
Abstract
The putative hypolipidemic properties of scopoletin have not been fully confirmed due to a lack of validation in an irreversible chronic hyperlipidemia animal model. The druggability also needs to be studied in terms of bioavailability in the vascular compartment. Accordingly, we conducted a study to assess the hypolipidemic and pharmacokinetic behavior of scopoletin in the high-fructose high-fat diet (HFHFD)-induced dyslipidemia model in Wistar rats. A total of 42 rats were studied, with 6 in each of the 7 groups. A 60-day HFHFD opted for induction of dyslipidemia. Group I and groups II–VII received normal rat chow diet and HFHFD, respectively. Oral scopoletin (1, 5, 10 mg/kg) and atorvastatin 5 mg/kg were administered in groups III–VI, respectively, once daily for the next 15 days. A separate group, group VII, was used for the pharmacokinetic assessment comparing the scopoletin 10 mg/kg intraperitoneally (IP) in group VII versus the oral (group V). Pharmacokinetic blood sampling was performed on the 10th day of continuous once-daily therapy. Rats were sacrificed for the histological examination. All three scopoletin dosages significantly decreased the total cholesterol, low-density lipoproteins, and triglycerides (P < .05 for all), but not in a dose-dependent manner. Atherogenic Index of plasma, Castelli's risk indices, and histopathological findings confirmed the protective effect of scopoletin. The IP administration showed a 23.18% higher exposure than the oral route (P < .001 for area under the curve and P < .05 for concentration-maximum). This study confirms the hypolipidemic efficacy of scopoletin in a more robust irreversible model of dyslipidemia. Scopoletin's gut absorption in the disease state may also boost the initial phase exploratory clinical trial.
INTRODUCTION
Lipoprotein derangement has become a common disorder due to dependence on computers, mobile phones, social media platforms, unhealthy eating habits, and sedentary lifestyle. Concurrent oxidative stress neutralizes antioxidant defenses in the body leading to another comorbidity, atherosclerosis. 1 The vicious cycle continues and leads to more cardiovascular disease burden in terms of increased mortality and health economic burden on patients and the family. The existing pharmacotherapeutic approaches suggest using first-line medicines such as statins or fibrates to manage hyperlipidemia.
However, these drugs have limitations in the form of adverse event profiles and eventual resistance. Combination therapies are not actively considered due to similar hepatotoxicity potential associated. 2 The research on discovering newer lipid-lowering agents is ongoing, for example, evolocumab and alirocumab discovery. These costly injectable preparations are associated with hypersensitivity propensity and the limited indication spectrum, that is, in statins and combination therapy failure patients. Therefore, newer medications are not suggested as first-line drugs for managing hyperlipidemia. 3
Ayurveda, an ancient medical science of Indian origin, heavily relies upon medicinal plants for almost all states of ill-health. Plant-based medicines are generally assumed to have a wider safety profile, as shown by toxicity studies conducted on animals with daily doses in grams. 4 Bridging the gap between Ayurvedic suggestions and the currently difficult-to-treat scenarios is possible through properly conducted in vitro and in vivo animal studies to further justify consideration in clinical trial settings. 5 Earlier studies by our group showed hypolipidemic action of crude plant extract of Convolvulus pluricaulis in a triton-induced hyperlipidemia model in rats. The same study also identified scopoletin in the plant extract that might be responsible for its hypolipidemic action. 6,7
Scopoletin has been studied for several clinical indications, such as anti-inflammatory and hepatoprotective action, besides its action on lipid and glucose metabolism. 8 –11 The present study was planned to validate the efficacy of scopoletin action in high-fructose high-fat diet (HFHFD)-induced hyperlipidemia. HFHFD-induced hyperlipidemia is an irreversible model closely mimicking chronic lipoprotein derangement as observed in clinical settings. To the best of our knowledge, scopoletin has not been evaluated pharmacologically for chronic irreversible hyperlipidemia in animal models. The present study further tries to answer the drug candidature of scopoletin by pharmacokinetic assessment.
MATERIALS AND METHODS
In-house HFHFD preparation
The high-fat diet was prepared according to the study by Srinivasan et al.,
12
and the diet consisted of the following constituents (g/kg): Powdered normal pellet diet-365, Lard-310, Casein-250, Cholesterol-10, Vitamin and mineral mix-60,
Animals
All animal experiments were performed following the “Committee for Control and Supervision of Experiment on Animals (CCSEA) guidelines.” Wistar rats of either sex weighing 150–200 g were housed in standard polypropylene cages with two rats per cage in compliance with the institutional animal housing rules. Food and water were provided ad libitum, and a 12-h light/dark cycle was maintained. Relative humidity and temperature were set at 55% ± 5% and 22°C ± 2°C, respectively. Seven days of acclimatization period was observed before the start of experimental procedures. All the animal procedures and protocols were approved by the Institutional Animal Ethics Committee (764/IAEC/110 held on October 27, 2020) of the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh. The ARRIVE (Animal Research: Reporting of In Vivo Experiments, version 2.0) guidelines were followed during conduct and reporting of the study.
