
Abstract
Diabetes mellitus (DM) is a chronic disease and one of the oldest known disorders. It is characterized by dysglycemia, dyslipidemia, insulin resistance (IR), and pancreatic cell dysfunction. Although different drugs, metformin (MET), glipizide, glimepiride, etc., have been introduced to treat type 2 DM (T2DM), these drugs are not without side effects. Scientists are now seeking natural treatments such as lifestyle modification and organic products known with limited side effects. Thirty-six male Wistar rats were randomized into six groups (n = 6 per group): control, DM untreated rats, DM+orange peel extract (OPE), DM+exercise (EX), DM+OPE +EX, and DM+MET. The administration was once daily through the oral route and lasted for 28 days. EX and OPE synergistically ameliorated the diabetic-induced increase in fasting blood sugar, homeostatic model assessment for insulin resistance (HOMA IR), total cholesterol (TC) and triglyceride (TG), TC/high-density lipoprotein (HDL), TG/HDL, triglyceride glucose (TyG) index, and hepatic lactate dehydrogenase, alanine transaminase, malondialdehyde, c-reactive protein, and tumour necrosis factor α when compared with the diabetic untreated group. Also, EX+OPE blunted DM-induced decrease in serum insulin, homeostasis model assessment of β-cell function (HOMA-B), homeostasis model assessment of insulin sensitivity (HOMA S), quantitative insulin-sensitivity check index (QUICK 1), HDL, total antioxidant capacity, superoxide dismutase, and hepatic glycogen. Furthermore, EX+OPE ameliorated the observed DM-induced decrease in glucose transporter type 4 (GLUT 4), expression. This study showed that OPE and EX synergistically ameliorate T2DM-induced dysglycaemia, dyslipidaemia, and down-regulation of GLUT4 expression.
INTRODUCTION
Diabetes mellitus (DM) is a chronic disease and one of the oldest known disorders. 1 The commonest type of DM is type 2 DM (T2DM), and it is characterized by dysglycemia, dyslipidemia, insulin resistance (IR), and pancreatic cell dysfunction. 2,3 Epidemiologically, ∼537 million people are living with DM, and it has been speculated that this figure will increase to 643 million by 2030. 4 An increase in morbidity and mortality is associated with T2DM because of its insidious onset and delayed diagnosis. 2
IR is the hallmark of T2DM and is connected with dysmetabolism, 5 an independent risk factor for diabetic complications. IR is the inability of the cells in the muscles, adipose tissue, and liver to respond optimally to insulin and unable to remove glucose from the blood. Insulin is a peptide hormone produced from the pancreatic β cells. It is responsible for maintaining glucose homeostasis by enhancing glucose uptake within the cells and maintaining carbohydrate, protein, and lipid metabolism. 6
Insulin maintains glucose homeostasis by stimulating glucose through the activation of the insulin-sensitive glucose transporter isoform 4 (GLUT4) at the plasma membrane. 7 Typically, GLUT4 is localized in the intracellular membrane. Still, the presence of insulin brings about its translocation from the intracellular membrane to the plasma membrane, where it helps transport glucose into the cell. After insulin is withdrawn, GLUT4 becomes internalized and returns to the intracellular membrane. 7 This piece of information shows the importance of GLUT4 in glycemic control, and its disruption has been implicated in dysglycemia and dyslipidemia. 8
Although different drugs, metformin (MET), glipizide, glimepiride, etc., have been introduced for treating T2DM, these drugs are not without side effects. Scientists are now seeking natural nutrients and lifestyle modification to reduce the side effects of these drugs. One of the natural ways to reduce DM complications are dietary and lifestyle modifications. Orange peel extract (OPE) has been reported to improve glycemic control, 9 and have antibacterial, 10 antioxidant, 11 and anti-inflammatory 12 activities. Furthermore, its antidiabetic and antihypercholesterolemic activities have been reported, 13 although sufficient information about its mechanism of action is lacking.
Another alternative factor for improving cell metabolic responses and insulin sensitivity is regular EX, which is known for relieving T2DM. 14 In fact, meta-analyses have repeatedly confirmed that T2DM patients observing anaerobic EX have better glycemic control, insulin sensitivity, and total oxidative capacity than their counterparts observing a sedimentary lifestyle. 15 EX has long been identified as management for T2DM, but it is the most underused. Despite the available information on the role of OPE and EX in T2DM management, no study has considered the possible synergistic effect of both in managing T2DM.
Also, their possible mechanism of action has not been fully established. This study was, however, designed to establish whether OPE and EX will synergistically reverse T2DM-induced dysmetabolism. Also, the role of GLUT4 in OPE and EX-induced glycemic control was probed.
