
Abstract
There is a lack of studies on the effects of Korean ginseng (Panax ginseng C.A. Meyer) on face or body temperature. Therefore, in this study, we evaluated the effects of a black ginseng extract, KGR-BG1, on head and face temperatures and compared them with those of red ginseng extract and a placebo. We assessed their safety and tolerability and examined changes in the serum levels of biomarkers associated with immune responses, as well as with glucose and lipid metabolism. A randomized, double-blind, placebo-controlled study was conducted with 180 participants. The participants were randomly assigned to the KGR-BG1, red ginseng extract, or placebo group. Each group received a 1500 mg oral dose of their respective substances containing 1000 mg of the active component or placebo twice daily for 6 weeks. After treatment, changes in the head, face, and body temperature were measured, and serum biomarkers were evaluated. A total of 172 participants completed the evaluation after 6 weeks of treatment. No significant differences were observed in the head, face, and body temperatures among the treatment groups. After 6 weeks of treatment, the serum levels of biomarkers associated with inflammation, glucose metabolism, and lipid metabolism were similar to the baseline levels in all treatment groups. KGR-BG1 was well-tolerated compared with red ginseng extract and placebo. KGR-BG1 did not significantly alter head, face, or body temperature, or serum biomarker levels, and it was well tolerated in healthy volunteers over 6 weeks of treatment. Study Registration: Registered at Clinical Research Information Service (CRIS;
INTRODUCTION
Korean ginseng (Panax ginseng C.A. Meyer) has been used in traditional Asian medicine for more than 2000 years. 1 Ginseng is arguably the most widely used herbal product worldwide because of the growing interest in alternative medicine and natural health foods. 2,3 Ginseng affects cognitive function, the cardiovascular system, digestive function, glucose and lipid metabolism, and immune function. 2,4 –7 In addition, ginseng is commonly used as an adaptogen, meaning that it increases resistance to physical, chemical, and biological stress, enhances many physical processes, and promotes general vitality. 2
Ginseng is consumed as white ginseng, red ginseng, and black ginseng, which are differentiated during the manufacturing process. White ginseng is produced by dehydrating fresh ginseng using sunlight, 8,9 and red ginseng is made by steaming fresh ginseng at 95–100°C for 2–3 h and then drying it at 55–60°C. 8,10 Black ginseng is produced by subjecting white ginseng to nine cycles of steaming at 95–100°C for 3 h. 8
Ginsenosides, the main active components of ginseng, have important pharmacological properties, including antidiabetic, anti-inflammatory, and antitumor activities. 8,11 –13 Studies have shown that the steaming process increases the pharmacological and biological activities of ginseng. 9,14 Specifically, black ginseng exhibits more potent pharmacological activity than white or red ginseng. 15,16 In addition, some newly identified ginsenosides, such as Rg3, Rg5, F4, Rg6, Rk3, Rs3, and Rs4, which are absent in white ginseng, are found in black ginseng. 14 KGR-BG1, an extract of Korean black ginseng that contains higher levels of Rg5, Rk1, and Rg3 than other ginseng preparations, was developed by Korean Ginseng Research Co., Ltd. (Gyeonggi-do, Korea). 17
However, there are concerns regarding the potential of Korean ginseng to increase body temperature. 18,19 In contrast, studies show that American ginseng (Panax quinquefolius L.) has a cooling effect. 20,21 However, there is a lack of evidence regarding the effects of ginseng or its components on body temperature. For instance, a previous animal study showed that neither white nor red ginseng has a significant effect on body temperature. 18 In contrast, pretreatment with ginsenoside Rb1 enhances thermogenesis and improves cold tolerance in rats. 22 Therefore, a thorough evaluation of the effects of ginseng on body temperature in humans is necessary to provide safety guidelines for the use of Korean ginseng.
This study aimed to investigate the effects of KGR-BG1 on head, face, and body temperatures compared with red ginseng extract and a placebo. We also examined the changes in the serum levels of biomarkers associated with immune responses, as well as with glucose and lipid metabolism. Furthermore, we evaluated the safety and tolerability profiles of KGR-BG1 and compared them with those of the red ginseng extract and placebo.
