycoside, is also reported in the Plantago genus. Verbascoside is also the main active ingredient isolated from mullein (Verbascum). Phenylethanoid glycosides such as forsythoside B, leucosceptoside B, and verbascoside, and iridoid glycosides such as aucubin, ajugol harpagoside, nigroside III, and nigroside VI are reported in Verbascum genus. 73
Verbascoside is the most studied active compound isolated from Verbascum, and anti-inflammatory properties of mullein are attributed to the verbascoside. 71 Interestingly, this glycoside is chemically composed by one caffeic acid moiety, and it is found in more than 200 plants from 23 families, including the Asteraceae, Lamiaceae, and Plantaginaceae. Verbascoside biosynthesis pathway is not fully understood, although its biosynthesis starts from phenylalanine and tyrosine precursors from the shikimate pathway. 86
C. papaya also reported phenolic compounds such as caffeic acid derivatives and phenolic glycosides, although the anti-inflammatory and immunoregulatory response of C. papaya are often attributed to the content of alkaloids and flavonoids. 70 Papain from C. papaya combined with other proteolytic enzymes also show anti-inflammatory activity, although flavonoids are the principal active compounds related to such response. 87
Polysaccharides are common in plants with immunological activity, A. vera is the plant with the higher total polysaccharide composition reviewed. From this plant, polysaccharides such as acemannan and aloeride have an immunological activity. 37 The immunological response of A. vera could be enhanced due to the presence of different proteins, such as lectins. 36 Garlic is reported to have also the presence of polysaccharides and fructooligosaccharides, the activity of which could enhance the effect of organosulfur compounds, their major bioactive molecules.
Organosulfur compounds include allyl sulfides and polysulfides, often derived from alliin, which is rapidly transformed to allicin and different derivatives after the “damage” of the garlic. 88 Lectins and agglutinin-type proteins have been isolated from A. sativum with demonstrable immunological function. 89 Alliin derivatives, organosulfur compounds, can also be found in different members of the genus, such as A. cepa (onion), A. porrum (leek), and A. schoenoprasum (chives), A. iranicum, and A. elburzense. 90
PROPOSED THERAPEUTIC USAGE OF MEDICINAL PLANT-DERIVED PREPARATIONS FOR COMPLEMENTED TREATMENT AND PREVENTION OF COVID-19
It is of extreme importance to emphasize that the usage of plant-derived preparation should not be intended to substitute established medical treatments against COVID-19. It should be intended to be used as a mean to synergistically promote and module an adequate immune response, in combination with medical treatments, with the authorization and under the supervision of a qualified physician.
Extracts and compounds that enhance the immune response must be considered in the early stages of an infection or as a preventive agent. Such is the case of Echinacea genus, garlic, Plantago genus, and specific preparations of T. officinale and compounds from A. vera. Compounds and preparations, which also show an immunoregulatory response, are more suitable for a long-term regimen since its response is modulated by the immune response state, being able to control abnormal responses.
As mentioned earlier, some of the principal problems in chronic diseases are related to the constant cytokine overproduction, leading to severe tissue damage. Long-term infections in patients with chronic disorders tend to magnify the proinflammatory cytokine response. In advanced stages of the infection, it is recommended to use preparations with significant anti-inflammatory activity, such as the case of rosemary and C. papaya preparations. In long-term chronic states, the use of anti-inflammatory preparations can be indicated, especially those with modulating activity, such is the case of garlic, Verbascum, and A. vera preparations and derived compounds. This approach can be counted in the supplemental treatment and prevention of SARS-CoV-2 infection, where not only the evolution of inflammation factors should be counted but also lymphocytopenia, considering the usual clinical evolution. Figure 4 presents the timeline course of COVID-19 and prospective guideline suggesting a rational plant-based preparation usage, as co-treatment, for each stage.
