
Abstract
After consumption, probiotics provide health benefits to the host. Probiotics and their metabolites have therapeutic and nutritional properties that help to alleviate gastrointestinal, neurological, and cardiovascular problems. Probiotics strengthen host immunity through various mechanisms, including improved gut barrier function, receptor site blocking, competitive exclusion of pathogens, and the production of bioactive molecules. Emerging evidence suggests that intestinal bowel diseases can be fatal, but regular probiotic consumption can alleviate disease symptoms. The use and detailed description of the health benefits of probiotics to consumers in terms of reducing intestinal infection, inflammation, and digestive disorders are discussed in this review. The well-designed and controlled studies that examined the use of probiotics to reduce life-threatening activities caused by intestinal bowel diseases are also covered. This review discussed the active principles and potency of probiotics as evidenced by the known effects on host health, in addition to providing information on the mechanism of action.
Introduction
Pas live microbes that provide beneficial health attributes to the host by activating the immune system, maintaining host homeostasis, and enabling protection from microbial infections. This is based on an original definition of probiotics as “A live microbial feed supplement, which beneficially affects the host animal by improving its intestinal balance.” 1 Later, the term was further redefined as “live microorganisms, when consumed in adequate amounts, confer a health effect on the host.” 2 Normal bacteria associated with humans are naturally involved in a symbiotic relationship.
Bacteria start colonizing the gastrointestinal tract (GIT) right at birth and keep growing over a life period but are accompanied by substantial age-specific alterations. 3 Gram-positive bacteria such as Bifidobacterium and Lactobacillus species-specific strains act as potent probiotics and have provided prominent, useful effects in diseases such as diabetes, liver diseases, obesity, cardiovascular diseases, diarrhea, cancer, inflammatory bowel disease (IBDs), and syndrome (IBS). 4
Probiotics are used to provide health benefits against different disorders, including digestive issues such as diarrhea, constipation, and IBS. Probiotics and prebiotics from functional foods may have beneficial effects, including activation of the immune system, modulation of the digestive system, neutralization of toxins, and preventing the attachment of pathogens to the intestinal epithelial cell membrane.
Probiotics transmit signals to the goblet cells to enhance mucus secretion in the intestine, acting as a barrier against infections by undesirable microbes and mitigate oxidative stress induced gut dysfunction. 5,6 The probiotic strain Bifidobacterium lactis proved effective in protecting bone biomass and ameliorating tissue damage by strengthening the intestinal barrier and reducing inflammatory cytokines in the ulcerative colitis (UC) mice model. 7
Probiotics of fermented foods origin provide a wide range of beneficial health effects to the host, but such microorganisms must be tolerant to bile and gastric acid, adhere to the intestinal epithelial cell, produce anti-microbial compounds, and exhibit the property of competitive growth and multiplication-based exclusion of pathogens. Potential probiotics are identified using DNA/DNA hybridization and 16S RNA sequencing.
Genomics and proteomics are being used to define the molecular mechanisms of probiotics to assess their pre-clinical safety and enhanced delivery. 8,9 The comprehensive study was primarily done to review the possible beneficial properties of probiotics through which they help to alleviate the gut disorders caused by pathogens. So, this study could provide new insights and possible mechanisms that may be useful for researchers working in a gut health area.
Inflammatory Bowel Diseases
IBDs are a constant problem; over 6.8 million people are affected globally. 10 IBDs include UC, intermediate colitis, pouchitis, Crohn's disease (CD), and chronic inflammatory disorders occurring in the GIT due to microbial dysbiosis. Therefore, modulation of intestinal microbiota could significantly reduce inflammation in the experimental model of UC. 11
For example, regular consumption of Bifidobacterium infantis significantly prevented colonic inflammation and mucosal damage while modulating the goblet cells. Probiotics have displayed their efficiency against IBD in two ways: either by modulating the action of anti-inflammatory cytokine and strengthening the gut barrier or by altering the mucosal immune responses to bacterial antigens in the lumen.
Probiotics positively impact gut microbial homeostasis 12 and restore normal microbiota by interfering with microbial dysbiosis. For example, besides preserving the mucus depleted goblet cells and thickening of muscularis externa, accompanied by insignificant submucosal oedema, there was diminished crypt abscess in B. infantis fed animals. 11
The impact of two Lactobacillus reuteri (rat-derived R2LC and human-derived ATCC PTA 4659 strains) against dextran sodium sulfate induced colitis in the mice model has also been reported. 13 Both Lactobacillus strains significantly reduced the severity of colitis. A significant reduction in the levels of inflammatory cytokines/chemokines such as IL6, IL1β, myeloperoxidase, and mouse keratinocyte chemoattractant was achieved after feeding with L. reuteri.
This bacterium also increased the adherent mucus layer's thickness in control and dextran sodium sulfate treated mice. Similarly, probiotics have been reported to enhance the expression of occludin and zonula occludens-1 proteins of the tight junction in colonic crypts. 13 Further, the use of B. lactis BL-99 leads to substantial reductions in levels of major proinflammatory cytokines such as TNF-α and IL-17. Moreover, consumption of probiotic strain leads to enhanced expression of Claudin-1, MUC2, ZO-1, and Occludin, in addition to an overall reduction in osteoporosis, reflected as substantial improvements in bone volume and thickness of trabecular bone tissue. 14
Oral administration of probiotics supported increased trans-epithelial resistance and modulated fecal bacterial load in people undergoing surgical procedures. The percentage abundance of Bifidobacteria and Lactobacilli increased, whereas Enterobacteriaceae and Pseudomonas decreased. Denaturing gradient gel electrophoresis analysis of 16S rRNA showed diverse bacterial load in the probiotics fed group. 15 Colectomy is the surgical procedure to remove a part of the colon or entire colon that becomes severely damaged due to IBDs such as UC or CD, mechanical bowel obstruction, and conditions such as colic ischemia or colic injury, etc.