MATERIALS AND METHODS
Animals
The animals used for this study were purchased from the biochemistry department at the University of Ilorin, Ilorin. They were handled carefully based on the Guidelines for Laboratory Animal Care published by the National Institute of Health (NIH). Ethical approval was obtained from the institutional ethical review committee. In total, 36 animals of similar weights (160–180 g) were housed in standard cages (n = 6 rats per cage). They were given unrestricted access to feed and water under the natural condition of 12 h cycle of light and darkness. After 2 weeks of acclimatization to their new environment, the animals were randomly divided into six groups, and the administration lasted 28 days. The dosage used in this study is similar to that used in Adeyemi et al. 16
Group 1: Control, received 1 mL/kg b.w. normal saline (CTRL).
Group 2: DM untreated rats, received 1 mL/kg b.w. normal saline (DM+U).
Group 3: DM rats treated with 600 mg/kg b.w. OPE (DM+OPE).
Group 4: DM rats with EX for 60 min daily (DM+EX).
Group 5: DM rats treated with 600 mg/kg b.w. OPE and EX (60 min/day) (DM+OPE+EX).
Group 6: DM rats treated with 180 mg/kg b.w. MET (DM+MET).
OPE extraction
The sweet orange (Citrus sinensis) was obtained from the citrus farm of the Lower Niger River Basin, Ilorin. The citrus farm is not for commercial purposes but a part of the domestic botanical garden in the institution. The samples collected from the institution were then taken to the University of Ilorin Herbarium, Department of Plant Biology, for identification and Voucher No. UIH0001/159 was obtained. The OPE was extracted according to the method of Adeyemi et al. 16
EX training protocol
Animals in the EX groups were made to run on the modified EX wheel for 60 min/day for 2 weeks of sensitization before induction of T2DM, and they continued the EX after the induction of T2DM for 28 days.
Induction of T2DM
After the acclimatization period, the rats were blindly separated into two groups: the control and the high-fat diet (HFD). The HFD rats were fed with the dietary manipulation (Table 1) for 12 weeks 17 before being injected with streptozocin (STZ). The STZ was preserved in an amber bottle covered with aluminum foil to prevent light interference. A low dose of STZ (35 mg/kg) was dissolved in a citrate buffer (pH 4). It was immediately administered through intraperitoneal (IP) injection into the overnight fasted rats in the HFD group. 18
Composition of High-Fat Diet
The control group also received an equal volume of the vehicle (0.5 mL of citrate buffer) through a similar route. 19 The manipulated feed was continued for 4 weeks while the control rats were placed under the standard chow, and animals with glucose levels >300 mg/dL after 72 h postinduction were considered diabetic for the study.
This model was adopted because a low dose of STZ induces T2DM by targeting the pancreatic β cells but does not induce IR, which is the hallmark of T2DM. 20 Unlike the STZ injection, animals fed with HFD developed IR. 19 Therefore, studies that induce IR by feeding animals with HFD and also disrupt pancreatic β cells through the injection of a low dose of STZ are those that closely mimic T2DM pathogenesis.
Sample collection
Twenty-four hours after the last treatment, the overnight fasted rats (for 12 h) were euthanized through the IP administration of 40 mg/kg of ketamine and 4 mg/kg of xylazine. 21 Blood samples were collected through cardiac puncture into appropriate sample bottles. Blood samples were centrifuged at 3000 rpm (Eppendorf 54115 D) for 5 min to obtain the serum for biochemical analysis. The liver was harvested, and the adhering tissues were removed. The liver was then homogenized and centrifuged at 10,000 rpm (Eppendorf 54115 D) for 10 min at 4°C to obtain the supernatant, which was used for biochemical analysis.
Biochemical assays
Fasting blood sugar
The terminal fasting blood sugar was determined by the glucose oxidase method using a digital glucometer (On Call®Plus ACON Laboratories, Inc., San Diego, CA, USA).
Serum insulin
Serum insulin level was estimated by the enzyme-linked immunosorbent assay (ELISA) technique based on the manufacturer's guideline (RayBio®, GA, USA). The estimation was based on the direct sandwich technique in which two monoclonal antibodies are directed against separate antigenic determinants on the insulin molecule. The reaction was read spectrophotometrically at 450 nm.
Insulin sensitivity and pancreatic β cell
Insulin sensitivity and pancreatic β cell function were estimated using homeostasis model assessment (HOMA), qualitative insulin check index (QUICKI), and triglyceride–glucose ratio (TyG index). 22,23
Homeostasis model assessment of β cell function (HOMA-β) = 20 × fasting blood insulin level (μU/mL)/fasting blood glucose (mmol/L) −3.5.
Homeostasis model assessment of insulin sensitivity (HOMA-S) = [1/HOMA-IR] × 100%.
Homeostasis model assessment of insulin resistance (HOMA-IR) = Fasting glucose concentration (mmol/L) × fasting blood insulin concentration (μU/mL)/22.5.
QUICKI = (1/[log (fasting insulin level) + log (fasting glucose level)]).
TyG index = In [fasting triglyceride (mg/dL) × fasting glucose (mg/dL)]/2.