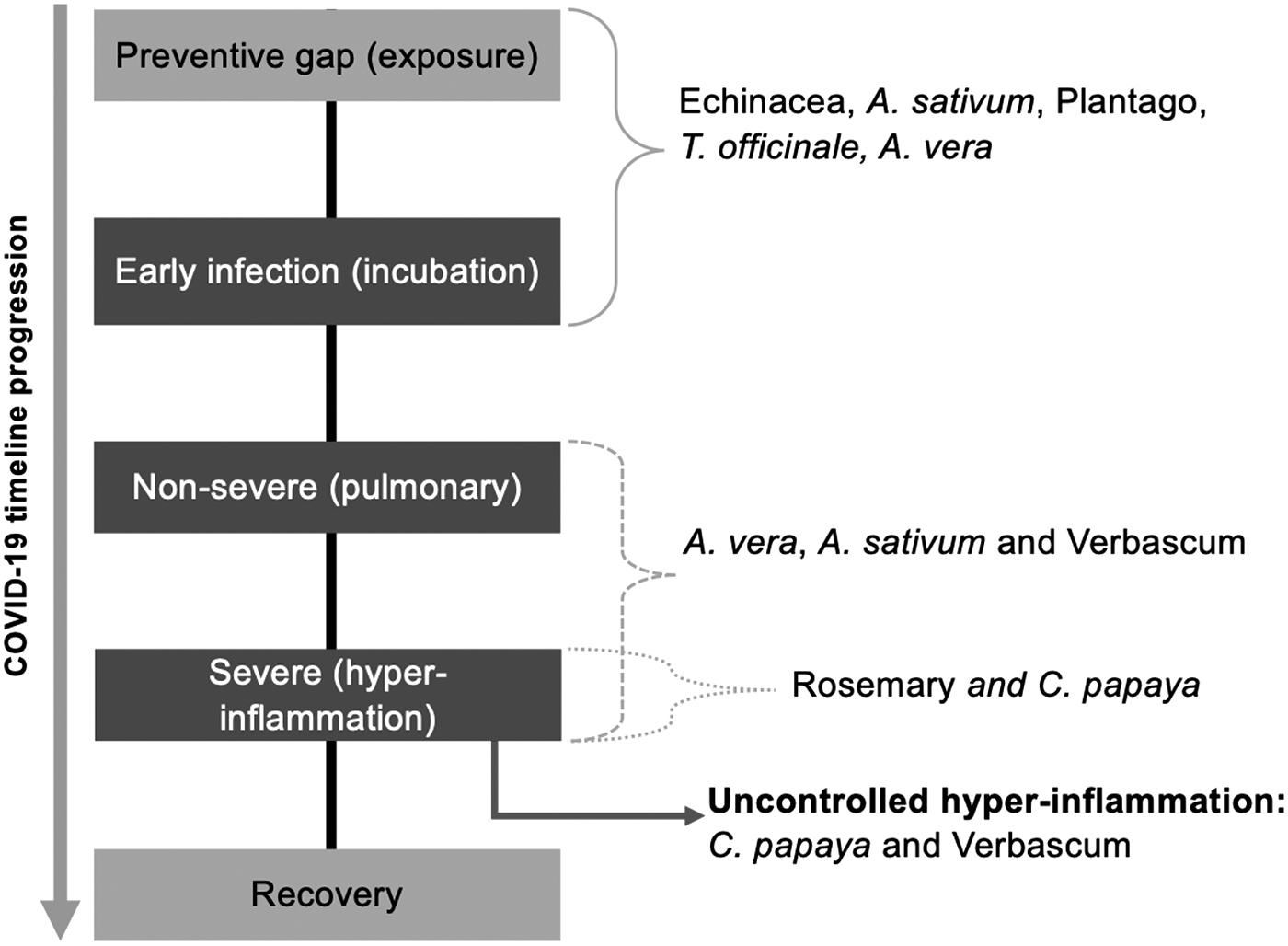
COVID-19 stages in timeline progression and prospective guideline for the rational usage of plant-derived preparations as co-treatments for each stage. Brackets indicate the proposed plant species/genus proposed for the stage in accordance to their effects (Fig. 2). Red arrow indicates the possibility of use C. papaya and Verbascum preparations in a severe and uncontrolled hyperinflammation clinical condition.