An experimental rat model study observed that after colectomy, the composition of mucosa-associated microbiota shifted with an increase in the concentration of pathogens such as Shigella spp., Enterococcus, and Escherichia spp. 16 Researchers have concluded that probiotics might positively affect the recuperation of bowel action in these patients.
However, some researchers have shown in a study that preoperative consumption of probiotic capsule (containing a mixture of strains such as Lactobacillus acidophilus, Lactobacillus plantarum, Lactobacillus casei, Streptococcus thermophilus, Bifidobacterium longum, and Bifidobacterium breve) before colorectal surgery did not correlate with mortality or reduction of complications that appeared after the colorectal surgery. 17
Currently, there is insufficient evidence for the role of probiotics in treating CD or UC when compared with standard treatment therapies (drugs) for human IBDs. Experiments on murine and rat models using probiotic strains have been carried out over a few decades. Dextran sulfate sodium (DSS) and 2,4,6-trinitrobenzene sulfonic acid (TNBS) have been used widely in experimental animal model colitis. DSS is a chemical compound with anticoagulant properties used most often to induce colitis in a mouse model.
The DSS-induced model most typically imitates the human UC. Estimation of B. infantis BB-02 effect on DSS-induced UC in BALB/c mice model showed decreased clinical signs and symptoms of the disease. The histopathological analysis showed a reduction in edema in the gut with decreased mucin production. However, DSS administration resulted in a damaged area in the distal part of the colon, anomalous cellular function, adhesion of muscle layers, and the appearance of acute inflammation in the induced colitis animal model.
Administration of probiotics lowered intestinal permeability and improved intestinal barrier integrity. sIgA acts as a barrier against the adherence of pathogens to the mucosal layer of the intestine. In DSS-induced colitis, sIgA production increased as a protective response against increased intestinal permeability; however, lowered expression of sIgA was observed in the presence of B. infantis probiotic strain. Reduced colon inflammation appeared due to a decrease in the activities of neutrophils along with KC/CXCL-1 level when B. infantis BB-02 was administered in DSS-induced colitis mice. 18
Another study on DSS-induced animal colitis, when administered with Lactobacillus delbrueckii, showed an anti-inflammatory effect in the model and moderate innate immune responses by modulating the nuclear factor kappa B (NF-κB) activation in the intestinal epithelial cells. 19 TNBS is a hapten that acts as an antigen on binding to tissue protein and leads to induced immunologic responses.
Ethanol breaks the mucosal barrier and creates a passage for TNBS to enter the mucosal layer of the intestine and induce colitis in animals. In a study of the TNBS-induced colitis rat model, administration of L. plantarum 21 (LAB 21) and sulfasalazine drug showed antioxidative and immunomodulation properties by increasing the concentration of reduced glutathione and reducing nitric oxide and rate of lipid peroxidation.
LAB 21 also significantly decreased mRNA and protein levels of IL-1β and TNF-α while upregulating the protein expression level of anti-inflammatory cytokine IL-10 in TNBS induced colitis rats. 20 Another study on TNBS-induced colitis in CD-1 mice showed alteration in gut microflora 3 days after injecting 1.5 mg/mouse in 50% ethanol intrarectally. TNBS administration caused colonic inflammation, and clinical signs appeared in the CD-1 mice.
The microbiological result showed susceptibility to both ethanol and TNBS treatments and increased Clostridium and Escherichia coli species with reductions in Lactobacillus and Bifidobacterium strains. 21 UC is restricted to the epithelial linings of GIT and is characterized by inflammation in the large intestinal descending colon and rectal part. UC patients suffer from pain in various locations of the lower abdominal area.
Diarrhea, weight loss, and blood discharge from the rectum are some of the signs and symptoms of UC. 22 Alternative remedies are preferred in IBD patients due to increased risks in clinical efficacies. 10,23 Children could suffer extensively from IBDs during early life that involves the initial establishment of gut microflora and the development of the immune system. 23,24 Another recent study showed the protective effects of a combination of probiotics and symbiotics from fermented tea leaves.
The combination proved beneficial in retaining body weight and maintaining colon length. The treatment leads to reduced edema and crypt distortion, thereby maintaining the structural integrity by altering tight junctions to varying degrees. The combination of probiotics and symbiotics significantly reduced the level of TNF-α and IL-6, whereas IL-10 was upregulated, thus attenuating the systemic inflammation in the DSS-induced colitis model and proved to be significant therapy. 25
Protective effects of probiotics and tea leaves symbiotic were also observed in DSS-induced colitis. The combination proved beneficial in retaining body weight and maintaining colon length. The treatment reduced edema and crypt distortion, thereby maintaining structural integrity by altering tight junctions to varying degrees, and proved to be significant therapy against inflammatory colitis. 25
Genetic Association with Different Forms of IBDS
Impact of NOD2 on intestinal health
Different forms of IBD are diagnosed based on histopathological and clinical data, though many genetic variants are also found to be associated with different forms of IBD. Nucleotide oligomerization domain containing 2 (NOD2) gene belongs to the nucleotide oligomerization domain-like receptor (NLR) family, which is located on chromosome 1626 and has shown a genetic association with IBD. NOD2 is highly expressed in macrophages and dendritic cells but the expression of NOD2 is quite low in T cells. 22
NOD2 is also known to be expressed by ileal Paneth cells, intestinal stem cells, epithelial enterocytes, and goblet cells. 27 Because of the presence of conserved sequence N-acetylmuramyl-L-alanyl-D-isoglutamine in both Gram-positive and Gram-negative bacterial peptidoglycan layers, NOD2 can detect a wide variety of bacteria. 28 NOD2 can recognize muramyl dipeptide that is derived from the peptidoglycan found in Gram-positive bacteria to a greater extent than in Gram-negative bacteria. 26
NOD2 shows high susceptibility to CD, highlighting its importance in the innate immune response in IBD pathology. NOD2 mutations in CD play an important role in regulating bacterial flora by secreting NOD2 protein, an intestinal anti-microbial peptide such as cryptdins. 29 In mice, NOD2 acts as an essential regulator of ileal commensal microbiota by controlling the secretion and expression of anti-microbial peptides. 28
NOD2-deficient mice showed decreased bactericidal activity, enhanced commensal bacterial load, and more propensity to colonization by harmful bacteria in addition to increased susceptibility to intestinal inflammation and bacterial infections. 26 Thus, NOD2 regulates pivotal functions in the relationship between commensal bacteria and the host immune system. Impaired immunity has been observed in NOD2 –/– mice because of the defective cytokines produced by the dendritic cells that provided susceptibility to Bacteroides vulgatus. 30
Inflammatory gene expression and goblet cell dysfunction associated with increased IFN-γ production by intraepithelial activities are some of the serious abnormalities occurring in the small intestine of NOD2 –/– mice. And all these abnormalities intensify when there occurs a microbial expansion of Bacteroides vulgatus in the small intestine of the NOD2 –/– mice.