Experimental design
We used a total of 42 rats in this present study. The animals were divided equally into seven groups (n = 6). Animals were fasted overnight with free access to water before the experiment. On the day of the experiment, baseline lipid profile parameters were measured. Group I served as the normal control (NC), receiving distilled water alone, and group II served as experimental control (EC), receiving HFHFD as a disease-inducing agent. Groups III, IV, and V were study groups that received HFHFD, followed by scopoletin 1, 5, and 10 mg/kg, respectively. Group VI served as a positive control (PC), receiving HFHFD followed by atorvastatin 5 mg/kg orally. Group VII served as the bioavailability comparator group (to group V rats) that received HFHFD, followed by high-dose scopoletin (10 mg/kg) intraperitoneally (IP).
Induction of dyslipidemia and study medication intervention
We provided a regular chow diet to group I and HFHFD to the remaining groups, namely groups II, III, IV, V, VI, and VII, for 60 days, respectively. After 60 days, the model induction was confirmed with a biochemical analysis of blood samples. The test medications were administered daily after that, for 2 weeks orally.
Biochemical assessment in the blood samples
Serum was collected after centrifugation of blood samples at 7400 g for 5 min and stored at −80°C until analysis. Lipid parameters such as total cholesterol (TC), triglycerides (TGs), low-density lipoproteins (LDL), and high-density lipoproteins (HDL) were measured using Roche biochemical test kits with a semi-auto analyzer by colorimetric methods.
Assessment of various indices
Atherogenic index
The Atherogenic Index of plasma (AIP) is a well-validated index that helps in cardiac risk estimation. 8 Increases in the lipid profile parameter levels make individuals more prone to atherosclerotic complications. 13
% Protection
Castelli's risk index (CRI)
CRI-I:
It is also known as cardiac risk ratio. It reflects coronary plaque formation and has a diagnostic value as good as TC.
CRI-II:
It is an excellent predictor of long-term cardiovascular risk. It has been correlated reasonably well with insulin resistance and acute myocardial infarction prediction.
High-performance liquid chromatography standardization of scopoletin in the mobile phase and rat plasma matrix
Scopoletin standard, Methanol (high-performance liquid chromatography [HPLC] grade), ortho-Phosphoric acid (min 88% Guaranteed Reagent), and 8-methoxypsoralen were purchased from Sigma–Aldrich, USA. Lipid parameter assessment kits were obtained from Roche Co., Ltd. Scopoletin is available with several chemical vendor companies and online sellers as a pure plant extract phytochemical powder (HPLC grade). However, a voucher specimen was still maintained at the Department of Pharmacology, PGIMER, with a voucher specimen (ANP/PGI/Pharma/SCO001/22) for future reference.
The scopoletin primary stock solution was made using methanol at a 1 mg/mL concentration. Once prepared, the primary stock solution was covered and stored at 4°C. Working standard solutions for scopoletin were diluted from primary stock solutions with methanol. The calibration standards of scopoletin were arranged by serially diluting blank plasma to yield final concentrations of 0.19, 0.39, 0.78, 1.56, 3.125, 6.25, 12.5, 25, 50, and 100 μg/mL. Control samples were prepared at the same concentrations as those in the rat plasma samples for calibration. In a constant volume of internal standard, calibration standards of different concentrations of scopoletin were prepared as: 3.125, 6.25, 12.5, 25, 50, and 100 μg/mL. The 100 μL volume of 8-methoxypsoralen (internal standard) was added.
Pharmacokinetic blood sampling and assessment
Blood sampling was performed on the 10th day of continuous once-daily therapy at 0 h, 0.1, 0.17, 0.25, 0.3, 0.5, 0.75, 1, 1.5, and 2 h post-dosing. Inhalational ketamine anesthesia and retro-orbital sinus blood sampling were used to obtain an average blood volume of 350 μL. The Microsoft Excel 2016 version with the built-in “Forcast” function was utilized for the pharmacokinetic assessment (trapezoid rule method). Different time point concentration data were compiled for the study groups and later used for pharmacokinetic (PK) parameters calculation, such as the area under the curve (AUC), half-life, clearance, and the volume of distribution (Vd).
Histological examination
We sacrificed the rats at the end of the experiment. Liver tissue was cautiously removed and fixed with a 10% formalin solution. For histological studies, the tissue paraffin sections were stained later with hematoxylin–eosin and examined under the microscope.
Statistical analysis
SPSS version 26 was used for the statistical analysis. All the data obtained are expressed as mean ± standard error of the mean. One-way analysis of variance (ANOVA) followed by Bonferroni post hoc test was performed for day 60 and day 75 for various parameters.