Hepatic glycogen concentration and GLUT 4 expression
Hepatic glycogen content was determined using a colorimetry method according to the manufacturer's guidelines (Abcam, MA, USA), whereas GLUT 4 (Elabscience, USA) activities were determined using the ELISA method.
Lipid profile
Total cholesterol (TC), triglyceride (TG), and high-density lipoprotein cholesterol (HDL-c) levels were determined using a colorimetry method based on the manufacturer's guidelines (Agappe diagnostic kit, Switzerland). TC/HDL and TG/HDL were calculated as the markers of atherogenic dyslipidemia. 23
Hepatic injury markers
Hepatic lactate dehydrogenase (LDH) and hepatic alanine aminotransferase (ALT) (Aggape Diagnostic, Switzerland) were assayed by a spectrophotometric method using ELISA kits.
Oxidative stress and inflammatory markers
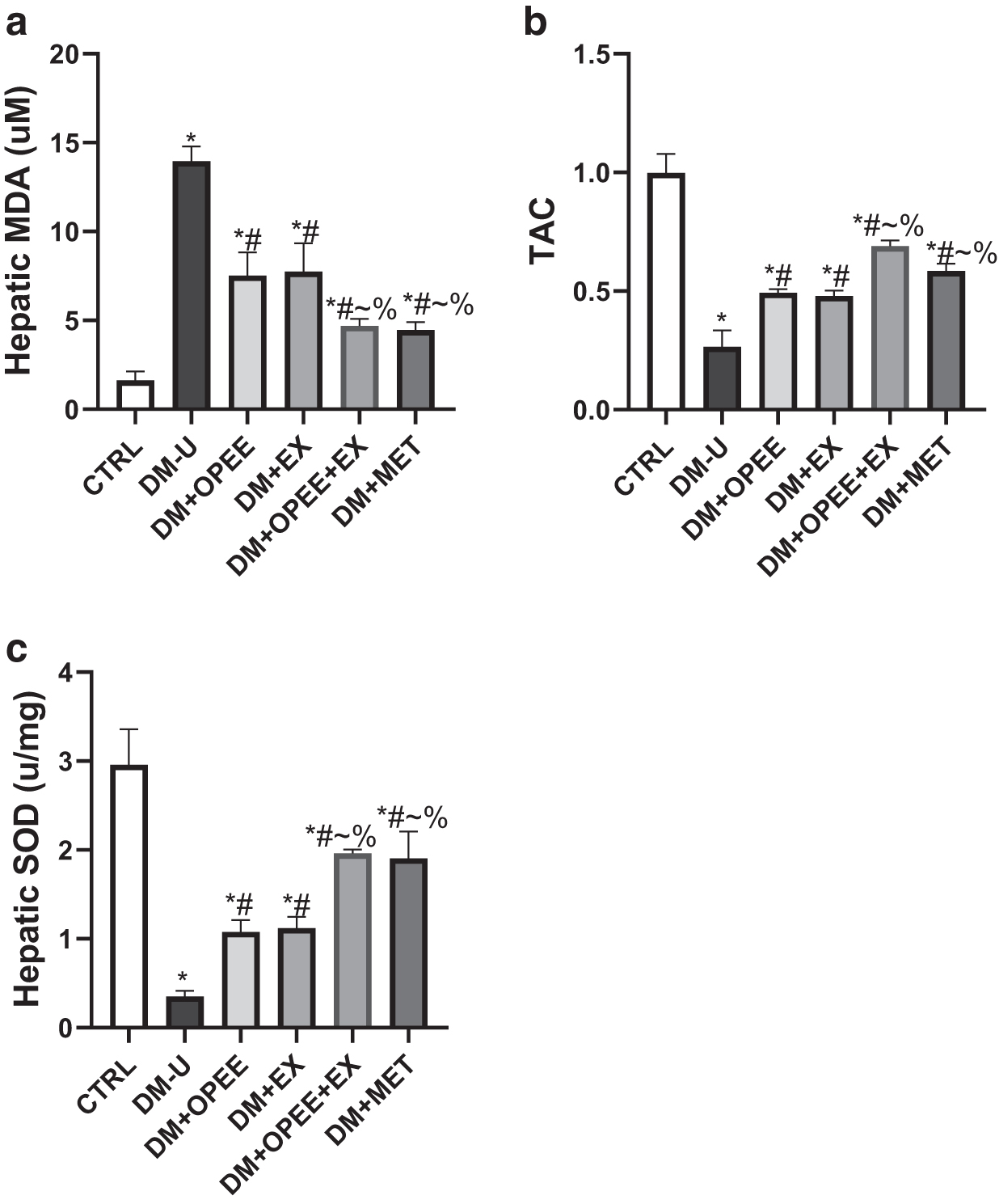
Hepatic malondialdehyde (MDA) was determined as previously documented, 24 whereas superoxide dismutase (SOD) was estimated according to the method of Afolabi et al. 25 and Hamed et al. 23 The total antioxidant capacity (TAC) that provides more accurate information about the antioxidant status of a biological system than those obtained from their individual components 26 was assayed using a colorimetry method (Fortress Diagnostic kit, Switzerland).
