
Abstract
Although lactose-free dairy products for the clinical management of lactose intolerance (LI) are widely available, scientific evidence on their efficacy is still lacking. This study comparatively analyzed the efficacy of flavored lactose-free milk (LFM) and whole milk (WM) in reducing symptoms in South Korean adults with LI. This prospective study was conducted in adults suspected of LI. All screened participants underwent the hydrogen breath test (HBT) using 570 mL of chocolate-flavored WM (20 g of lactose) and responded to a symptom questionnaire. LI was confirmed when the ΔH2 peak exceeded 16 ppm above baseline values and with the occurrence of symptoms after WM consumption. The participants who were diagnosed with LI underwent the HBT again with 570 mL of chocolate-flavored LFM (0 g of lactose), followed by the symptom questionnaire survey after 1 week. After excluding 40 participants who did not meet the diagnostic criteria for LI and 2 who were lost to follow-up, a total of 28 lactose-intolerant individuals were enrolled in the study. The ΔH2 values in the first HBT were significantly higher than those in the second HBT (33.3 ± 21.6 ppm vs. 8.6 ± 6.3 ppm, P < .001). Similarly, there was a significant reduction in the total symptom score in the second HBT (4.18 ± 1.51 vs. 0.61 ± 0.98, P < .001). Flavored LFM is well tolerated in South Korean adults diagnosed with LI based on the HBT and symptom questionnaire results. Therefore, LFM may be a viable alternative to WM.
INTRODUCTION
Milk is a significant component of the daily diets of many people given its high nutritive value. Lactose, the main sugar in milk products, is a disaccharide consisting of galactose bound to glucose by a β-galactosidic linkage. 1 Intestinal absorption of this disaccharide requires hydrolysis to free the glucose and galactose through a reaction catalyzed by lactase at the brush border of the small intestine. Although high concentrations of lactase are present in newborns, ∼75% of the world's population experiences a sharp decline in intestinal lactase synthesis after weaning and are unable to properly digest lactose. 2 This results in unabsorbed lactose reaching the colon and being fermented by the gut microbiota, yielding various products including short-chain fatty acids and gases such as hydrogen, carbon dioxide, and methane. These byproducts and unfermented lactose cause symptoms of diarrhea, abdominal pain, bloating, and flatulence.
Lactose malabsorption (LM) refers to the failure of the gut to properly digest and/or absorb lactose because of reduced expression/activity of lactase in the small intestine. Lactose intolerance (LI) refers to the occurrence of symptoms such as abdominal pain, diarrhea, bloating, or flatulence in patients with LM after ingestion of lactose. Owing to some genetic polymorphisms associated with lactase expression, the prevalence rates of LM and LI are strongly related to ethnicity. The lactase nonpersistence phenotype is found in 2–20% of the northern European population, 40% of the Mediterranean population, 65–75% of the African population, and in >90% of the Asian population, including South Korea. 3 –5 However, few individuals with lactase nonpersistence show LI-related symptoms. 6 Although a recent meta-analysis estimated the global prevalence of LM at 68%, the prevalence of LI is unknown because of the lack of a consensus for the criterion for diagnosis. 7,8 Because many individuals with LM have no symptoms after ingestion of a standard serving of dairy products, it does not attract clinical attention in most cases.
However, LI and its related gastrointestinal symptoms are common health concerns. Considering the long-term effects of lactose avoidance, LM and LI are likely to have a relevant impact on nutrition. Dairy products are easily available and excellent sources of calcium and vitamin D. Some studies have demonstrated an association between dairy product consumption and height, body mass index (BMI), and vitamin D levels in lactose-intolerant patients. 9 –11 Although numerous studies have shown conflicting results on the impact of dairy consumption on the risk of osteoporosis and fracture, lactose avoidance may predispose individuals to deficient bone acquisition, loss of bone mineral density, and other adverse outcomes. 12,13 In addition to the nutritional aspect, LI also mimics other functional gastrointestinal disorders (FGIDs) in terms of clinical manifestations. 14 A recent meta-analysis showed that LI, but not LM is more frequent among patients with irritable bowel syndrome (IBS) than among healthy controls. 15
Therefore, clinicians should be aware of the clinical implications of LI and provide systematic and rational management plans based on scientific evidence. Because the traditional strategy to manage LI is to restrict the consumption of dairy foods containing lactose, such a diet usually does not contain the recommended daily intake levels of calcium and other nutrients. 16 Therefore, commercial products have been developed for LI persons, including lactose-reduced or lactose-free milk (LFM) and lactase supplements. Probiotics and colonic adaptation by prebiotics also can be applied, but these strategies lack sufficient evidence of efficacy. 8 LFM may be one of the most reliable methods for managing LI from the standpoints of nutrition and convenience. However, previous studies have reported inconsistent results regarding the efficacy of LFM in patients with LI; moreover, there are very few studies in Asian populations on this topic.
Flavored milk is milk to which sugar and other flavorings have been added to increase the palatability, especially for children. Despite concerns surrounding added sugars, it has the potential to increase milk consumption resulting in sufficient micronutrient intake, especially of calcium. 17,18 Almost all studies investigating the implications of flavored milk have been conducted in children who are usually lactose tolerant. 18 The applicability of flavored LFM in adults with LI has never been studied. In addition, the effect of added sugar in flavored milk on LI-related symptoms has also not been sufficiently explored. Therefore, this study investigated the applicability of flavored LFM over whole milk (WM) to South Korean adults with LI.