Thus, NOD2 plays an efficient role in averting inflammation by limiting pathological expansion and supporting gene-microbe interactions. 31 Another study revealed that NOD2 mutation does not increase the risk of UC but increases the rate of colectomy and intravenous-steroid refractoriness. 32
Autophagy-related genes and their association with IBDs
Another gene called autophagy-related 16 like-1 (ATG16L1) shows a strong association with CD. Autophagy is a critical process known to degrade proteins and membrane lipids into their simplest forms of amino acids and free fatty acids, which are then required to carry out essential metabolic processes such as ATP production, protein synthesis, etc.
Several reports have identified single-nucleotide polymorphisms linked to CD pathogenicity. ATG16L1 is an adaptor protein with three alternative splicing isoforms, which are α, β, and γ, and comprises ATG5-binding region on the N terminal, coil–coil domain followed by a seven-tryptophan aspartic acid (WD) repeat domain. 33 In a previous study, it was observed that the presence of ATG16L1 along with ATG5 autophagy protein are important for maintaining the coherence of the Paneth cell that functions by secreting granule contents comprising anti-microbial peptides and other proteins to protect the intestinal stem cells and prevent notable abnormalities in granule exocytosis process. 34
ATG16L1 T300A mutated gene has been known to increase the risk of CD. In a study conducted with risk allele ATG16L1 T300A, there was increased dysbiosis in the mutated mice, specifically with an increase in Bacteroides ovatus, and also increased Th1 and Th17 immune cell response, which induced a change in inflammatory cell response and microbiota in the gut. 35 Another study showed that during ileal inflammation, CD patients homozygous for ATG16L1 risk allele were not able to clear pathosymbionts to a sufficient extent, and the presence of Fusobacteriaceae was found in increased numbers.
Also, CD patients homozygous for ATG16L1 protective allele had reduced numbers of Enterobacteriaceae, Bacteroidaceae, and relatively more numbers of Lachnospiraceae than patients who carried the risk allele. However, it was observed that the ATG16L1 allele hardly affected the bacterial composition in the non-inflammation region of the ileum. 36 Autophagy-related protein (ATF4) was found to reduce significantly in the inflamed intestinal mucosa of a patient with active UC. 37 A comprehensive detail regarding probiotics attributes for regulating intestinal infections and digestive disorders has been compiled in Table 1.
Summary of Probiotics Attributes and Their Ability to Regulate Intestinal Infections and Digestive Disorders
CFU, colony forming units; DSS, dextran sodium sulfate; IBS, irritable bowel syndrome; IBS-D, irritable bowel syndrome-diarrhea; MLNs, mesenteric lymph nodes; TNBS, 2,4,6-trinitrobenzene sulfonic acid.
Vitamin D network and its impact
Patients suffering from UC were found to have low vitamin D receptor (VDR) expression levels, in addition to deregulated Vitamin D signaling. 38 VDR may downregulate intestinal inflammation by induction of autophagy-mediated inflammasome. 39 However, during intestinal inflammation, it has been observed that adherent-invasive E. coli adhere to epithelial cells of the intestine and dodge autophagy clearance by getting swallowed inside the macrophages. 40
In DSS-induced UC models, the contribution of autophagy in maintaining and restoring gut microbiota homeostasis was observed. The use of galangin flavonoid not only increased gut microbial diversity but also enhanced the level of short-chain fatty acid, with increased Butyricimonas spp and progressive recovery of Lactobacillus spp, thus leading to UC prevention. 41 All these studies revealed that autophagy-related studies are advantageous in the treatment of UC and CD and demanded further exploration in the future as well.