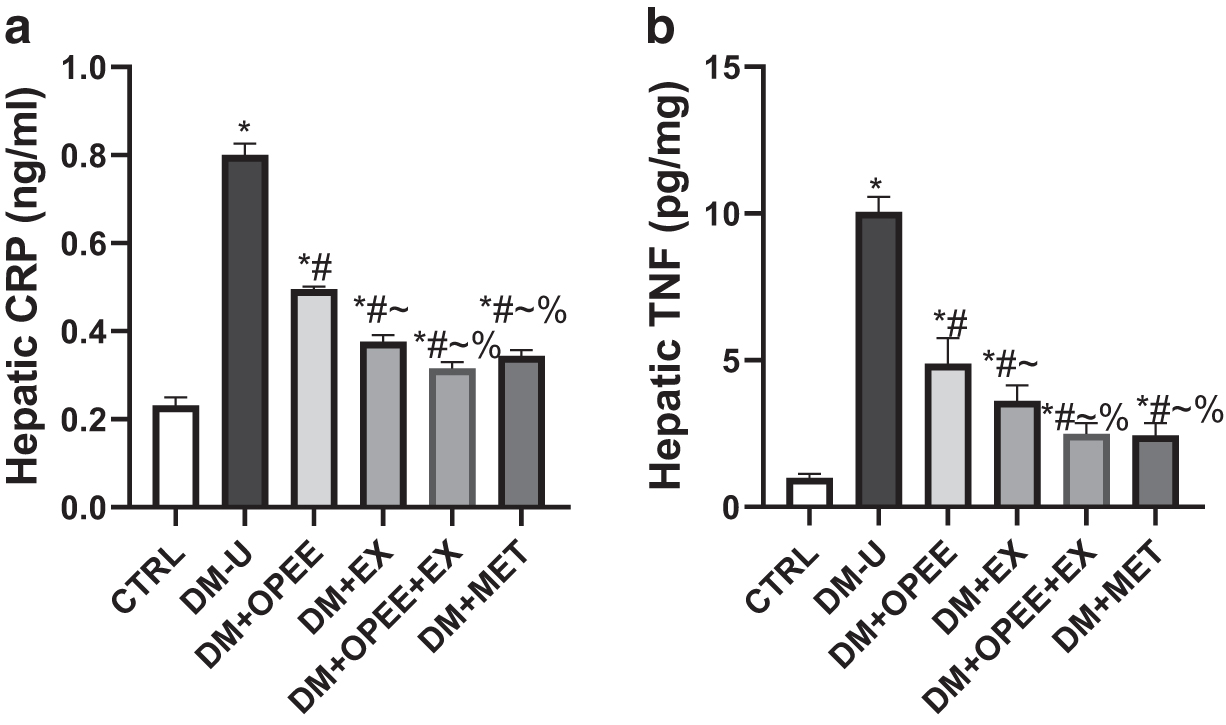
Hepatic tumor necrotic factor-alpha (TNF-α) (Solarbio, China) and C-reactive protein (CRP) (Elabscience, USA) were assayed using an ELISA kit.
Statistical analysis
GraphPad PRISM 5 software (GraphPad Software, La Jolla, CA, USA) was used in carrying out the statistical analysis with a one-way analysis of variance (ANOVA) and Tukey's posthoc test. Data were reported as mean ± standard deviation. Values of P < .05 were considered statistically significant
RESULTS
Effect of OPE and EX on glucose homeostasis
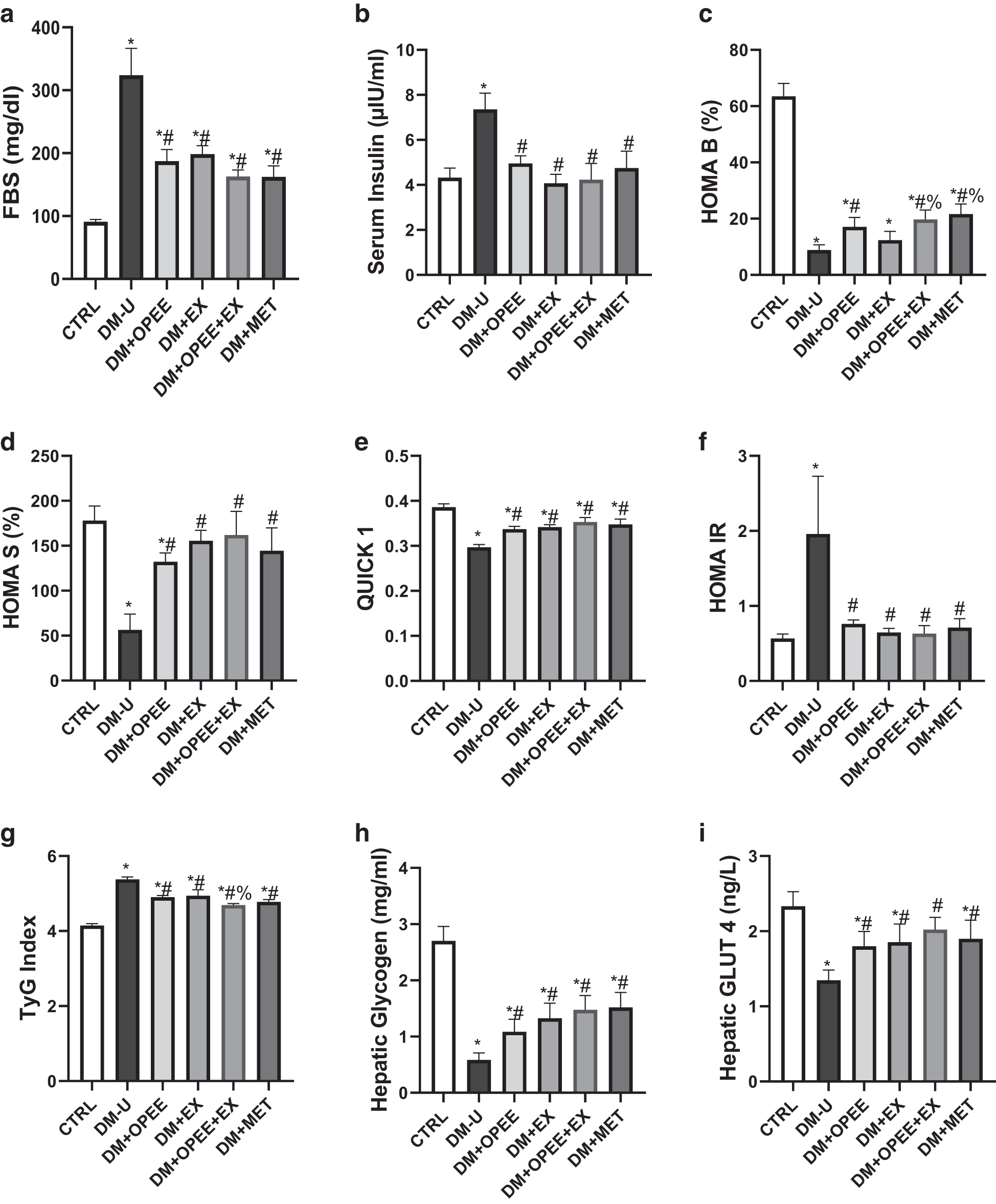
OPE and EX significantly ameliorated the diabetic-induced increase in terminal fasting blood sugar (Fig. 1a) and decreased serum insulin (Fig. 1b). The observed ameliorative effect was noticed across all the DM-treated groups. Furthermore, OPE significantly improved pancreatic β cell function by significantly increasing DM-induced reduction in HOMA-β, whereas EX did not significantly alter pancreatic β cell function. Although OPE increased HOMA-β, a combination of OPE and EX showed a better ameliorative effect than when administered singly (Fig. 1c).
Effect of orange peel extract and physical exercise on
In fact, the result of this study showed that the combination of OPE and EX has the same ameliorative effect on the DM-induced decrease in HOMA-β with MET, a known antidiabetic drug. In addition, OPE, EX, and a combination of both improved insulin sensitivity in DM rats, evident by the significant increase in HOMA-S (Fig. 1d) and QUICKI (Fig. 1e). Also, OPE, EX, and their combination improved insulin sensitivity by significantly decreasing HOMA-IR (Fig. 1f) and TyG index (Fig. 1g).
Furthermore, OPE and EX and a combination of both ameliorated the diabetic-induced decrease in hepatic glycogen content and GLUT4 expression (Fig. 1h, i).