MATERIALS AND METHODS
Study population
This prospective study was performed in a tertiary hospital in South Korea between October 2019 and July 2020. South Korean adults suspected of LI based on the self-assessment of symptoms, such as bloating, pain, or diarrhea, after usual consumption of dairy products were enrolled consecutively during the study period. The exclusion criteria were as follows: (1) previous gastrointestinal surgery; (2) history of FGIDs diagnosed by a clinician such as IBS; (3) history of inflammatory bowel disease; (4) prior use of antibiotics, probiotics, laxatives, or drugs affecting gastrointestinal motility within 4 weeks; and (5) presence of gastrointestinal symptoms. This study was performed in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Kyung Hee University Hospital (KMC IRB 2019-08-042).
Study protocol and outcome measurements
Initially, all the screened participants underwent the hydrogen breath test (HBT) using 570 mL of chocolate-flavored WM containing ∼20 g of lactose (WM-HBT) and responded to the symptom questionnaire after the test. LI was confirmed when the ΔH2 peak exceeded 16 ppm above baseline values and symptoms developed after milk consumption. The HBT result was considered abnormal if the hydrogen levels exceed the basal value by 16 ppm. Hence, the participants with a baseline hydrogen value of >20 ppm were excluded. 19 The participants who were diagnosed with LI based on the first HBT and symptom questionnaire survey underwent a second HBT and survey with 570 mL flavored LFM after 1 week (LFM-HBT).
The HBT was performed after an overnight fast, and measurements were taken 10 min before and 20, 40, 60, 80, 100, and 120 min after lactose ingestion. The participants were instructed to avoid dairy intake, smoking, and chewing gum in the previous 24 h. 19 The concentration of hydrogen in the breath samples was analyzed by gas chromatography (Quintron Instruments, Milwaukee, USA). The chocolate-flavored LFM (Easily Digested Milk Chocolate; Maeil Dairies Co. Ltd., Pyeongtaek, South Korea) used in this study was hydrolyzed by adding lactase, resulting in the absence of measurable residual lactose. The milk used in the study contained carbohydrates (21 g), sugar (16 g), protein (5 g), total fat (7.8 g), cholesterol (20 mg), sodium (75 mg), and calcium (150 mg per pack; 190 mL). The WM had a similar concentration as the LFM, except that it contained 6.5 g of lactose per 1 pack (Supplementary Table S1). All the milk samples, both WM and LFM, used in this study were packaged without any label on the outside for blinding of the participants.
All participants completed the questionnaire on gastrointestinal symptoms during the 24-h period after each test. The questionnaire items were selected from among those most frequently reported ones by LI patients: diarrhea, abdominal pain, flatulence, and bloating. The severity of symptoms experienced after lactose ingestion was self-rated by the participants using the following categories: 0 denoting none, 1, mild, and 2, severe symptom. The total symptom score of the questionnaire was obtained by summing the individual scores of the four items. Thus, the total score ranged from 0 to 8. Only the participants with a total symptom score of 2 or more in the first HBT were invited for the second round of tests.
The primary outcomes were the improvement in ΔH2 and symptom scores at the LFM-HBT. In addition, we analyzed the variables according to age (20–29, 30–39, and ≥40 years), sex, and BMI (<23 and ≥23 kg/m2).
Statistical analysis
The data were analyzed by repeated-measures analysis of variance. Because the distribution of the data was skewed, a nonparametric test was used to analyze the results. Continuous variables were expressed as mean ± standard deviation, and categorical variables, as percentages. Continuous variables were compared using t-test or two-factor analysis of variance for parametric data and the Mann–Whitney rank rum test or Kruskal–Wallis H-test for nonparametric data. Categorical data were compared using the chi-square or Fisher's exact test. Statistical analyses were performed using the R software (ver. 3.5.3; R Foundation for Statistical Computing, Vienna, Austria). A value of P < .05 was considered significant.
RESULTS
In all, 70 participants who experienced dairy consumption-related gastrointestinal symptoms were invited to participate in this study. After excluding 40 who did not meet the diagnostic criteria for LI based on the WM-HBT and symptom questionnaire results, 30 participants were included. Among them, two were lost to follow-up after the first HBT, resulting in a final sample of 28 participants (17 men and 11 women) (Fig. 1). The mean age of the participants was 39.4 ± 12.3 (24–65) years and mean BMI was 22.5 ± 2.6 kg/m2. The ΔH2 values for the WM-HBT and LFM-HBT are given in Figure 2. The mean ΔH2 value for WM was significantly higher than that for LFM (33.3 ± 21.6 vs. 8.6 ± 6.3 ppm, P < .001). Likewise, the total symptom scores at the WM-HBT were significantly higher than those at the LFM-HBT (4.18 ± 1.51 and 0.61 ± 0.98, respectively; P < .001; Fig. 3). The differences in the symptom scores between WM and LFM are given in Figure 4.