Probiotics and immunomodulation
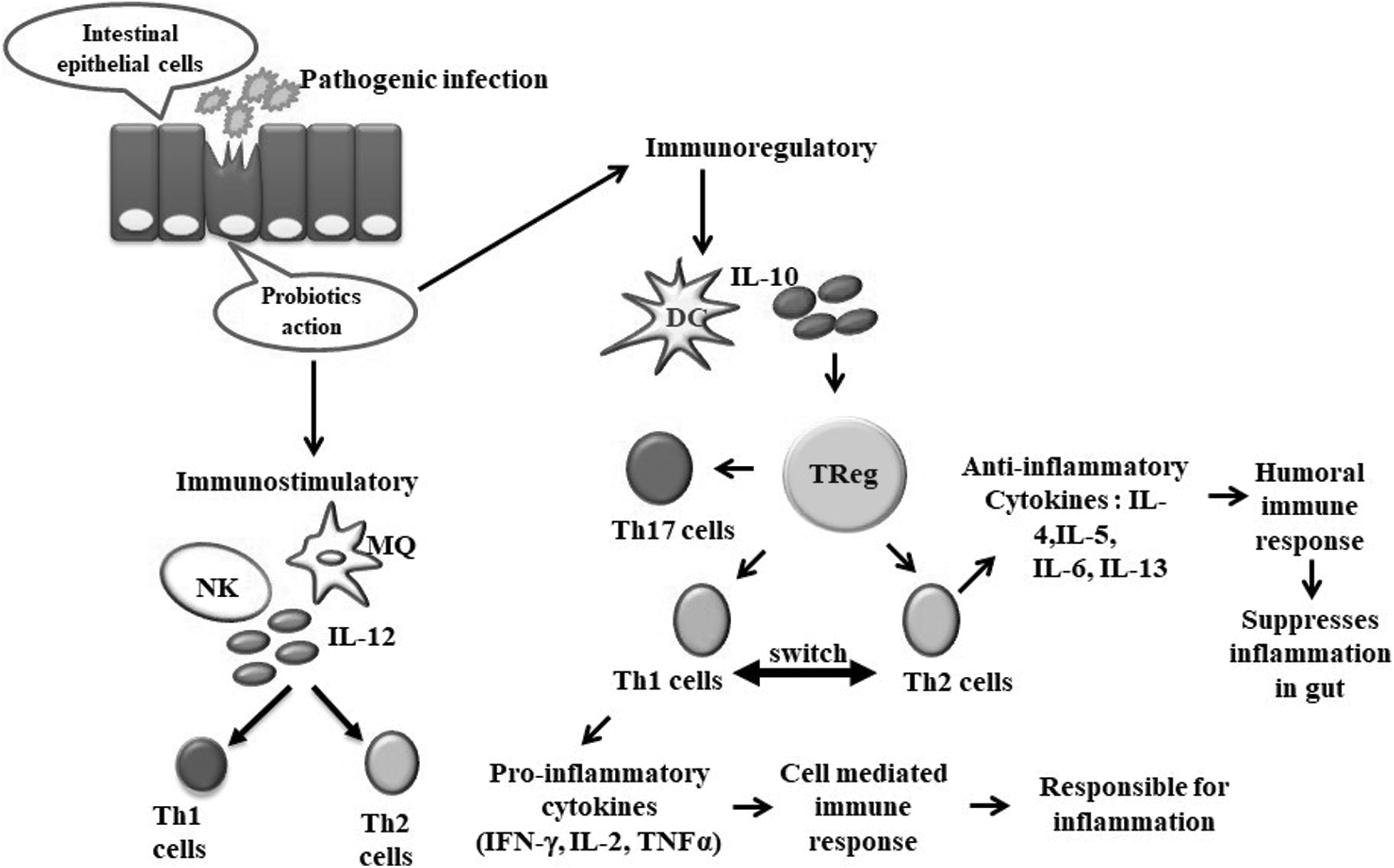
Probiotics modulate immune cell functions and interact with dendritic cells, T helper cells, and Treg cells that can regulate the effect of pro- and anti-inflammatory cytokines. Probiotics may trigger either immune-stimulatory or regulatory responses. Immunostimulatory probiotics mainly act against infections, cancers, and allergies, whereas immunoregulatory probiotics are associated with the production of IL-10 and the induction of Treg cells. 4 The pathways followed in IBDs show heterogeneous effects on activation.
There are IBD-associated alterations, including intestinal barrier maintenance function, autophagy pathway, innate immune response, microbiota population, epithelial restitution, reactive oxygen species, and the balance of Th17 and Treg cells. The autophagy pathway in epithelial cells mainly causes bacterial clearance, but when executed in macrophages, the same pathway secretes IL-1β. 42,43 IL-1β may stimulate the secretion of IL-17 and IL-22 to induce chronic inflammation of the gut. 42,44 JAK2, STAT3, TNFSF15, and TYK2 influence the IL-23 signaling that can impact IBD by reducing GIT inflammation. 45
Another protective effect of probiotics was reported in Citrobacter rodentium induced colitis. A probiotics consortium that included L. acidophilus, Lactobacillus rhamnosus, and L. plantarum A, stimulated the production of CD11c+ dendritic cells in the spleen and mesenteric lymph nodes in a CD patient. The probiotics upregulated the CD-associated CD4+ CD25+ Foxp3+ regulatory T cells in mesenteric lymph nodes via downregulation of inflammatory cytokines IL-17, TNF-α, and IFN-γ, 46 thus supporting the immunomodulatory ability of probiotics in regulating IBD inflammation.
The important lymphocytes that participate in proliferation in IBD are mainly Th cell lineage like helper T cells (Th1, Th2, Th17) and Treg cells (Type 1 regulatory cells, or Tr1). 22 These cytokines mainly consociate with intracellular bacteria and the killing of viruses. 47 TNF-α plays an important role during inflammation, with elevated levels observed in IBD patients. 22
Increased TNF-α induces the proliferation and differentiation of cells and upregulates the adhesion molecules on endothelial cells. Anti-inflammatory cytokine regulation is mediated by Th2 cells. 47 Among IBD patients, the gut microbiota gets disturbed; reductions in Treg cell and a disbalance between Th17/Treg cell population are observed. 47 The release of TNF-α gets increased in patients with active CD as a result of inflamed ileal mucosa.
However, inflamed ileal mucosa, when incubated with probiotics such as Lactobacillus bulgaricus and L. casei, has been observed to release significantly lower TNF-α levels. 48 The activity of IL-17 is crucial because when it cannot block the helper T cells, the Th1 and Th2 distort effects between Th1/Th17 and Th2/Th17, that is, immune switch. 47 Anti-inflammatory drugs utilized in IBD treatment include 5-aminosalicylic acid, azathioprine, infliximab, methotrexate, adalimumab, natalizumab immunomodulators, etc. Such compounds mainly trigger Th2 response and weaken Th1 influence on inflammation (Fig. 1).

Immune regulation by probiotics: Effect of probiotic action resulted in immune response and regulation of the inflammatory action in the intestinal cells. Th2 cell activity causes secretion of anti-inflammatory cytokines, which enhances its activity and attenuates Th1 influence on inflammation by dampening the pro-inflammatory cytokines, thus preventing Crohn's disease.