Effect of OPE and EX on lipid profile
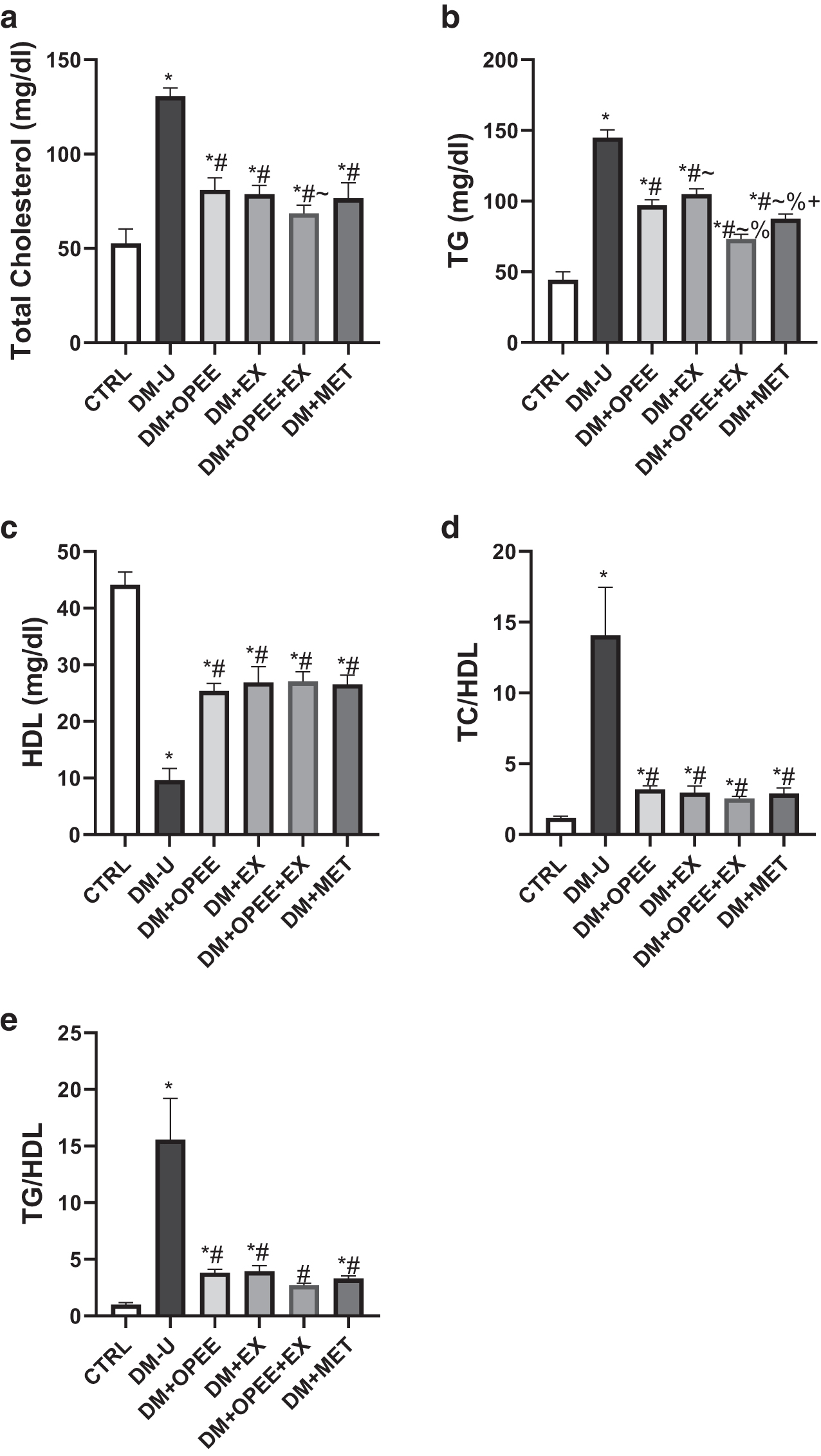
DM induction significantly elevated TC and TG in the serum and decreased serum HDL compared with the control. In contrast, OPE and EX ameliorated the observed DM-induced elevated TC and TG and DM-induced decline in HDL (Fig. 2a–c). Although OPE and EX individually ameliorated DM-induced dyslipidemia, the observed ameliorative effect was more exhibited in rats that received both OPE and EX. Furthermore, the observed DM-induced increase in atherogenic indices evidenced by the increase in TC/HDL and TG/HDL ratios was abolished by treatment with OPE and EX (Fig. 2d, e). The combination of OPE and EX was more effective in ameliorating the DM-induced increase in atherogenic indices.