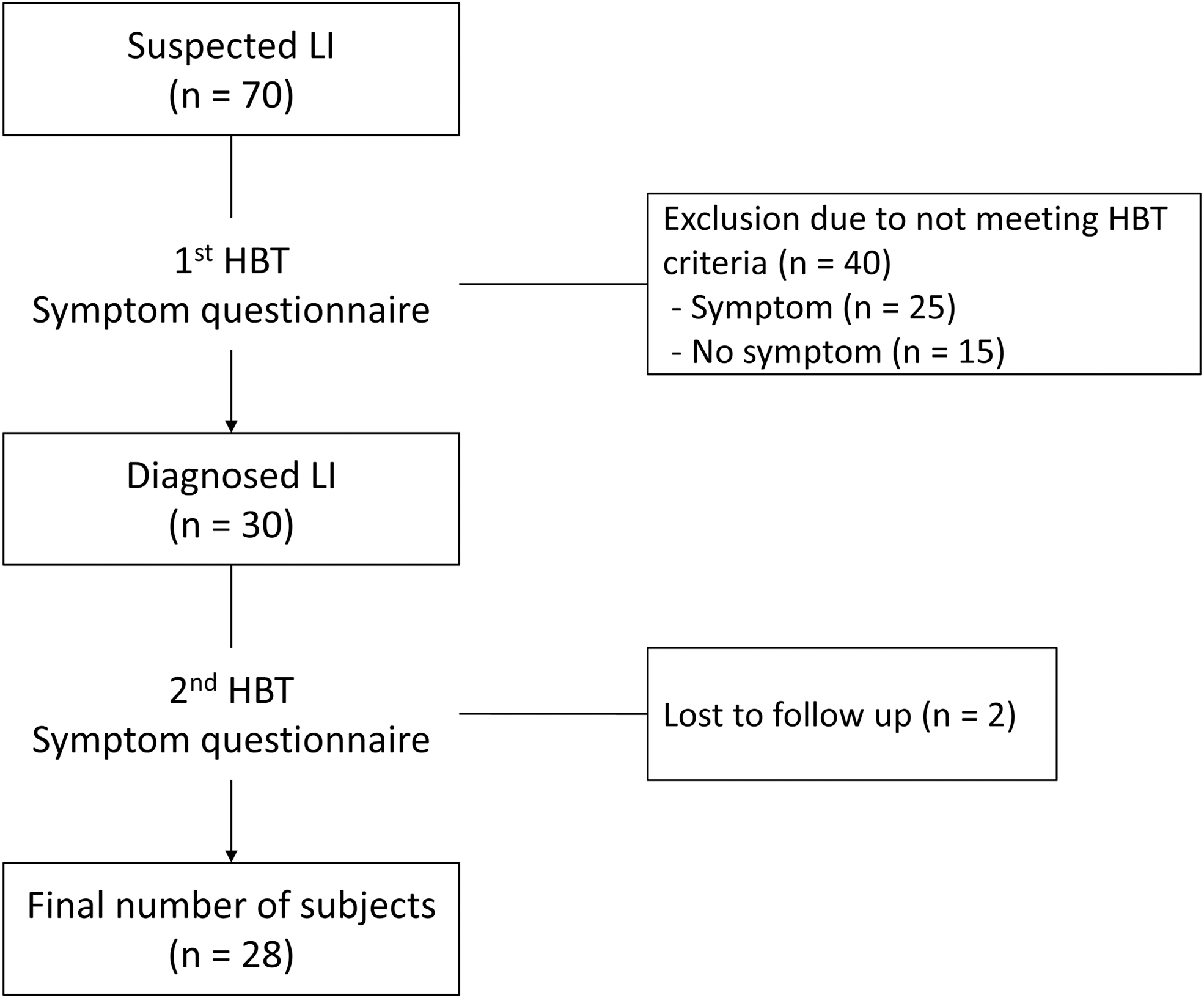
Flow diagram illustrating participant enrollment. HBT, hydrogen breath test; LI, lactose intolerance.