Anti-TNF-α antibodies mainly act on the reduction of circulating soluble TNF-α in the body. Infliximab is a drug that mainly neutralizes TNF-α activity by interfering with the TNF-α receptor, thus representing a potential and effective CD treatment. Thalidomide, an immunomodulatory agent, also participates in CD by suppressing inflammatory cytokines in the intestine.
Irritable Bowel Syndrome
Irritable bowel syndrome (IBS), which is classified as a disorder of gut-brain interactions, is one of the most common bowel problems and, on average, afflicts every 10th person in the world. 49 In India, about 15% of the population is said to have IBS. Studies have suggested a potential modulating role for intestinal microflora in IBS. Impaired metabolic activity and irregular gut microbiome composition are common features in IBS patients. 50,51
A double-blind, randomized clinical trial concluded that using the probiotic Clostridium butyricum in patients with diarrhea predominant IBS (IBS-D) improved the overall clinical symptoms while reducing stool frequency. 52 Use of the breast milk-derived probiotic Lactobacillus gasseri BNR17 significantly mitigated IBS-D symptoms in treated patients compared with the placebo group. 52
A randomized controlled trial stated that the use of Saccharomyces cerevisiae resulted from reductions in abdominal pain and discomfort in patients with IBS. 53 In addition, B. infantis 35624 and B. bifidum MIMBb75 were reported to improve abdominal pain, incomplete evacuation, straining, bowel dysfunction, bloating, and gas passage in IBS patients. 54,55 Combinations of different probiotics to check their efficacy against IBS were also studied.
For example, the effect of a probiotic mixture containing B. breve Bb99, L. rhamnosus GG, L. rhamnosus LC705, and Propionibacterium freudenreichii ssp. shermanii JS was studied for 6 months in patients and shown to reduce IBS symptoms such as abdominal pain, flatulence, and distention by up to 42% compared with the control group. 56 A combination of probiotics, B. bifidum CUL20, B. lactis CUL34, L. acidophilus CUL60, and CUL21 also improved IBS symptoms in patients. 57
However, the commercial BIO-25 formulation (11 probiotics) consumed by IBS-D women patients had no superior effect on symptoms compared with the placebo group. 58 Another trial used Bio-Kult® (a mixture of 14 bacteria) in 400 IBS-D patients and concluded that consumption of this mixture led to significant improvements in patients compared with the placebo group. 59 Probiotics mixture VSL#3 consumption by patients with IBS-D also improved abdominal bloating significantly compared with controls after 10 weeks of treatment. 60
It was concluded that melatonin regulation by VSL #3 might be responsible for improved IBS symptoms. 61 Administration of the liquid probiotics mix “Symprove” for 12 weeks was well tolerated by IBD patients and significantly improved disease symptoms. 62 In contrast, the fermented milk-derived Bifidobacterium animalis DN-173 010 creates bloating and discomfort in IBS patients compared withthe control group. 63
Although many positive outcomes in treating and managing IBS were furnished using probiotics, some studies reported no significant improvement in conditions even after using different probiotics. 64 The use of probiotic mixes containing Bifidobacterium Bb12, Lactobacillus paracasei ssp. paracasei F19 and L. acidophilus La5 led to no observable positive effects in patients with IBS compared with controls, even after 6 months of treatment.
Similarly, a combination of six different probiotics containing B. lactis W52, L. acidophilus NCFM, Lactobacillus salivarius W57, L. casei W56, Lactococcus lactis W58, and L. rhamnosus W71 was used to treat a group of patients having IBS with visceral hypersensitivity for 6 weeks. This randomized, double-blind trial concluded that no significant improvement in patient condition was noticed compared with the placebo group. 64
It can be stated that the effect of probiotics in different IBS conditions varies with microbial strain and conditions of the patients. This may be the reason why some probiotics are not consistent in all situations. Such observations strongly warrant more controlled studies with large numbers of participants to conclude how and which probiotics are most beneficial in IBS. Nonetheless, probiotics remain an excellent adjuvant/prophylactic measure in alleviating the myriad of IBS-related complications and serve as an excellent supplement for maintaining a healthy bowel.
Prevention Of Diarrhea
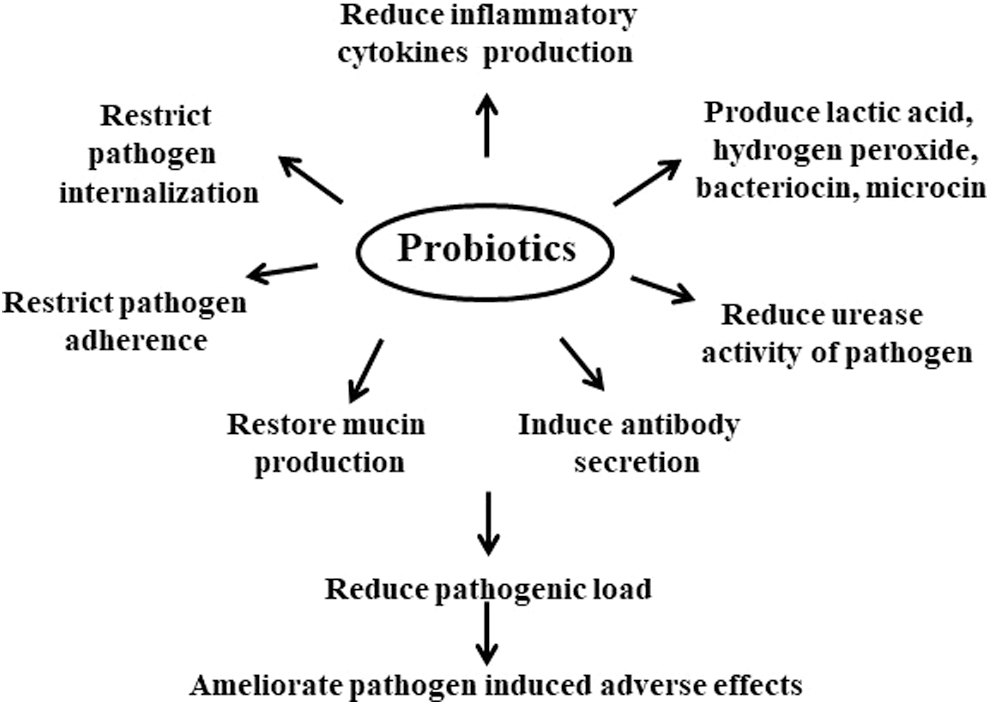
Worldwide, >1.6 million people die from diarrhea each year, 65 and it is the fifth leading cause of mortality in children <5 years, having its harshest impact in developing and underdeveloped countries. 65,66 Diarrhea is caused by the infection of different bacteria (including E. coli and Salmonella spp.), viruses (most notably Rotavirus spp.), and protozoa. During diarrhea, the gut microbiota gets disturbed by the pathogenic attack and results in intestinal dysbiosis characterized by frequent watery stools, abdominal pain, severe dehydration, blood/mucus in stool, etc., which in serious cases may lead to fatality. 67 Probiotics have shown the potential to restore normal gut microbiota and curb intestinal disturbances, including diarrhea (Fig. 2).