MATERIALS AND METHODS
Study population
Healthy volunteers aged 20–64 years who presented no abnormalities in their medical history, physical examination, or clinical laboratory tests were considered eligible to participate in the study. The study's purpose, benefits, risks, and procedures were fully explained to all participants before obtaining written informed consent.
The study protocol and informed consent forms were approved by the Institutional Review Board of Kyung Hee University Hospital, Seoul, Korea (approval No. KHUH 2017-03-081). All procedures were conducted according to the Declaration of Helsinki and Korean Good Clinical Practice (Clinical Research Information Service [CRIS;
Preparation of the treatments
KGR-BG1 and red ginseng extract were manufactured from Korean ginseng (P. ginseng C.A. Meyer) and obtained from the Korean Ginseng Research Co., Ltd. KGR-BG1 was prepared by extracting and concentrating fresh 6-year-old Korean black ginseng, which involved five cycles of steaming and drying. The KGR-BG1 contained 13.43 mg/g of ginsenosides: Rg3, Rg5, and Rk1. The red ginseng extract was prepared by extracting and concentrating Korean red ginseng, which was purchased from Punggi Ginseng Cooperative Association (Yeongju, Korea). The red ginseng extract contained 28.98 mg/g of ginsenosides: Rb1, Rg1, and Rg3. The placebo was composed of maltodextrin in 500 mg capsules identical in appearance to the ginseng products.
Study design
A randomized, double-blind, placebo-controlled study was conducted with 180 participants. Volunteers were randomly assigned to three different treatment groups: KGR-BG1, red ginseng extract, and the placebo. After baseline assessments (including measuring each person's head, face, and body temperature), they were each administered 1500 mg (3 capsules × 500 mg), of which 66.6% was active component (KGR-BG1 or red ginseng extract). Therefore, each participant was administered 1000 mg of the active component or placebo twice daily for 6 weeks. Two weeks after beginning the administration, investigators asked about any adverse effects (AEs) and verified patient compliance over the phone. Six weeks after beginning administration, changes from the baseline (values at week 6 minus baseline values) in head, face, and body temperature, safety, tolerability profiles, and serum levels of biomarkers were evaluated.
The required sample size was calculated according to the methods described in a previous study, 23 where temperatures were measured at 11 acupuncture points in participants who were administered red ginseng, white ginseng, or a placebo. Based on the results of that study, the effect size was calculated using the one-way fixed-effects analysis of variance (ANOVA) test. 24 Based on the calculated effect size of 0.248, the number of participants required in our study was 54 per treatment group, at a significance level of 0.05, and power of 80%. Assuming a drop-out rate of 10%, a total of 180 participants per group was considered appropriate.
Measurement of temperature
Temperatures on the head (at the vertex) and face were measured using a skin thermometer (ST500; Courage and Khazaka Electronic GmbH, Cologne, Germany) in a humidity chamber maintained at a constant temperature at the Kyung Hee Medical Science Research Institute Clinical Trials Center (Seoul, Korea). The temperature and humidity of the chamber were maintained at 20–25°C and 40–60%. The temperature was measured at the following five acupuncture points on the face: between the inner edges of the eyebrows (Indang), between the upper lip and base of the nose (Sugu), at the midline of the chin (Seungjang), and the left and right sides below the lower border of the zygomatic bone (Quanliao). In addition, the tympanic temperatures of the left and right ears were measured to evaluate the core body temperature.
Exploration of changes in serum levels of biomarkers
We evaluated changes in the levels of biomarkers associated with glucose metabolism (insulin, glucose, hemoglobin A1c [HbA1c]), and with the homeostatic model assessment of insulin resistance [HOMA-IR]) and lipid metabolism (total cholesterol, triglyceride, high-density lipoprotein [HDL]). We also measured the changes in low-density lipoprotein (LDL) levels. Furthermore, the concentrations of high-sensitivity C-reactive protein (hs-CRP) and interleukin 6 (IL-6) in the serum were measured to assess the effects of the different substances on immune responses. For the IL-6 assay, an enzyme-linked immunosorbent assay was performed in duplicate using a commercial kit (BMS213HS; Bender MedSystems GmbH, Vienna, Austria) according to the manufacturer's instructions. The intra- and interassay coefficients of variation were 4.9% and 6.0%, respectively, with a 0.03 pg/mL lower limit of detection. To determine the concentration of IL-6, absorbance was measured at 450 nm using a Tecan Spark 10M multimode microplate reader (Tecan Group Ltd., Männedorf, Switzerland).