RESULTS
Lipid parameters assessment
Lipid profile at day 0
Lipid parameters such as TC, TG, LDL, and HDL showed no statistical difference in intergroup comparisons among all groups at baseline (P > .05).
Model induction on day 60
The hyperlipidemia model induction was evident from the different lipid parameters at day 60 after feeding the rats with HFHFD. The animal groups showed significant changes in lipid profile parameters compared with the NC group. There was a significant increase in TC (84.47 ± 1.12 in EC vs. 52.76 ± 1.85 in NC), LDL (28.08 ± 1.20 in EC vs. 7.4 ± 0.49 in NC), and TG (156.33 ± 24.29 in EC vs. 49 ± 2.64 in NC). However, HDL levels were declining (43.47 ± 2.33 in EC vs. 44.28 ± 0.07 in NC) toward the end of 2 months. Other groups fed with HFHFD also showed a significant rise in lipid parameters compared with the NC group. However, HDL levels were significantly reduced (P < .05) (Fig. 1).
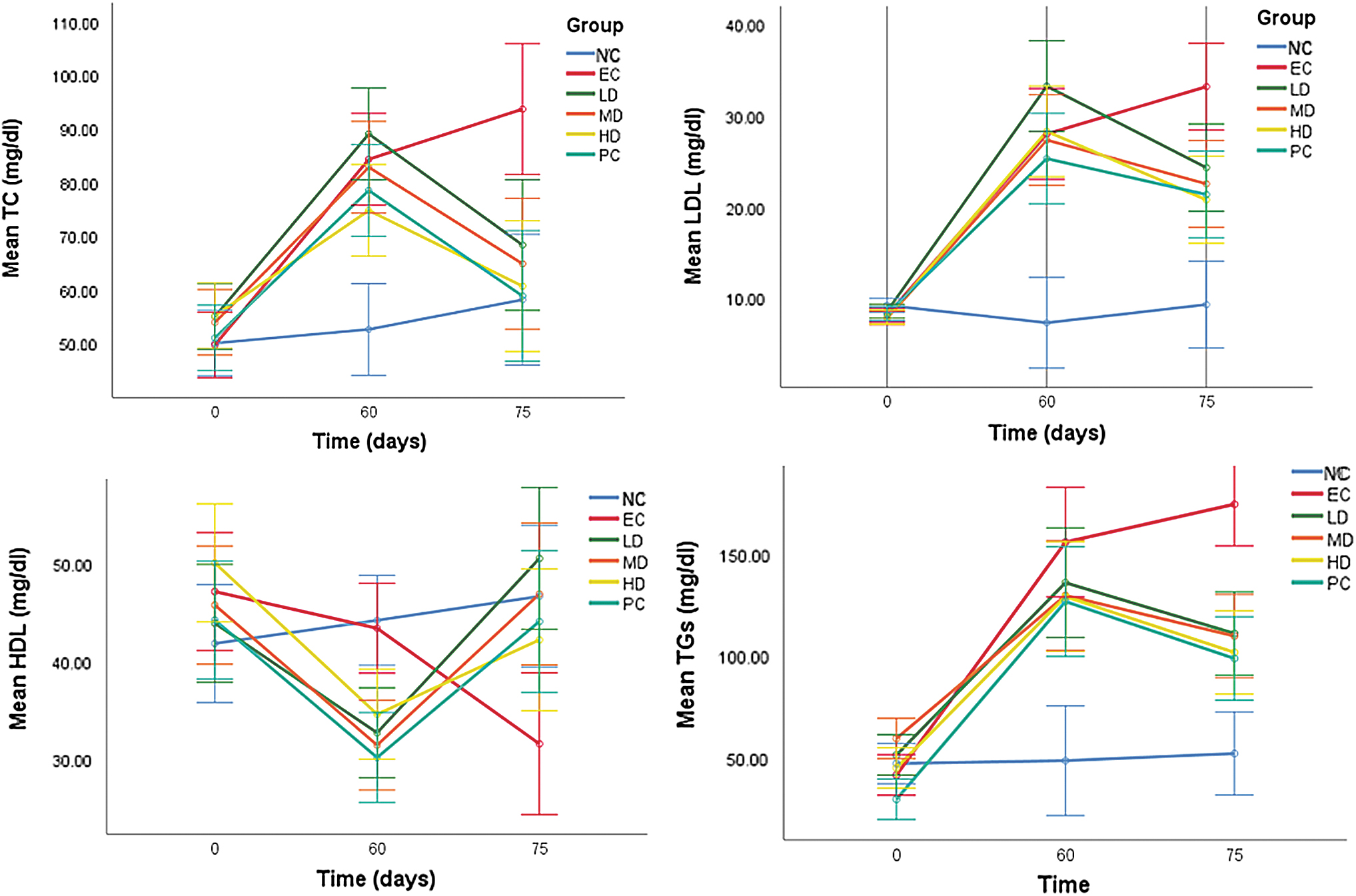
Repeated-measures analysis of variance test applied showing high-fructose high-fat diet-induced hyperlipidemia model development.