Effect of orange peel extract and physical exercise on
OPE and EX improved hepatic dysfunction in DM-induced rats
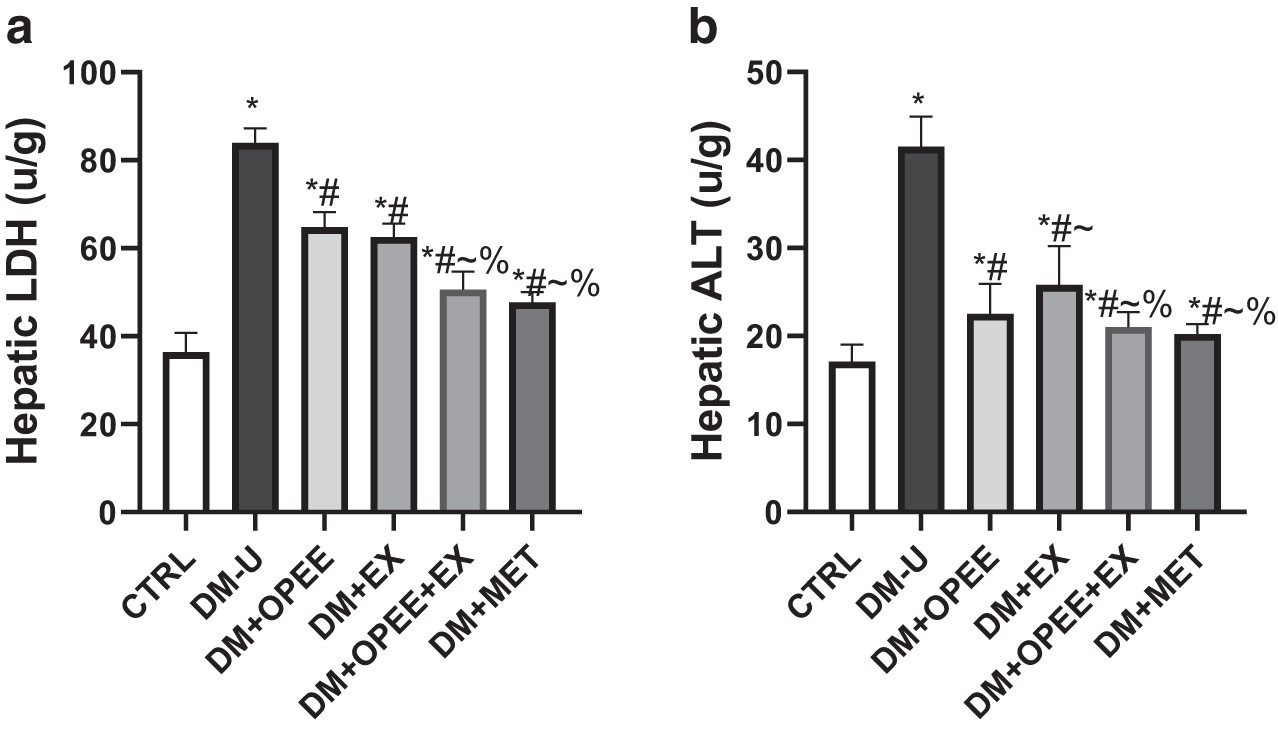
DM impaired hepatic functions as indicated by an increase in LDH and ALT, which are markers of hepatic injury (Fig. 3a, b). The administration of OPE and EX blunted these observed increases in hepatic injury markers. Although animals treated with only OPE and EX exhibited improved hepatic functions, those treated with the combination of OPE and EX displayed improved hepatic function when compared with their counterparts treated with either OPE or EX.
Effect of orange peel extract and physical exercise on
OPE and EX restore DM-induced oxidative stress and inflammatory markers.
Hepatic MDA concentrations were increased in DM-untreated animals when compared with the control. Furthermore, there was a significant decrease in TAC and SOD of animals in the DM untreated group (Fig. 4a–c). These observed differences were ameliorated by OPE and EX. However, combining OPE and EX is more potent in protecting the animals against DM-induced oxidative stress.
Effect of orange peel extract and physical exercise on
Furthermore, the DM-induced inflammatory response evidenced by the significant increase in CRP and TNF-α was ameliorated by administering OPE and EX (Fig. 5). However, the animals treated with the combination of OPE and EX exhibited better ameliorative effect than their counterparts treated with either of the two.
Effect of orange peel extract and physical exercise on
DISCUSSION
This study shows that OPE and EX synergistically improve glucose homeostasis and atherogenic lipids coupled with the upregulation of GLUT4 activities. IR is gradually becoming a global public health challenge, 5 with an increased risk of T2DM. 27 Patients with IR have been shown to exhibit hyperglycemia, lipid dysmetabolism, and reduced GLUT4 concentration, whereas OPE was considered a waste product, has now been shown to possess antihyperglycemic properties. 28 Also, EX has been recommended for individuals with T2DM, and it has been speculated to maintain glucose homeostasis. 29 Hence, the synergistic effect of OPE and EX on DM-induced glucose dyshomeostasis, hepatic lipid accumulation, and the oxide-inflammatory response was explored.
Fasting blood glucose and insulin are important diagnostic and prognostic tools in glucose dysmetabolism, which are essential features of T2DM. 23 IR markers such as HOMA-β, HOMA-S, HOMA-IR, and Tyg index also predict T2DM. In consonance with the findings of Ahmed et al. 28 and Reddy et al., 29 this study agrees that OPE and EX can individually ameliorate DM-induced glucose deregulation as depicted by reduced FBG, elevated serum insulin, improved β cell dysfunction, and IR. However, the findings from this study showed that the combination of OPE and EX synergistically restored glucose homeostasis and improved pancreatic β cell functions.
The insulin-sensitive GLUT4 is mainly expressed in insulin-sensitive organs such as the liver, 30 which is responsible for insulin-induced glucose uptake. Once insulin binds with its receptor, it activates exquisite intracellular sorting of signals, leading to the translocation of GLUT4, which enhances glucose influx and glycogen replenishment. 31 The findings from this study that OPE and EX ameliorated DM-induced downregulation of GLUT4 and depletion of glycogen content agreed with those of the study by Ahmed et al. 28 and Richter and Hargreaves, 32 respectively.