Safety and tolerability assessment
The occurrence of AEs was monitored throughout the entire study period. AEs were assessed by an investigator in terms of severity (mild, moderate, severe) and their relationship with the treatment. In addition, changes from the baseline in vital signs, results of physical examinations, and results of clinical laboratory tests, including hematology, blood chemistry, and urinalysis, were evaluated to assess the safety and tolerability of the treatments over 6 weeks.
Statistical analyses
The continuous variables were summarized using descriptive statistics. The demographic characteristics of each treatment group were compared using the chi-square test or Kruskal-Wallis test. Changes in head, face, and body temperatures between the treatment groups were compared using ANOVAs, which were also conducted to determine the significance of the differences in biomarker levels in each treatment group. In addition, a paired t-test was performed to determine the differences in temperature and serum biomarker levels before and after 6 weeks of treatment. The lower limit of detection values for hs-CRP (0.01 mg/L) and IL-6 (0.03 pg/mL) were used for statistical analyses in cases where the concentrations were below the detection limits.
The number of participants who reported AEs at least once was compared between the treatment groups using the chi-square test. P < .05 was considered statistically significant. Statistical analyses were performed using SPSS (version 22.0; IBM SPSS, Inc., Chicago, IL, USA) and R version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Demographic characteristics
Of the 180 participants, 177 who were administered either ginseng at least once were included in the safety and tolerability assessment. To analyze changes in head, face, and body temperature, a total of 172 participants who completed the evaluation after 6 weeks of treatments were included. These 172 participants were also included for measurement of the serum levels of biomarkers, except for IL-6 levels. For measuring serum IL-6 levels, a total of 166 participants were included because of missing values: 58 in the KGR-BG1 group, 55 in the red ginseng extract group, and 53 in the placebo group.
Various demographic characteristics in each treatment group, such as sex, age, weight, and height, were included in the analysis, but they were not significantly different (P > .05) (Table 1).
Demographic Characteristics of the Participants in Each Group Who Completed the Evaluation After 6 Weeks of Treatment
chi-square test.
Kruskal-Wallis test.
Evaluation of head, face, and body temperature
No significant changes were found in the head or face temperatures between the treatment groups after 6 weeks of treatment (Table 2). Moreover, individual changes in head or face temperatures were balanced at approximately zero in all treatment groups (Fig. 1). Furthermore, there were no significant changes in head or face temperatures after treatment with either KGR-BG1 or red ginseng extract. However, there were statistically significant changes in the temperature at two acupuncture points in the placebo group (P = .017 for Sugu and P < .001 for Seungjang, paired t-test) (Fig. 2). In addition, similar mean core body temperatures were maintained before and after treatment regardless of the treatment group (Table 2).