Effects of 2 weeks of regimens of various interventions on lipid profile
We observed a significant decrease in lipid parameters in the atorvastatin-treated group evident from day 75 serum levels of TC (59.00 ± 7.24 vs. 93.83 ± 8.06 in the EC group), LDL (21.45 ± 2.66 vs. 33.26 ± 3.43 in the EC group), and TG (99.16 ± 8.407 vs. 174.96 ± 11.74 in the EC group) (P < .05). Similarly, the atorvastatin-treated group also showed a rise in HDL levels (44.16 ± 1.77) compared with the EC group (31.66 ± 2.27) (P < .05).
All three doses of scopoletin, that is, low, medium, and high, produced a statistically significant decline in lipid parameters after successive days of treatment in a once-a-day dosing pattern. The low dose (LD) (mg/dL) level readings (68.5 ± 5.81 in the LD group; 65.00 ± 5.170 in the medium dose [MD] group; and 60.83 ± 5.84 in the high dose [HD] group) were found to be decreased in scopoletin dosage groups when compared with the EC group (93.83 ± 8.06) (P < .05). The LDL (mg/dL) levels (24.4 ± 2.705 in LD; 22.61 ± 1.86 in MD; and 20.87 ± 1.63 in HD) were reduced with scopoletin at the three dosages compared with those in the EC group (33.26 ± 3.43) (P < .05). The TG (mg/dL) levels (136.4 ± 16.72 in LD; 110.2 ± 16.83 in MD; and 102.16 ± 8.498 in HD) were observed to be reduced in all three scopoletin dose groups when compared with those in the EC group (174.96 ± 11.74) (P < .001). However, an appreciable increase in HDL (mg/dL) levels was observed, but it was statistically significant only in the low-dose group (50.6 ± 4.58) compared with the EC group (31.66 ± 2.27) (P < .05) (Table 1).
Effect of Different Interventions on Various Lipid Profile Parameters on Day 0, Day 60, and Day 75
Data are expressed as mean ± standard error of the mean. One-way analysis of variance, followed by Bonferroni post hoc test applied on day 60 and day 75.
P < .001 versus NC; * P < .05 versus NC; † P < .05 versus EC; ** P < .0001 versus NC; # P < .001 versus EC.
EC, experimental control; HD, high dose; HDL, high-density lipoproteins; LD, low dose; LDL, low-density lipoproteins; MD, medium dose; NC, normal control; PC, positive control; TC, total cholesterol; TGs, triglycerides
A repeated-measures ANOVA test was also applied to check the model development and effects of different interventions from day 0 to day 75 (Fig. 1).
Effects of various interventions on AI of plasma and percent (%) protection on day 75
Serum AI was higher in EC (2.05 ± 0.37 vs. 0.30 ± 0.12 in NC) (P < .0001), whereas the atorvastatin-treated group showed a significant decline (0.38 ± 0.23) when compared with the EC group (P < .001) on day 75. The scopoletin-treated groups showed a significant decline in AI (0.41 ± 0.19 in LD; 0.42 ± 0.16 in MD; and 0.49 ± 0.18 in HD) in comparison to the EC group (2.05 ± 0.37) (P < .001). The percent protection in the atorvastatin-treated group was observed to be 81.62%. There was a statistical difference in the percent protection observed with scopoletin-treated groups when compared between the groups (79.82 ± 9.59 in LD; 79.53 ± 7.97 in MD; and 75.88 ± 8.83 in HD).
Effect of various interventions on CRI-I and CRI-II on day 75
Castelli's risk index-I
A significant increase was observed in CRI-I of EC (2.69 ± 0.31) compared with the NC group (1.304 ± 0.124) (P < .0001). It indicates the increased risk of cardiovascular risk in the EC group rats receiving the HFHFD compared with the NC group receiving a regular chow diet. On day 75, the atorvastatin-treated group showed a significant decline in CRI-I (1.377 ± 0.225) in comparison to the EC (2.69 ± 0.31) (P < .0001). Fifteen days of treatment with scopoletin significantly reduced CRI-I (1.23 ± 0.02 in LD;1.07 ± 0.05 in MD; and 1.64 ± 0.09 in HD) compared with the EC group (2.69 ± 0.31) (P < .001).
Castelli's risk index-II
The atorvastatin-treated group showed a significant decline in CRI-II (0.5006 ± 0.204) compared with the EC group (1.083 ± 0.147) (P < .0001). Fifteen days of treatment with scopoletin also significantly reduced CRI-II (0.5043 ± 0.078 in LD; 0.496 ± 0.201 in MD; and 0.510 ± 0.208 in HD) compared with the EC group (1.083 ± 0.147) (P < .001) (Table 2).