The early treatment of COVID-19 with immunoenhancing compounds/extracts of A. vera, Echinacea, Plantago, garlic, and dandelion can be beneficial to increase the immediate immune response by elevating proinflammatory cytokines (Figs. 1 and 2), which also activates and elevates migration and differentiation of several immune cells, including lymphocytes and especially Th1 and Th2 (T cells suffer a significant decrease). These compounds and extracts can also exert an anti-inflammatory effect, so their activity modulates depending on the response stage. Treatment with the plant derivatives will not contribute to an excessive inflammatory response.
However, it decreases considering their modulating response and the fact that an effectively conducted immune response promptly controls the infection, preventing the rise of severe later stages. If the infection is not efficiently restrained, the use of compound/extracts of C. papaya and Verbascum can help reduce the production of proinflammatory factors; both plant-derived preparations do not have a significant enhancing response, so they are more likely to have a more potent anti-inflammatory response. A. vera, Echinacea, Plantago, garlic, and rosemary could be also considered anti-inflammatory agents since they report a reducing effect in the production of TNF-α and IFN-γ. A. vera and Plantago particularly have both TNF-α and IFN-γ, increasing their anti-inflammatory spectrum (Figs. 2 and 4).
Although the reviewed plants and plant-derived preparations have been in used in traditional medicine for a long time without showing negative toxicological effects, it is relevant to define an adequate dose for each patient case-by-case. 65,86,91 –93 The dosage commonly depends on the weight of the subject, its current medical condition, anamnesis, and the concentration of the main bioactive component in the preparation. Thus, it is important to consider the standardization of each plant preparation to adjust the dose based not only on the weight of the patient but also on other medical conditions such as obesity and renal and hepatic function.
CONCLUSIONS
The use of plants and plant-derived preparations with immunoregulatory activity is a viable co-treatment option for different diseases, such as bacterial and viral infections and auto-inflammatory and autoimmune disorders. The reviewed plant preparations, unlike another therapeutic agents, show a response that is modulated depending on the state of the patient. Hence, undesired secondary effects can be reduced. Also, plant-derived preparations tend to be more economical and accepted for the general population, particularly those looking for “natural” treatment options. As mentioned before, the use of such plant-derived preparation should be intended to synergistically promote and module an adequate immune response, in combination with established medical treatments, including the novel vaccines. Nutrients such as vitamins C and D, and zinc are also being studied as co-treatment in several trials. These nutrients have shown similar effects as immune response enhancers. 94
A relevant area of opportunity regarding the use of plant-derived preparations as co-treatments is the lack of standardization, as the concentration of bioactives within the plant may vary significantly based on growth, harvest, and storage conditions. Furthermore, the process by which the preparation is obtained (infusion, maceration, drying, etc.) may also affect the concentration of plant bioactives. Standardization guidelines should be carefully designated to guarantee the desired therapeutic effect, preventing at the same time the appearance of adverse side effects. The final objective is to regulate their use based on scientific evidence and the assurance of its efficacy and safety, so these types of preparations could be rationally used as an adjuvant in the treatment of current COVID-19 pandemic and extrapolated to similar viral diseases.
Footnotes
AUTHORs' CONTRIBUTIONS
The article was written through contributions of all authors. All authors have given approval to the final version of the article.
ACKNOWLEDGMENTS
Authors acknowledge the national postdoctoral scholarship from the Consejo Nacional de Ciencia y Tecnología (CONACyT) to T.V.-C. and the support of Tecnológico de Monterrey, Bioprocess Research Group.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
The authors acknowledge the Consejo Nacional de Ciencia y Tecnología (CONACyT) for the national postdoctoral scholarship granted to Teresa Vargas-Cortez, as well as the support of the Molecular and Systems Bioengineering research group from Tecnologico de Monterrey.