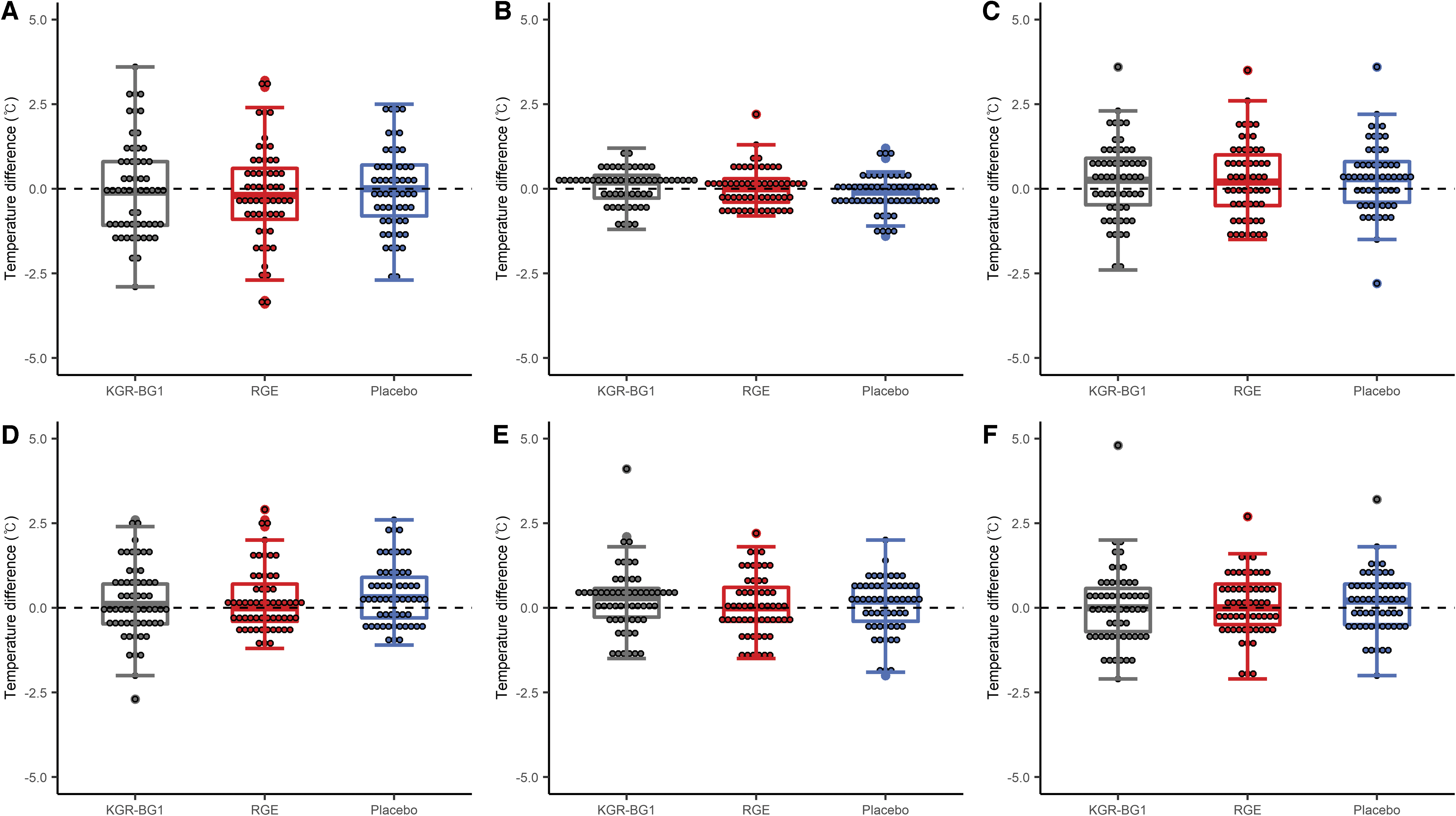
Distribution of changes in temperature of the
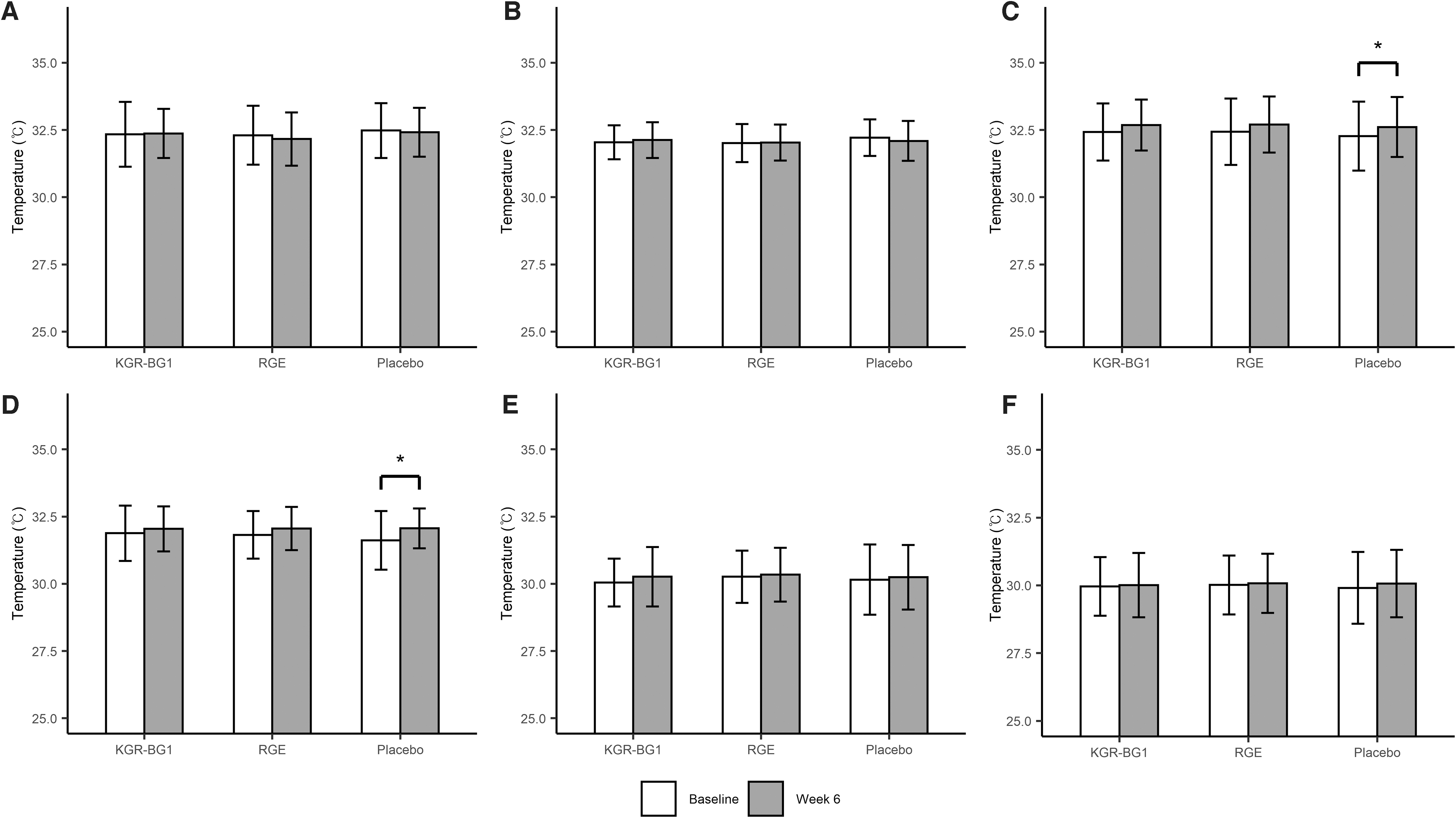
Temperature of the
Changes in Head, Face, and Body Temperature in Each Group Before and After 6 Weeks of Treatment
Data are presented as the arithmetic means ± standard deviations.
ANOVA for the changes between the treatment groups.
ANOVA, analysis of variance.
Serum levels of biomarkers
After 6 weeks of treatment, the serum levels of all biomarkers associated with inflammation (hs-CRP and IL-6), glycemic control (insulin, glucose, HOMA-IR, and HbA1c), and lipid metabolism (total cholesterol, triglyceride, HDL, and LDL) were similar to those at baseline. No statistically significant changes were found in serum levels of biomarkers before and after 6 weeks of treatment, except for insulin and HOMA-IR in the placebo group (P = .011 for insulin and P = .012 for HOMA-IR, paired t-test). Furthermore, the change was not significantly different between the treatment groups (P > .05, Table 3).
Changes in Biomarkers Associated with the Immune Response, as Well as Lipid and Glucose Metabolism, in Each Group Before and After 6 Weeks of Treatment
The data are presented as the arithmetic means ± standard deviations.
The ANOVA test was used to analyze changes between the treatment groups.