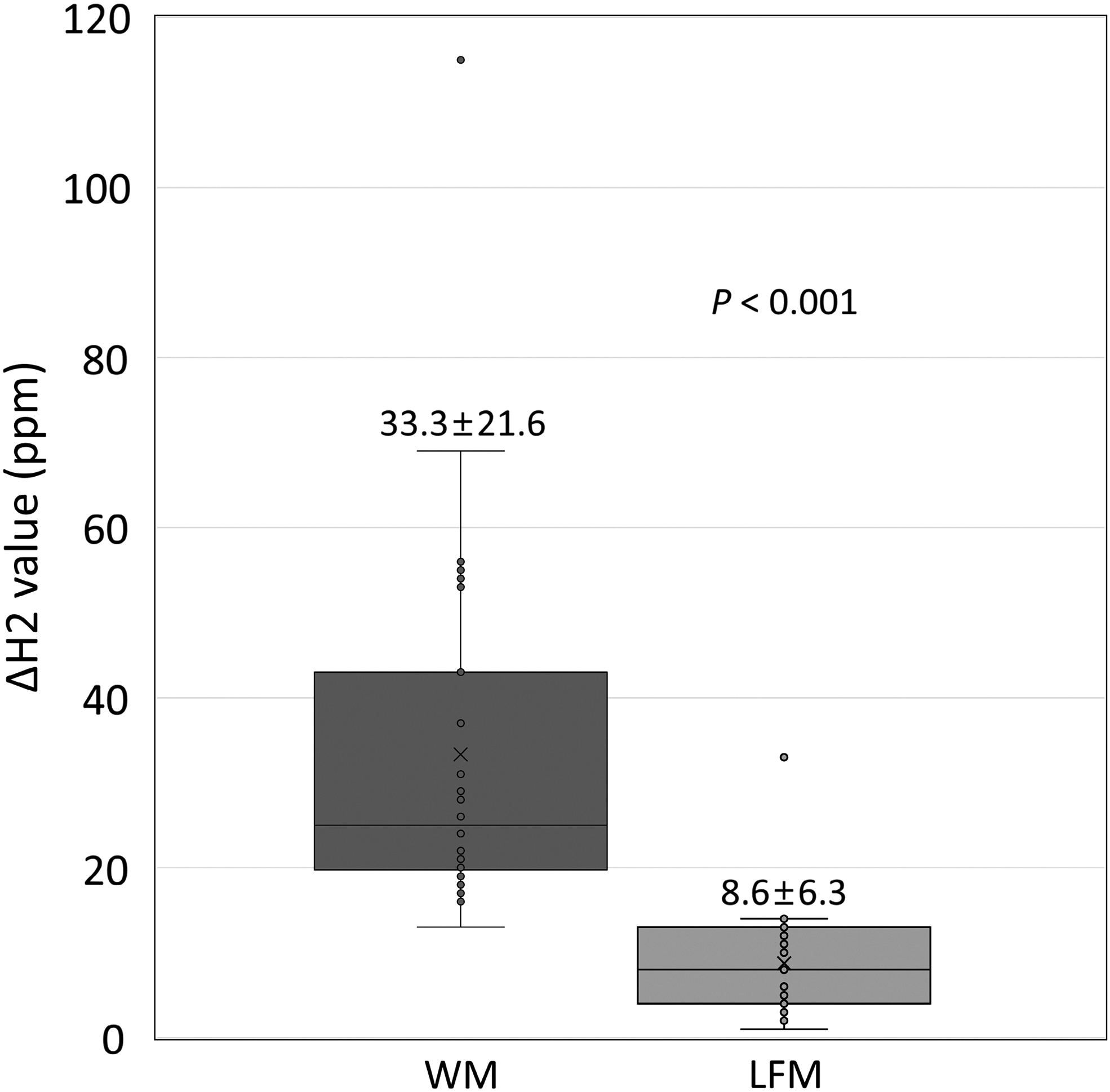
The ΔH2 value of HBT with WM and flavored LFM. Data are presented as mean ± SD. Comparison between groups was analyzed using t-test. LFM, lactose-free milk; SD, standard deviation; WM, whole milk.
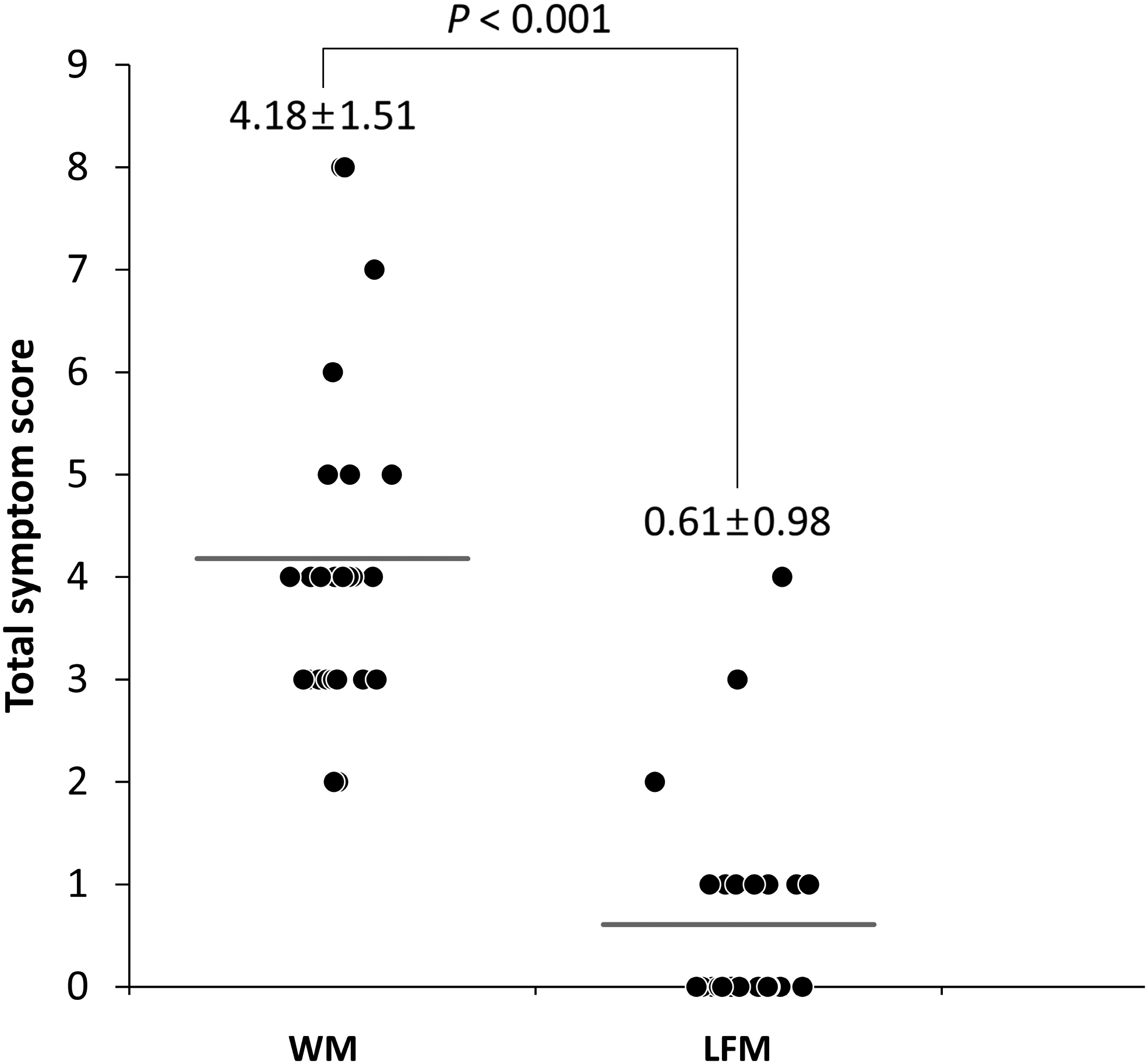
The differences in total symptom score between tests with WM and flavored LFM. Data are presented as mean ± SD. Comparison between groups was analyzed with Mann–Whitney U-test.
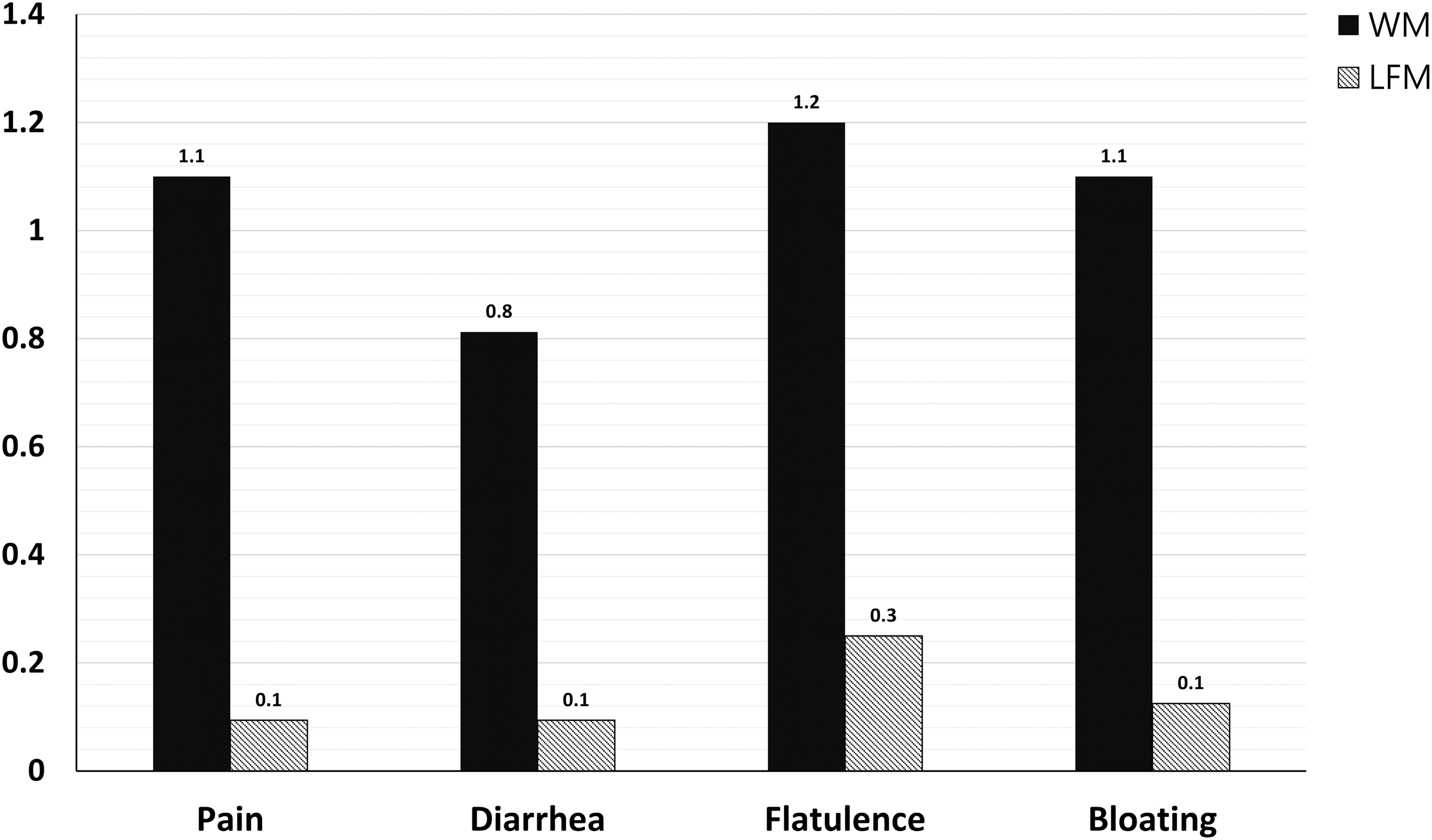
The differences in each symptom score between tests with WM and flavored LFM. Data are presented as mean ± SD. Comparisons between groups were analyzed with Mann–Whitney U-test. There were statistically significant differences between the two groups in all symptom items.