Probiotics exert various effects on or by host cells in the production of various inflammatory cytokines, induce antibody secretion, and modulate pathogen internalization to ameliorate the adverse effects.
Among several probiotic microorganisms, Lactobacillus sp., Bifidobacterium sp., and Saccharomyces sp. are the most rigorously investigated. 68,69 Several pre-clinical and clinical studies have shown the remarkable potential of probiotic supplementation in human subjects, especially in children diagnosed with acute diarrhea. A randomized controlled trial demonstrated that administration of L. rhamnosus GG in children aged between 6 months and 5 years suffering from acute watery diarrhea had significant improvements in the frequency, duration, and consistency of stool. 70,71
Similar results were obtained in a group of similar-aged children who were fed L. reuteri. 71,72 In another trial, B. lactis BB-12 supplementation resulted in a similar recovery outcome from acute diarrhea in children aged 15–23 months. 73 S. bouraldii has also been reported to be effective in reducing acute diarrhea in a group of children between ages 3 months and 5 years during a clinical trial. 74 Further, a meta-analysis report in 2006 also suggested the efficacy of probiotics Saccharomyces bouraldii, and Lactobacillus sp. in combination or as individuals in reducing the occurrence of acute diarrhea. 75
Excessive intake of antibiotics may lead to disturbances in gut microbiota, which subsequently make the body susceptible to pathogenic microbes, including Clostridium difficile, and such clinical manifestation is termed antibiotic-associated diarrhea or AAD. 76,77 Consumption of probiotics was found to mitigate the AAD crisis, and the idea behind using probiotics is to restore the original conditions of gut microflora. 78,79
Treatment of a group of children aged 1–12 years with a probiotic mixture containing B. lactis BB-12, L. rhamnosus GG, and L. acidophilus proved effective in ameliorating AAD. 80 In addition to the earlier discussed probiotics, several other microbial strains were recently investigated with promising potential to counter the symptoms of acute AAD. A group of children in a clinical trial was found to have recovered from acute diarrhea on being provided with Bacillus clausii. 81
The probiotic efficacy of B. clausii against rotavirus infection was further demonstrated using human enterocyte cell culture study. 82 Further, in two different clinical trials, AAD was found to be treated in groups of children fed a probiotic mixture (containing B. subtilis and B. licheniformis) and C. butyricum MIYARI strain. 83,84 Similarly, administration of the probiotic mixture containing C. butyricum and B. infantis was shown to restore gut microbiota and attenuate systemic inflammation in a mouse model of AAD. 85
In addition, the anti-diarrheal efficiency of probiotic microbial species such as Pediococcus spp., Leuconostoc sp., and Streptococcus sp. has also been investigated at pre-clinical levels. 86,87 Traveling brings hygiene issues, climatic variations, etc., which put travelers at a high risk of getting infected by diarrhea-causing pathogens (commonly called travelers disease). Intake of probiotics (L. rhamnosus GG) was shown to reduce the occurrence of diarrhea among travelers. 88,89
Consumption of L. rhamnosus GG provided evidence of probiotics-mediated pathogen clearing in the case of traveler's diarrhea, confirmed by the meta-analysis that showed that probiotic prevention of traveler's diarrhea was statistically significant. 90 Delving into the mechanism of action, different strains of probiotics may adopt different routes to fight against intestinal pathogens. Several in-vitro and animal studies demonstrated that probiotics inhibited the adhesion of pathogens to the host intestinal cell surface, possibly through competitive exclusion from host cell receptors. 91,92
Such competition may result in steric hindrance and structural and chemical modification of the receptors, which blocks the pathogens from binding to the host intestinal cells. 93,94 In addition, probiotics can also restrict the internalization of pathogens into host cells by modulating ERK1/2 MAP pathway mediated signal transduction, as well as enhancing the integrity of cell junctions of host intestinal epithelium by enhancing the expression of tight junction proteins, namely occludin and zonula occludens-1. 95,96
Further, probiotics have also been reported to stimulate the immune system of the host body, possibly by suppressing the production of reactive oxygen species and inflammatory cytokines such as IL-8, IFN-β, and enhancing the production of intestinal mucin and antibodies (especially IgA), as well as several peptides and proteins involved in the defense mechanism of host body. 7,97,98 The anti-pathogenic activity of probiotics can also be attributed to the secretion of certain peptides, which arrest the survival of pathogens as well as degrade the released toxins. 99,100
For instance, the protein bacteriocin produced by Gram-positive probiotics acts by increasing membrane permeability and interfering with cell wall synthesis to destroy pathogens. 101,102 In contrast, microcin produced by Gram-negative strains inhibits enzymatic activities that are crucial for synthesizing nucleic acids, thereby destroying the pathogen. 103,104
The accumulating evidence, therefore, suggests probiotics (most commonly Lactobacillus sp., Bifidobacterium sp., Saccharomyces sp., while recently Bacillus sp., C. butyricum, Pediococcus sp. Leuconostoc sp., Streptococcus sp.) as emergent and excellent therapeutics for treating different forms of diarrhea, especially acute and AAD, as well as a possible prophylactic to prevent diarrheal incidences. 12,89,91,105,106 However, a few studies also suggest the nil or marginal effect of probiotics against diarrhea. 93,107,108
Further, almost all the investigations till now support the efficacy of probiotics against diarrhea caused by rotavirus or E. coli infection, whereas reports supporting the same against other two most addressed diarrheal pathogens, that is, adenovirus and norovirus, are lacking, except one study that reported anti-noroviral effect of probiotic cocktail containing L. rhamnosus GG and the non-pathogenic strain E. coli Nissile 1917. 109
Also, evidence supporting the role of probiotics in treating traveler's diarrhea is limited, which demands more research activities in this area. Hence, more extensive and multifaceted investigations are required to focus on different microbial strains against different diarrheal pathogens, their dosage, composition, and host body responses to establish the efficacy and safety of probiotics in the treatment of diarrhea in varied human populations.