The observed ameliorative effect of OPE and EX on DM-induced glucose deregulation could be through insulin-induced GLUT4-dependent mechanism or phosphatidylinositol 3-kinase (PI3K)/protein kinase B (Akt) signaling. Insulin-induced GLUT4 translocation and glucose uptake through insulin receptor substrate (IRS) may be impaired by the activation of the serine/threonine kinase cascade that triggers serine phosphorylation of IRS, which in turn impairs tyrosine phosphorylation, resulting in IR through PI3K/Akt signaling. 33
OPE and EX also ameliorated DM-induced hepatic lipid accumulation and elevated TC/HDL and TG/HDL, an indicator of energy imbalance and IR-associated dyslipidemia. These findings agreed with the study of Pineda-Lozano et al. 34 and Wang and Xu, 35 which reported a similar effect. Thus, OPE and EX-enhanced insulin sensitivity and glucolipid regulation, accompanied by improved atherogenic dyslipidemia, explain the enhanced pancreatic β cell function that was observed in this study. Furthermore, excessive TG accumulation has been established to be associated with IR and hepatic injury.
The presence of IR and increased TG promotes T2DM and other metabolic disorders. 23 The accumulation of TG in this study probably promotes the formation of toxic metabolites such as diacylglycerol and ceramides, which can lead to inflammatory response, oxidative stress, and hepatic injury.
Furthermore, OPE and EX ameliorate DM-induced hepatic injury by suppressing the activities of LDH and ALT, which could be because of their ability to prevent the formation of toxic metabolites that could damage the liver. Findings from this study corroborate those of AbdEl-Gwaad et al. 36 and Cannata et al., 37 which reported a similar result.
Oxidative stress, which is majorly caused by reactive oxygen species (ROS), contributes to the pathogenesis of IR and metabolic disorders. Although ROS at the physiological level is required for homeostatic function, signaling processes, and defense mechanisms, 38 they lead to oxidative stress once they are generated in excess. 39 DM-induced exacerbated ROS generation, and the subsequent suppression of antioxidant defense mechanisms can disrupt the cellular organelles and enzymatic activities, increase lipid peroxidation, and develop IR. 40 This deleterious effect of oxidative stress can lead to the development and progress of T2DM complications.
The observed ameliorative effect of OPE and EX on the DM-induced increase in pro-oxidant (MDA) and antioxidants (TAC and SOD) agreed with the study of Selmi et al. 41 and Atalay and Laaksonen 42 that reported an increase in antioxidant activities after treatment with OPE and EX, respectively. DM leads to the excessive generation of ROS through glucose oxidation and nonenzymatic protein glycation. 43
Inflammation is a homeostasis process by which the immune system identifies and removes harmful stimuli and begins healing. 44 Acute inflammation is required for various physiological activities, whereas chronic inflammation has been implicated in the pathogenesis of multiple disorders, including T2DM. 45 IR is linked with chronic inflammation through the release of inflammatory cytokines such as TNF-α, interleukin (IL)-1β, and IL-6, and a decline in the production of anti-inflammatory cytokine (IL-10). Also, other inflammatory factors, such as CRP, have been associated with IR. 45 The findings that OPE and EX ameliorated DM-induced elevated TNF-α and CRP concurred with the study of Hamed et al. 23 and Chen et al. 46
In conclusion, this study clearly demonstrates that OPE and EX synergistically improve DM-induced dysmetabolism and insulin sensitivity associated with enhanced pancreatic β cell function and improved atherogenic dyslipidemia through oxidative-sensitive signaling, coupled with upregulation of GLUT4. It is crucial to monitor fasting blood sugar during the treatment with OPE and EX to avoid hypoglycemia.
FUTURE PERSPECTIVES
Possible areas to look into for future research are to assess the long-term effects of the combined intervention on glucose metabolism and overall metabolic health in rats with T2DM; conduct a longitudinal study to evaluate the sustainability of the observed improvements and to monitor any potential side effects or adverse outcomes associated with prolonged treatment; also, translate the findings from animal models to human clinical trials; and conduct randomized controlled trials in individuals with T2DM to investigate the efficacy and safety of OPE supplementation in combination with structured physical EX.
Footnotes
AUTHORs' CONTRIBUTIONS
L.A.O, K.B.O. and A.F.O. conceived and designed the study. L.A.O., K.B.O., D.J.J., A.J.A., and A.F.O. carried out the experiments. L.A.O., K.B.O, J.D.J., A.J.A., and A.F.O. contributed reagents and analytical kits. A.F.O. analyzed and interpreted data. L.A.O. and A.F.O. drafted the article. L.A.O., K.B.O., J.D.J., A.J.A., and A.F.O. read and approved the final article.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.