Next, we analyzed the differences in ΔH2 values and total symptom scores between WM-HBT and LFM-HBT according to subgroups of age, that is, 20–29 (n = 9), 30–39 (n = 10), and ≥40 (n = 9) years, sex, that is, male (n = 17) and female (n = 11), and BMI, that is, <23 kg/m2 (n = 10) and ≥23 kg/m2 (n = 18). Regardless of age, sex, and BMI, the ΔH2 values and symptom scores were significantly lower in the LFM-HBT than at the WM-HBT (Fig. 5). However, the mean ΔH2 value at the WM-HBT were significantly higher in the women than in men (46.1 ± 29.8 vs. 25.1 ± 8.8 ppm, P = .044) (Fig. 5C). Furthermore, the mean total symptom score at the LFM-HBT was also significantly higher in women than in men (1.2 ± 1.3 vs. 0.2 ± 0.4, P = .042) (Fig. 5D). Regarding BMI, the mean symptom score at the LFM-HBT was significantly higher in the <23 kg/m2 group than in the ≥23 kg/m2 group (1.3 ± 1.3 vs. 0.2 ± 0.4, P = .033) (Fig. 5F).
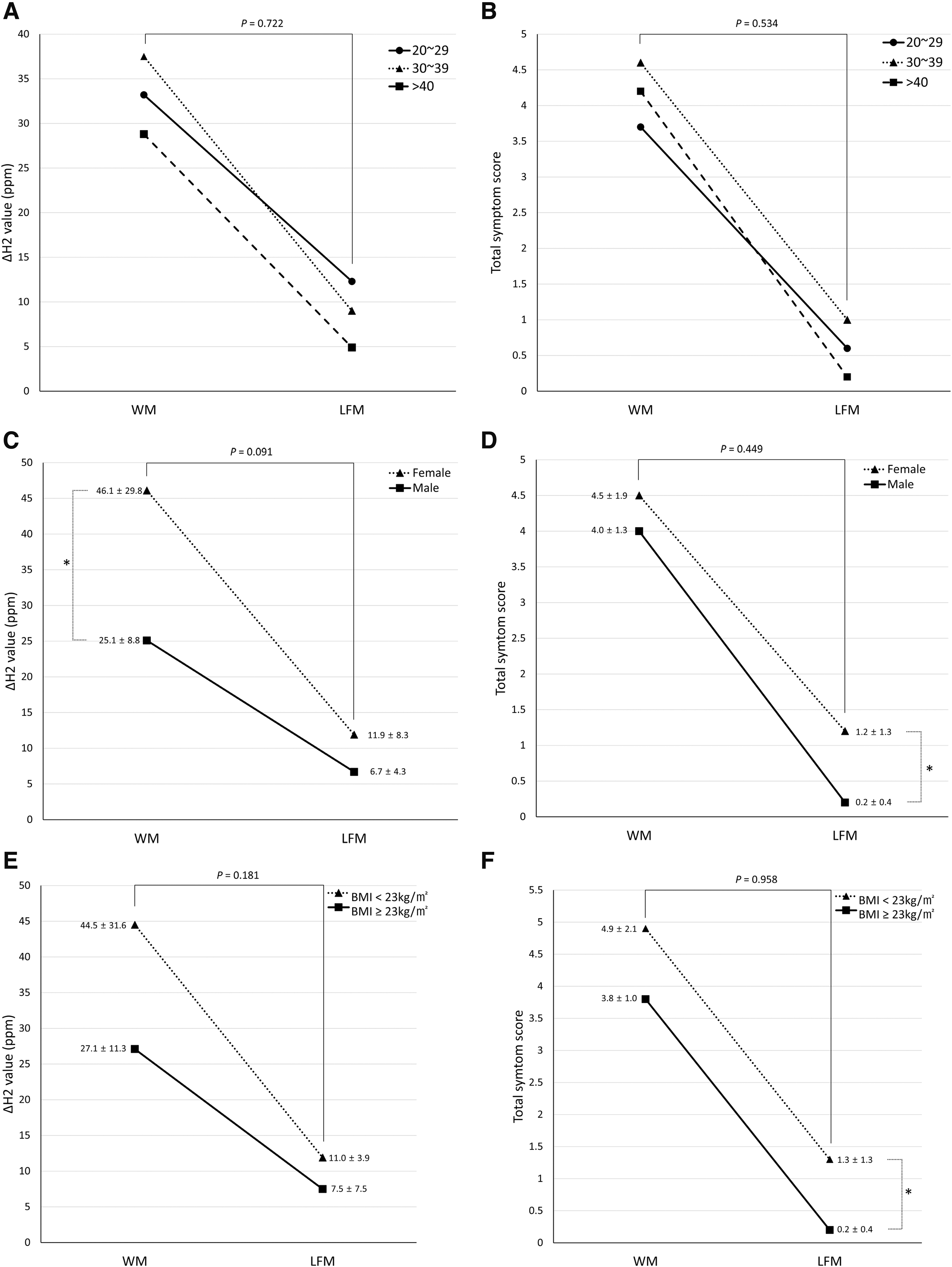
The differences in total symptom scores and peak ΔH2 values of HBT between WM and flavored LFM, stratified by age
Although all participants experienced symptoms when consuming the WM-HBT, 11 (39.3%) experienced symptoms with the LFM-HBT, with a mean symptom score of 1.5 ± 1.0. The participants with symptoms when using the LFM-HBT had significantly lower BMI than those who did not have symptoms (21.3 ± 2.4 vs. 23.3 ± 2.5, P = .049). Although the proportion of women was higher in the group with symptoms than in the group without symptoms (63.6% vs. 23.5%), it did not reach statistical significance (P = .084). There were no differences in age and ΔH2 values when consuming WM-HBT and LFM-HBT between the two groups (Table 1), and the total symptom score decreased in most participants using the LFM-HBT, from 4.3 ± 1.6 to 1.5 ± 1.0 (Table 1). Only one 42-year-old woman showed no difference in symptom scores of 2 (abdominal pain and diarrhea) between the two tests, but the ΔH2 value had significantly decreased from 55 to 11 ppm.
Characteristics of Enrolled Participants by Symptom During the Hydrogen Breath Test Using Lactose-Free Milk
Data are presented as mean ± SD. Comparisons between groups were analyzed by t-test or Mann–Whitney U-test.
HBT indicates the hydrogen breath test using whole milk.
LFM-HBT indicates hydrogen breath test using lactose-free milk.
BMI, body mass index; HBT, hydrogen breath test; LFM, lactose-free milk; SD, standard deviation; WM, whole milk.
DISCUSSION
LI is a common health problem that highly impacts nutritional intake and quality of life owing to the avoidance of dairy products. Therefore, the purpose of LI management is to improve lactose-related symptoms and to avoid the risk of malnutrition/undernutrition in the long term. 8 Although the strategy of restricting the consumption of lactose-contained foods is most commonly implemented, it results in critical nutritional limitations. Thus, pertinent strategies to alleviate symptoms through various interventions without restricting food intake, such as lactose-reduced or lactose-free diet, oral lactase supplementation, use of probiotics, or colonic adaptation through gradual increases in the dietary lactose load are needed. Among them, lactose-reduced or lactose-free diets are the most easily achievable and effective method, but previous studies have not shown clear and convincing evidence. 