Effect of Different Interventions on Atherogenic Index, Percent Protection, and Castelli's Risk Indices I and II
Data are expressed as mean ± standard error of the mean. One-way analysis of variance on day 60 and day 75, followed by Bonferroni post hoc test.
P < .0001 versus NC; * P < .001 versus EC; # P < .05 versus NC; ** P < .0001 versus EC; † P < .05 versus EC.
CRI, Castelli's risk index.
Pharmacokinetic HPLC method development
The HPLC analysis was performed using the Synergi 4-u Fusion reverse phase-80 A column (150 × 4.6, 4 μg). The analysis used 0.05% (v/v) phosphoric acid with methanol and distilled water (49:51 v/v) as the mobile phase at a flow rate of 1 mL/min. The pressure was set at 2300 psi with temperature maintained at 25°C. Chromatograms were extracted at 345 nm. The retention time was determined to be 3.26 min. The calibration curve of scopoletin in mobile phase, that is, methanol (Fig. 2A) and in blank rat plasma (Fig. 2B) was developed. The same method was used later for pharmacokinetic analysis of scopoletin in study rats (Fig. 3A).
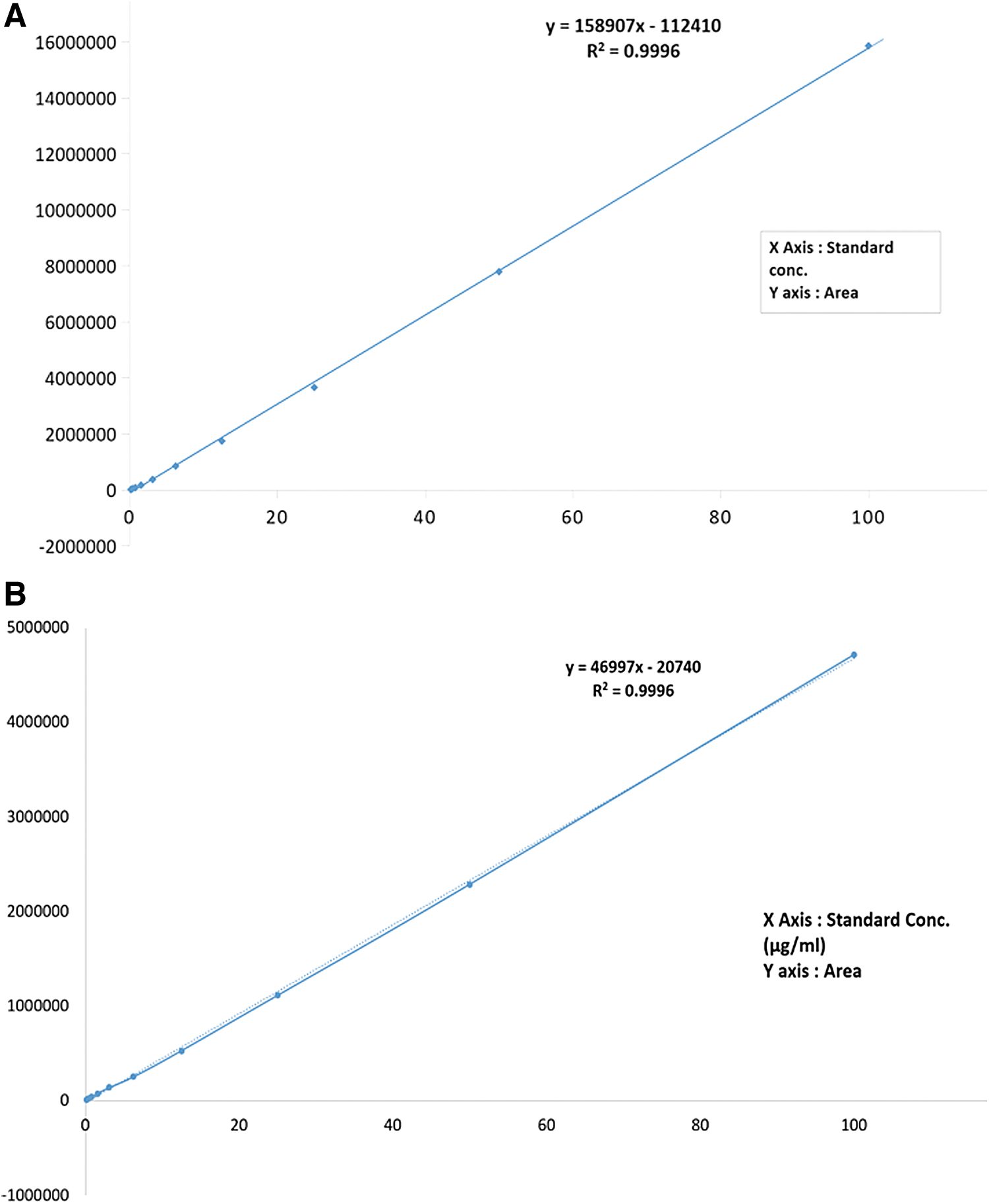
Standardization (calibration) of scopoletin estimation method in the mobile phase
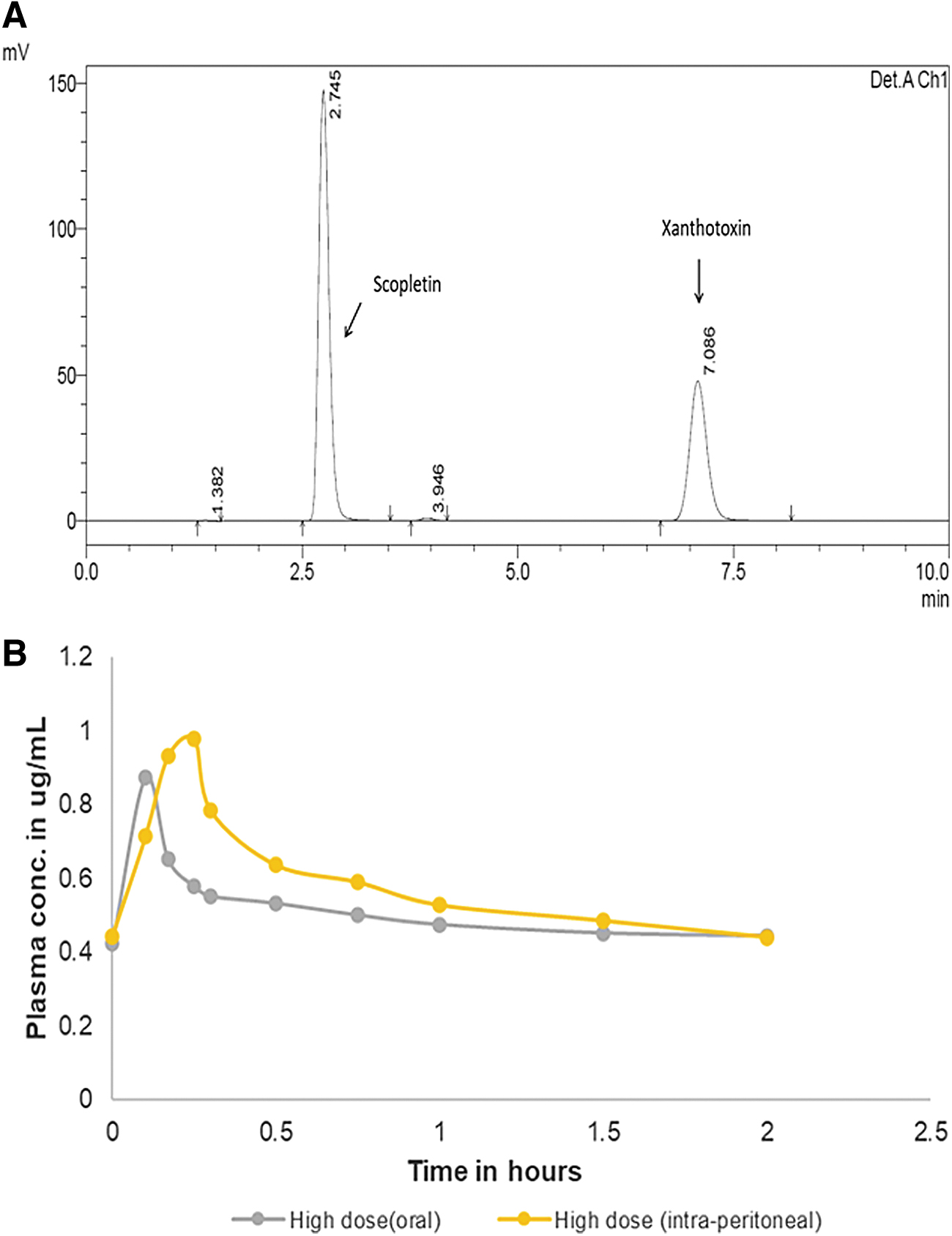
Estimation of scopoletin in rat plasma in the presence of internal standard xanthotoxin
Rat plasma scopoletin concentration assessment
High-dose oral scopoletin (10 mg/kg) reached its peak plasma concentration (Cmax, 0.87 ± 0.049) at 0.1 h and then declined. The Cmax after IP injection of scopoletin (10 mg/kg) was found to be 0.99 ± 0.092 μg/mL at 0.25 h (P = .02). The t½ of high-dose scopoletin given by IP route was 0.41 h, while it was 0.6 h for the oral route. However, no statistical difference was observed between the t½ half-lives of the two groups (P = .39).