Helicobacter Pylori Infection
About 50–80% of the global population is annually infected by H. pylori, a Gram-negative bacterium that causes peptic ulcer, type B gastritis, and gastric cancer. 110 Entry of H. pylori into the host's GIT, followed by colonization, disrupts the normal gastric mechanism of activities and evokes inflammatory reactions, resulting in acute to chronic gastritis and ulcerative consequences on persistence.
The use of probiotics as therapeutic and prophylactic agents against H. pylori infections resulted in advantageous consequences. Supplementation of probiotics showed increased antibiotics' effects and provided favorable microbial balance in the host's GIT. Probiotics affect the cells of H. pylori by forming peroxide ions, causing oxidative damage to membrane lipids, DNA, and proteins of the pathogen. 111 Certain L. bulgaricus (GLB strain) produced antibacterial agents such as bacteriocin-like inhibitory substances (BLISs), which are heat-stable. BLIS showed an inhibitory effect on the growth not only to >81% of H. pylori antibiotic-sensitive strains but also to >71% H. pylori antibiotic-resistant strains. 112
Probiotics effects can be easily measured via reliable endpoints, including the subduing of infection, and combination treatments with antibiotics, thus leading to reduced after-effects such as acid reflux and lowered risk of repetitive infection. Within a few days, frequent heartburn and recurring acid reflux may act as symptoms for GERD (gastroesophageal reflux disease). Besides H. pylori infection, lifestyles such as smoking, excessive food consumption, late night eating habits, fried foods consumption, and beverages such as alcohol, etc. elevate GERD.
Studies showed that H. pylori infection is one of the prevalent reasons for GERD in some Asian countries. 113 Supplementation of certain Lactobacillus strains alone or a combination of probiotics of some strains of bacteria showed effective results in the eradication of H. pylori and also reduced disease-related symptoms. 114 Microencapsulation of lactic acid bacteria 115,116 was used to obtain the best delivery of probiotics into the intestinal tract.
The survival of microencapsulated cells was significantly higher when exposed to gastric juice at pH 2.0. Microencapsulated Lactobacilli cells were observed in larger amounts in simulated small intestine juice, suggesting the potential of the encapsulated therapy to reduce H. pylori infection.
Among different probiotics with therapeutic efficacy against H. pylori, non-pathogenic microbes such as Lactobacillus sp., B. bifidum, and S. boulardii exhibit promising effects. Evidence from several ex vivo and in vivo studies suggests that different strains of Lactobacillus, including L. acidophilus, L. bulgaricus, L. rhamnosus, L. plantarum, L. reuteri, L. johnsonii, possess remarkable therapeutic abilities to be used as probiotics against H. pylori infection. 117,118
Moreover, in a double-blind placebo-controlled trial, L. reuteri administration in H. pylori infected human subjects led to significant reductions in pathogenic load and urease activity in addition to ameliorated GIT symptoms, including abdominal pain, acid and acid regurgitation, epigastric burn, stool inconsistency, etc. 119 H. pylori-infected gastrointestinal cells and animal models treated with probiotics containing B. bifidum had significant declines in pathogenic load and a reduced extent of gastric tissue damage. 120,121
Similar results, along with the decline in serum pepsinogen and allied gastrointestinal symptoms, were observed in H. pylori-infected human subjects on treatment with B. bifidum. 122,123 Probiotic efficiency against H. pylori infection has also been shown by the yeast strain S. bouraldii, as evident in previous human clinical trials. 124,125
In addition to the earlier discussed known probiotics, other strains, including C. butyricum, Bacillus subtilis, and Pediococcus acidilactici, have also been investigated in ex vivo and in vivo studies, and the findings report significant antibacterial effects of these strains against H. pylori infection. 126,127 Further, it is noteworthy to mention that treatment with probiotics was also found to alleviate the adverse side effects (such as nausea, taste disturbance, diarrhea) of antibiotic therapy against H. pylori infection by enhancing adaptation to the changed intestinal microbiota. 128,129 Delving into the action mechanism, probiotics adopt different ways to inhibit H. pylori activity and destroy the pathogenic cells (Fig. 3).
A schematic diagram showing different routes adopted by probiotics to counter and reduce pathogenic loads.