2,16 In this study of participants diagnosed with LI by the HBT and symptom questionnaire results, we found a significant reduction in the breath hydrogen concentration and symptom scores with flavored LFM. Although these findings were consistent regardless of age, sex, and BMI, the degree of symptom improvement after ingestion of LFM was somewhat lower in women and in the low BMI group (<23 kg/m2) groups than in their male and high BMI counterparts.
The LFM used in this study had the lactose eliminated by lactase treatment and ultrafiltration. Previous studies on LFM have shown inconsistent results. 16,20 In a systematic review from the National Institutes of Health (NIH) conference that assessed evidence on the effectiveness of clinical interventions for the treatment of LI from 36 randomized trials, 16 lactose-reduced or hydrolyzed milk did not consistently reduce gastrointestinal symptoms related to LI compared with regular milk. 16 Lactose-free dairy products are widely available around the world, but they were not marketed until 2016 in South Korea, although the prevalence of LI is high. Accordingly, studies on the efficacy of LFM in Asian populations are sparse and, to our knowledge, we reported the efficacy of LFM in South Koreans with LI for the first time. 21 Although flavored milk facilitates sufficient micronutrient intakes, such as that of calcium, the effect of added sugar has not been investigated. 17,18 In this study, we showed that flavored LFM reduced LI-related symptoms and hydrogen production in South Korean adults with LI.
Another review by Levitt et al demonstrated that 14 studies with >15 g lactose dosages showed mixed results on the efficacy of lactose-reduced products, 2 but only one study showed a significant improvement in the overall symptom score. 22 In terms of individual symptoms, improvement in abdominal pain, diarrhea, or flatulence was reported in 5, 2, and 6 of the 14 studies, respectively. In contrast, the other five studies showed no significant improvement in the overall or individual symptom scores. 2 There are several potential explanations for these findings including the use of insufficient lactose dosages, limitations in methodology, such as HBT, and characteristics of enrolled participants. The lack of improvement can be attributed to uninvestigated FGIDs. Because many patients are sensitive to various nutrients other than lactose and mechanical and chemical stimuli, they would not be expected to respond to restriction of lactose alone. 23
In our study, one female participant who did not show improvement in symptoms (abdominal pain and diarrhea) with LFM may have had hypersensitivity to some ingredients other than lactose. Furthermore, studies have reported a higher frequency of visceral hypersensitivity or IBS in women than in men. 24,25 Moreover, the result of less improvement in symptoms after taking LFM in women than in men found in our study supports this explanation.