For IL-6, the number of participants was 58, 55, and 53 for KGR-BG1, red ginseng extract, and placebo, respectively, owing to missing values.
HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HOMA-IR, homeostatic model assessment of insulin resistance; hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin 6; LDL, low-density lipoprotein.
The mean changes from the baseline levels in hs-CRP were 0.05, 0.02, and 0.09 mg/L, and IL-6 were −0.06, −0.11, and −0.02 pg/mL, for KGR-BG1, red ginseng extract, and the placebo, respectively. Overall, KGR-BG1, red ginseng extract, and the placebo did not significantly change the serum levels of biomarkers associated with immune response, glucose metabolism, or lipid metabolism in healthy participants after 6 weeks of treatment.
Safety profiles and tolerability
Seventy-five of the 177 participants experienced at least 1 AE during the entire study period. Among those, 23 participants reported treatment-related AEs: 8 from the KGR-BG1 group, 9 from the red ginseng extract group, and 6 from the placebo group. There was no statistically significant difference in the number of participants that reported at least one study product-related AE between the treatment groups (P = .705, Chi-square). No serious AEs were reported during the study period. The most frequent treatment-related AEs were dyspepsia (seven cases in six participants), followed by feeling hot (five cases in five participants) and epigastric discomfort (four cases in four participants) (Table 4). Regardless of the treatment group, no significant changes were found in safety or tolerability parameters, including vital signs, physical examination, or clinical laboratory tests.
List of Treatment-Related Adverse Events in Each Treatment Group
Data are presented as the number of participants (%).
DISCUSSION
There were no significant changes in head, face, or body temperature before and after 6 weeks of treatment in the KGR-BG1, red ginseng extract, or placebo groups. In addition, individual head and face temperatures did not show specific trends of change. The extent of the changes in head, face, and body temperature was similar between all treatment groups. Therefore, neither treatment with KGR-BG1 nor red ginseng extract increased head, face, or body temperature in healthy participants.
Korean ginseng may act as a modulator that maintains homeostasis in living organisms 25 and it is beneficial for developing cold tolerance in low-temperature environments. 22,26 However, previous reports have shown that Korean ginseng does not increase body temperature, especially not under low- or high-temperature conditions. For instance, no significant change in core body temperature was found in mice after administration of either white or red Korean ginseng, and energy expenditure in mice treated with ginseng extract was not different from that in mice treated with phosphate-buffered saline. 18 Moreover, simultaneous treatment with heat and Korean ginseng increased body temperature, whereas administration of Korean ginseng without heat treatment did not significantly increase body temperature in rats. 27
Our study also showed that 6 weeks of treatment with KGR-BG1 or red ginseng extract did not significantly increase head, face, or body temperature compared with a placebo. Overall, Korean ginseng extract did not increase head, face, or body temperatures at room temperature (20–25°C).
We did not observe any significant changes in the serum levels of biomarkers associated with lipid metabolism after 6 weeks of treatment with KGR-BG1 or red ginseng extract. Mechanistic and clinical evidence shows that ginsenosides exert antiobesity effects by modulating the expression of genes associated with lipid metabolism. Specifically, Korean red ginseng extract suppresses the expression of fatty acid synthase and 3-hydroxy-3-methylglutaryl coenzyme A reductase and therefore decreases hepatic lipid accumulation. 28 Moreover, ginsenoside Rg3, a major component of both red ginseng extract and KGR-BG1, inhibits 3-hydroxy-3-methylglutaryl coenzyme A reductase expression by activating 5′-adenosine monophosphate-activated protein kinase in HepG2 cells. 29
Furthermore, serum concentrations of total cholesterol, LDL, and triglycerides decrease, whereas HDL increases after administration of 2 g Korean ginseng extract three times daily for 8 weeks. 7 In contrast, administration of 500 mg Korean ginseng extract twice daily for 8 weeks did not have a significant effect on lipid profiles in patients with hyperlipidemia. 30 Considering this, administration of 1500 mg of ginseng extract (1000 mg of the active component) twice daily for 6 weeks in this study, which was determined based on an animal study, 17 may not have been enough to induce significant changes in the patients' lipid profile. Further studies with various dosage regimens and treatment periods would be helpful to elucidate the effects of KGR-BG1 and red ginseng extract on lipid metabolism.