The two groups were compared for relative AUCs. The AUC of the IP-administered scopoletin group was higher than the orally administered group (1.43 vs. 1.09) (P < .001). The clearance of the drug by both the routes of drug administration was observed to almost similar (26.25 L/h in oral vs. 24.04 L/h in IP group) (Fig. 3B).
Histological findings
In the HFHFD-fed EC group, the liver showed inflammation in the portal tract, whereas in the scopoletin-treated group, these changes were reversed similarly to those in the NC group (Fig. 4).
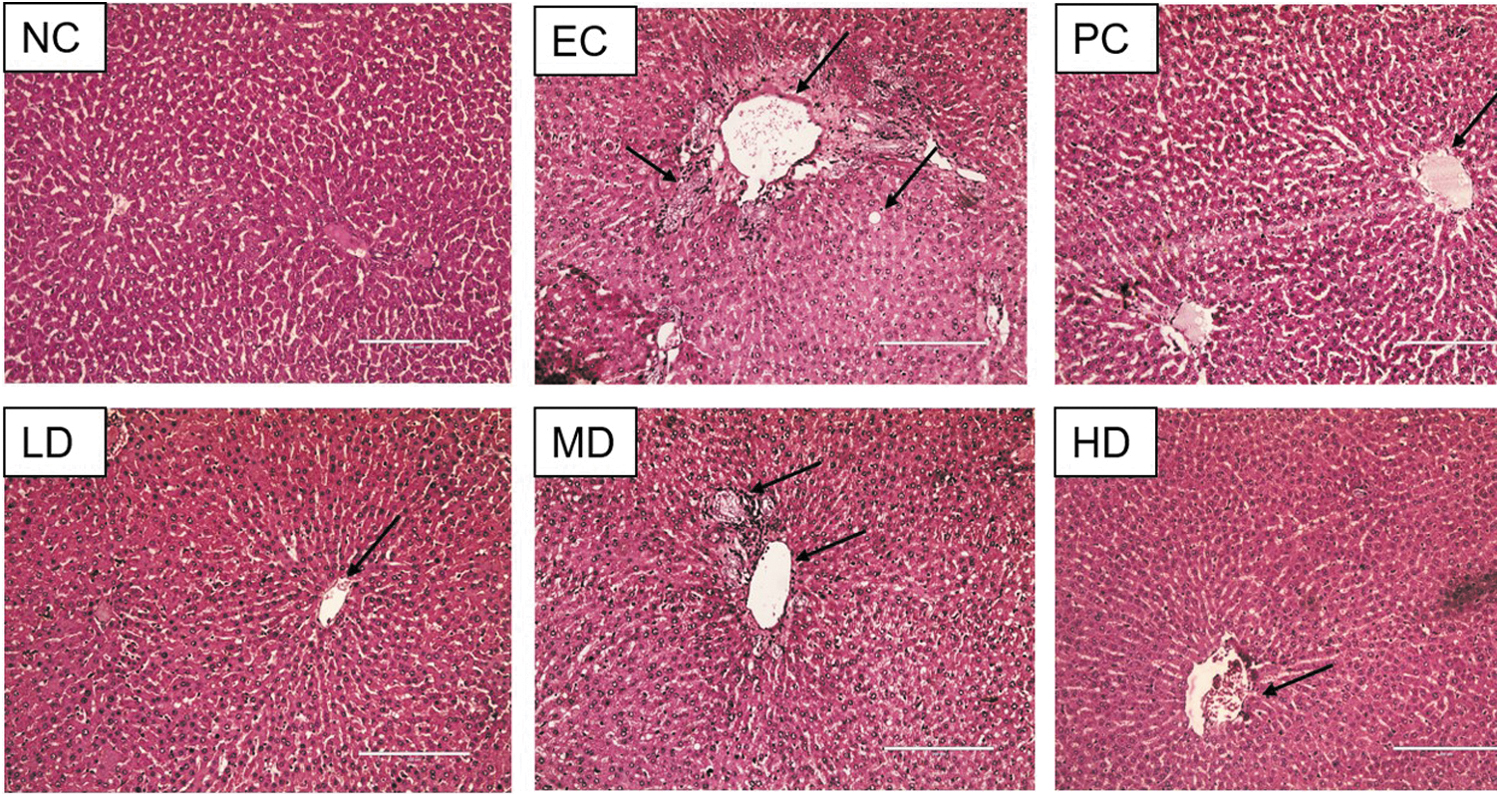
Effect of different interventions on liver morphology of rats (magnification 20 × ).