On the contrary, it is known that gas-related symptoms such as bloating and borborygmi occur more frequently after lactose ingestion in IBS patients compared with healthy individuals. 26,27 Accordingly, foods high in lactose may be considered high fermentable oligosaccharides, disaccharides, monosaccharides, and polyols diet that aggravates gastrointestinal symptoms include bloating and flatulence. 28 Although avoidance of dairy foods seems simple and easy for these patients, it impairs health-related quality of life. 14,28 Therefore, LFM may be a potential treatment option not only for LI patients but also for FGID patients such as those with IBS in terms of symptom control and quality of life.
Of interest, all the participants complained of gastrointestinal symptoms after the consumption of dairy products including milk in their usual life, but many of them (40 of the 70 participants) were excluded after the first HBT. The excluded participants did not meet the HBT criteria for LI and 15 of them had no significant symptoms after ingesting WM. There is evidence of a weak association between self-reported LI and objective evidence of LI on HBT. 27,29 A systematic review of 28 studies demonstrated that ∼27–97% of the patients with a positive HBT result reported symptoms after lactose ingestion compatible with LI. 29 Although the proportion of the review was highly variable, 42.9% (30 of 70 participants) in this study did not deviate significantly from that in previous studies. Considering the inconsistent and unreliable diagnostic performance of self-reported LI, clinicians should be cautious when recommending lactose-restricted diets to all patients. Alternatively, it is recommended that they recommend dairy products containing a tolerable dose of lactose, usually <12 g, 16 or to investigate for other FGIDs.
Although all the participants denied the presence of recurrent gastrointestinal symptoms or any history of diagnosed FGIDs or psychiatric disorders, some of them may have had undiagnosed conditions. However, by excluding the participants with these diseases, we were able to recruit participants who met the subjective and objective diagnostic criteria for LI. Because we used readily available WM instead of pure lactose for the HBT, the accuracy of the test may differ from that in previous studies. However, we believe that our findings can be easily applied to clinical practice because the use of milk available in the market reflects real clinical situations.
This study had some limitations. One major limitation is that the protocol of HBT was suboptimal in terms of cutoff values of ΔH2, test duration, and dose of lactose. A recent consensus suggested a lactose dose of 25 g and a rise of ≥20 ppm from baseline as the positive result for the HBT. 19 The test should be performed over at least 3 h to capture colonic fermentation. In our pilot trial, most participants did not meet the HBT criterion of ΔH2 of >20 ppm despite having severe gastrointestinal symptoms. We arbitrarily selected 16 ppm as the cutoff value of ΔH2. In addition, we performed the HBT only over 2 h because we did not find a significant difference in the results of the tests performed over 2 and 3 h in the pilot study. Consequently, our arbitrary decision may have influenced participant selection and outcomes.
Next, we used commercially available WM and LFM instead of pure lactose. Therefore, the participants diagnosed with LI in this study may not have met the diagnostic criteria. Finally, all milk samples used in this study were packaged without any label on the outside to eliminate the placebo effect according to the recommendation of the NIH consensus. 30 Initially, we tried to determine the difference between WM and LFM in each subject. Thus, randomization was not possible for our study purposes. In addition, informed consent was obtained after fully explaining the purpose and design of the study. Accordingly, it was insufficient to obtain a blinding effect because WM was first used for participant screening. Because of these limitations, future studies with larger samples are needed to determine the efficacy of LFM in helping patients with LI using clear diagnostic criteria and a large number of participants.
In conclusion, this study demonstrated that flavored LFM is well tolerated by South Korean adults diagnosed with LI based on HBT and symptom questionnaire results. Therefore, it may be a viable alternative for those who cannot consume WM products.
Footnotes
AUTHORs' CONTRIBUTIONS
J.-W.K. and Y.W.C. planned and designed the study; C.H.O., Y.M.P., H.Y.K., and J.K.P. enrolled patients; C.H.O. and Y.M.P. performed the test; Y.M.P. and J.-W.K. performed the statistical analysis; Drafting of the article was performed by C.H.O. and J.-W.K.; critical revision of the article for important intellectual content was performed by Y.M.P., J.-Y.J., and Y.W.C.; J.O.Y., H.Y.K., and J.K.P. contributed to critical review in the field of nutrition and food. All the authors have approved the final draft submitted including the authorship list. J.-W.K. had full access to the data and final responsibility for the decision to submit for publication.
AUTHOR DISCLOSURE STATEMENT
J.O.Y., H.Y.K., and J.K.P. are employees of the funding company (Research and Development Center, Maeil Daires Co., Ltd.) for this study. C.H.O., J.W.K., Y.M.P., J.Y.J., and Y.W.C. report no disclosures.
FUNDING INFORMATION
This study was supported by the Maeil Daires Co., Ltd. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, or in the writing of the article.
SUPPLEMENTARY MATERIAL
Supplementary Table S1