Studies have shown that ginseng and its components have beneficial effects on glycemic control. For instance, a meta-analysis of 16 randomized controlled trials showed that ginseng supplementation significantly lowers fasting blood glucose levels. 31 In addition, ginsenoside Rb1, a component of both KGR-BG1 and red ginseng extract, significantly decreases fasting blood glucose levels and improves glucose tolerance in high-fat diet-induced rats with obesity. 32 However, there is conflicting evidence regarding the effects of ginseng on some glycemic indices, especially HbA1c. Specifically, Korean red ginseng did not affect HbA1c levels after 12 weeks of supplementation in patients with well-controlled type 2 diabetes. 33
In our study, no significant changes in glycemic indices, including glucose, insulin, HOMA-IR, and HbA1c levels, were observed in either the KGR-BG1 or red ginseng extract groups. This absence of effect on glucose metabolism of KGR-BG1 and red ginseng extract may be due to the relatively short duration of the trial and the use of healthy volunteers.
Further studies have shown that ginseng and its components regulate immune responses by modulating cytokine secretion. 34 For example, ginsenoside Rb1 suppresses both the gene and protein expression of IL-6 in rats with cerebral ischemia. 35 In contrast, administration of 1.5 g of Korean red ginseng three times daily for 12 weeks does not significantly affect inflammatory markers, including hs-CRP, in participants with metabolic syndrome. 36 Ginseng has been known to act as an immune modulator that maintains homeostasis and enhances resistance to illness. 34 In this regard, the lack of significant changes in inflammatory cytokine levels after ginseng extract administration can be possibly explained by the study participants, which consisted of healthy volunteers. Further long-term studies in various patient groups would be beneficial to show the effects of Korean ginseng extracts on the immune response and glucose and lipid metabolism using biomarkers.
In the safety and tolerability assessment, no statistically significant differences were found in the number of participants who reported at least one treatment-related AE in each group. Previous clinical trials suggest that Korean ginseng is well tolerated by most users, with headache, gastrointestinal, and sleep disorders being the most commonly experienced AEs. 37 All treatment-related AEs were mild and no significant changes were observed in the safety and tolerability parameters in our study. The most frequently reported treatment-related AEs were gastrointestinal disorders, such as dyspepsia and epigastric discomfort, and feeling hot. Although these were previously reported AEs associated with ginseng preparations, 37 the general trend of AE occurrences was similar in all treatment groups.
Thus, we concluded that both KGR-BG1 and red ginseng extract were well tolerated in healthy participants for 6 weeks of administration. Further studies in a larger patient group with a longer period of treatment and controlling for the effects of hormones on body temperatures may be helpful to clarify the results of this study.
DISCUSSION
In conclusion, our study showed that KGR-BG1 did not induce a significant increase in head, face, or body temperature in healthy volunteers over 6 weeks of treatment compared with red ginseng extract and a placebo. There were no significant changes in the serum levels of biomarkers associated with the immune response, glucose metabolism, or lipid metabolism. Furthermore, KGR-BG1, similar to red ginseng extract and the placebo, was well tolerated in healthy volunteers for 6 weeks of treatment. Further long-term studies using various dosage regimens would be beneficial to confirm our results.
Footnotes
ACKNOWLEDGMENTS
The authors thank the clinical research team of the Kyung Hee Medical Science Research Institute Clinical Trials Center for supporting our research.
AUTHORs' CONTRIBUTIONS
S.-I.P., B.-H.K., and S.-V.Y. designed the present study; S.-I.P., H.-Y.L., S.-V.Y., and B.-H.K. conducted the research. S.-I.P., S.L., and B.-H.K. analyzed the data. All authors revised the article and approved its final version.
AUTHOR DISCLOSURE STATEMENT
The authors have no conflicts of interest related to this work.
FUNDING INFORMATION
This study was supported by the Ministry of Agriculture, Food, and Rural Affairs, Republic of Korea (grant No. 316014-03-3-HD050).