Urease is an essential enzyme secreted by bacteria to generate ammonia and bicarbonate on hydrolyzing urea. When released into the cytosol, these substances create a passage for bacteria to gain entry through the mucus layer that has been reformed into a viscous solution of increased pH from elastic and low viscous mucus layer. 130
Accumulating data indicate that lactic acid bacteria (LAB) such as B. longum, Lactobacillus species, etc. can reduce the urease activity of H. pylori, which is an important factor for the pathogen to survive in the host body. Also, when utilized as probiotics, LAB showed a reduction in gastritis and lowered the risk of infection of H. pylori without inducing any adverse side effects. 128,131,132
H. pylori was also reported to suppress the expression of genes and proteins responsible for mucin secretion in the host, thereby disrupting the host defense system, whereas probiotics, such as L. plantarum and L. rhamnosus, on the other hand, restored the host intestinal mucin production by upregulating the expression of genes MUC2 and MUC3, thus reinstating the mucosal permeability in the host. 133
Restoration of the host defense system is also exhibited through stimulating the secretion of immunoglobulins (IgA, IgG, IgE) by host immune cells to attack and destroy the H. pylori pathogens. 134 Further, H. pylori pathogenesis involves over-secretion of pepsinogen I and/or II, and pro-inflammatory cytokines (IL-6, IL-8, TNF-α), which marks gastrointestinal inflammation and subsequently leads to gastric and peptic ulcer, tumor, etc. 135 Probiotics modulate pepsinogen secretion and downregulate the expression of pro-inflammatory cytokines in the host's GIT, thereby reducing gastric inflammation.
For instance, H. pylori-infected human gastric epithelial cells exhibited an upsurge in the expression of IL-8 and TNF-α that was reported to be reduced by treatment with Lactobacillus sp. and Bifidobacterium sp.. 118,136 Other important antagonistic mechanisms adopted by probiotics against H. pylori include the secretion of anti-bacterial substances such as lactic acid, hydrogen peroxide, and bacteriocin that cause cell membrane disruption, oxidative damage, and nucleic acid fragmentation in pathogens. 137,138
Surprisingly, a study reported that the probiotic B. subtilis renders its effect against H. pylori infection through antibiotic secretion. 139 However, similar evidence in support of the same is lacking. Further, probiotics have also been observed to strongly restrict the binding of other microbes to host cell receptors, thereby inhibiting the adhesion of H. pylori to the gastrointestinal cells of the host. For instance, the probiotic L. reuteri inhibited H. pylori attachment to glycolipid receptors on the host cell surface by competing for binding sites. 140
Similarly, S. boulardii was found to inhibit H. pylori binding to membrane-bound sialic acid on human duodenal cells by exhibiting neuraminidase activity against the sialic acid residues in an ex vivo study. 141 Thus, the accumulating scientific evidence suggests that there is strong therapeutic efficiency of probiotics against H. pylori infection.
Eradication of the pathogen from the host body, reduction of the adverse consequences rendered by the pathogen on the host's gastrointestinal tissues, and attenuation of antibiotic-associated side effects are some of the beneficial outcomes of probiotic consumption against H. pylori infection. It is further important to mention that probiotic yogurts have benefited human health against pathogenic infections. The beneficial effect of probiotic yogurt with L. acidophilus and B. bifidum in restoring the intestinal microbiota and immunity in H. pylori-infected children.
Children with H. pylori infection showed significant increases in pepsinogen I and II levels, unaltered levels of IgG and IgE, high serum cytokine levels for IL-6, IL-10, TNF-α, and significantly lower IgA levels than uninfected controls. 135 Yogurt consumption restored the gut microbiota and stimulated the secretion of pepsinogen II to reduce the pepsinogen I/II ratio, in addition to stimulating serum IgA and decreasing the IL-6 level to suppress H. pylori colonization. 135 Therefore, the outcomes of these studies provide a strong rationale to consume yogurt regularly to maintain balanced intestinal microbiota and stimulate cellular and humoral immunity to reduce gastric pathogens.
However, a few reports also suggest that probiotics in combination with antibiotic therapy can prove more effective in treating H. pylori infections, thus indicating its efficacy more as an adjunct or supplement than as a therapeutic. 110,142 Another report also indicated the failure of the probiotic L. plantarum to exert any therapeutic effect against H. pylori infection. 143 Therefore, more extensive investigations are required to strengthen the scientific evidence for the therapeutic efficacy of probiotics in the treatment of H. pylori insults.
Future Directions
Research should be continued to properly characterize existing probiotics, identify the strain-specific health attributes, and determine efficacy doses. Evidence indicates the potential of probiotics to provide diverse health benefits on the consumption of optimal doses. Both dedicated efforts and policies are needed to confirm how such health benefits are conferred in humans while adhering to the probiotic use guidelines.
Stricter regulations should be in place to maintain safety protocols according to international standards such that the use of probiotics does not compromise human health. This is because an imbalance in the bacterial colonies in the intestine may trigger a cascade of reactions in the immune system, thereby resulting in small intestine and colon inflammation in addition to other negative ramifications.
Therefore, to produce the desired effects, the probiotics need to be delivered at levels that ensure the safety of the targeted site within the GIT and the whole body. Gut-targeted probiotics face maximum adversities, the biggest being stomach acidity and the presence of bile in the duodenum before reaching the targeted site and bringing about the desired effects. The current era of probiotics is to search for bacterial strains with the most potential to withstand such in vivo adversities while providing health benefits to human consumers.
Footnotes
Acknowledgments
The article is dedicated to the loving memory of late Dr. Sanjeev Kumar (first author), a brilliant scientist, whose contributions to the field of biological sciences will continue to inspire us. A.K.P. and his team is thankful to ICAR-NDRI for providing funding and other necessary support; M.S. to DST-Haryana (HSCSIT/R&D/2021/461), India, for the award of JRF (Financial support).
Authors' Contributions
Conceptualization, S.K., M.S., M.S., M.P., T.D., M.F.A, R.E.A., and A.K.P; writing—original draft preparation, S.A., P.N., R.R., R.B., I.G., V.L.D., H.S.D., E.S, M.P., and M.S.; writing—review and editing, T.D., R.E.A., A. R., H.H., S.Y., and A.K.P. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
The research program of Dr. R.E. Aluko is funded by the Natural Sciences and Engineering Council of Canada (NSERC), funding reference No. RGPIN 2018–06019. This research was supported by ALIES a non-profit Association for the Development of Research and Education in Health Sciences.