DISCUSSION
The present study was carried out to study hypolipidemic efficacy and pharmacokinetic assessment of scopoletin via two different routes in a chronic irreversible hyperlipidemia model. The previous reports have suggested the role of scopoletin in a reversible liver injury model and in vitro experiments. 6 Scopoletin is a phytochemical identified in roots and leaves of Datura metel, Mallotus resinosus, Solanum nigrum, Viburnum prunifolium, and many other plant species. Plant-based remedial solutions containing various combinations and permutations of phytochemical extracts have been mentioned and practiced for ages as a part of Ayurvedic medicine in Asian continents. 14,15
High-fat diets closely mimic the dietary habits of the present world in a fast-paced life, producing irreversible hyperlipidemia. 12,13 The model developed in the present study showed a rise in TC, TG, and LDL concentration with a reduction in the HDL concentration on day 60 of diet intervention. The daily administration of various scopoletin doses (1, 5, 10 mg/kg) for 15 days suppressed the rising levels of TC, TG, and LDL with a smaller action on the HDL component. In the HD group, the increase in HDL was less than that in the LD group, even though the decrease in TG was greater in the HD group. It can be deduced that in the HD group, HDL particles became smaller than in the LD group. It further supports the accumulating evidence on the regulation of hyperlipidemia. The LDL-C value, oxidative state, and particle sizes all affect atherogenicity. In contrast, the HDL-C value is no longer believed to be a decisive risk factor for ischemic disease, but only one factor that may affect atherogenicity.
The well-validated PC, atorvastatin, produced a statistically significant effect on all four lipoproteins. 16,17 Concurrent reduction in TC and LDL with scopoletin suggests a putative mechanism similar to the statin group of drugs. The hydroxymethylglutaryl-coenzyme A inhibitor statins have a maximum impact on TC and LDL levels by facilitating the hepatic uptake and removal of lipoprotein via the hepatic–bile route, cleaning the vascular compartment. The sequence of actions results in reduced plaque formation, atherosclerosis, and vascular risks. 18 Histopathological findings, AIP, percent protection, and CRI-I and II further supported the present study's results. Hyperlipidemia is associated with macrophage proliferation coupled with LDL oxidation. It subsequently leads to the deposition of the same in the form of plaques in blood vessel lumens in different organs. AIP and percent protection covers the same pathological events prediction in the animal mode. 6 The present study also attempted to evaluate future complication risks associated with hyperlipidemia.
The complication prediction correlation is better with evaluating CRI-I and CRI-II. These two formulas utilize the same biochemical information to depict coronary plaque formation and susceptibility to cardiovascular event occurrence. 19 The different doses of scopoletin exhibited benefits as good as atorvastatin on all three indices. Our findings are consistent with the results of Lee et al., which showed hepatoprotective action and cholesterol-lowering capacity of scopoletin in an alcohol and high-fat diet-induced hepatopathy mouse model. 9 One in vitro study tried mechanistic exploration for the hypolipidemic action and showed sirtuin-1 as a scopoletin target in a HepG2 cell line experiment. Sirtuin-1 is a nicotinamide adenine dinucleotide-dependent protein deacetylase in the hepatic nucleus, regulating the sterol regulatory element-binding protein-1c pathway. The experiment also demonstrated the subsequent downregulation of lipogenic genes. 11
In the last phase of the study, we assessed and compared the relative pharmacokinetic behavior of 10 mg/kg scopoletin administered via oral and IP routes. The study observed statistically significant differences in AUC and Cmax findings with two different routes of administration. This study confirms the oral absorption of the single phytochemical and easy compatibility with vehicle distilled water. The study also demonstrated a 23.18% rise in relative bioavailability with the IP route compared with oral route of drug administration. To the best of our knowledge, there is no study in the literature comparing the bioavailability of scopoletin by two different routes and simultaneously assessing oral bioavailability in diseased state rats. This PK finding has two significant implications. The study will pave the way for formulation-based studies and guide initial phase exploratory clinical trials.
Due to funding limitations, the current study could not further explore mechanisms for the observations and use the ideal pharmacokinetic comparator, that is, intravenous scopoletin. Evaluation of pharmacokinetic association with hypolipidemic effects could not be performed due to positive and negative side changes over the treatment duration.
In conclusion, this study confirms in vitro and initial in vivo findings in a more robust irreversible model of hyperlipidemia. The phytochemical is eligible for early phase exploratory clinical trials as well as pharmaceutical formulation-based studies.
Footnotes
ACKNOWLEDGMENTS
All authors would like to thank Mr. Sunil Sharma for HPLC standardization of the analytical method.
AUTHORs' CONTRIBUTIONS
A.N.P. designed the research. G.K.B., C.M., S.S., and A.A. performed all experiments. G.K.B. and A.N.P. analyzed the data. A.N.P. and G.K.B. wrote the article. A.B., S.B., S.R., and A.P. interpreted the HPLC, biochemical and histological data. A.P. and A.N.P. critically revised the article.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.