
Abstract
Oral nutritional supplements (ONSs) offer support for the nutritional needs of surgical patients. However, their efficacy is contingent upon the nutrient composition, absorption efficiency, and postingestion tolerance. Our study included a cohort of 84 patients who underwent elective open surgery involving at least one intestine anastomosis. To mitigate the risk of malnutrition, 2 groups of 28 patients each received either a high-protein low-osmotic ONS (Group I) or a high-calorie high-osmotic ONS (Group II). A standard diet was used in the control group (Group III). The metabolic effects were evaluated by measuring body weight and relative change in body weight (Δkg) from 24 h (−1 day) presurgery to 28 days postprocedure. Subjective tolerance following ONS consumption on the second postoperative day was also assessed. Our findings showed that, across all groups, the average body weight decreased during the initial 2 weeks postsurgery, subsequently stabilizing or returning to baseline levels by the third and fourth week of observation. Patients receiving ONS demonstrated greater weight gain between days 14 and 28, with Group I exhibiting the highest rate of gain. Low-osmotic ONS displayed superior tolerance and elicited fewer patient complaints postconsumption. Postoperative hospitalization duration did not differ significantly among the nutritional strategies. In conclusion, early administration of ONS supplies essential nutrients and facilitates refeeding, thereby reducing the risk of malnutrition. Low-osmotic preparations are better tolerated and contribute more effectively to the restoration of preoperative body weight, despite their lower caloric content.
INTRODUCTION
Approximately half of hospitalized patients encounter malnutrition, with nearly one in six experiencing rapid weight loss shortly after hospital admission. 1,2 The primary risk factors implicated in the development of malnutrition include active cancer diagnoses, advanced age, prolonged hospital stays, and surgical interventions, notably abdominal or head and neck procedures. 3,4
Since the 90s, surgical guidelines have advocated a heightened emphasis on preoperative nutritional quality, cessation of detrimental habits, and improvement of physical fitness. Presently, the combat against malnutrition constitutes a keystone of prehabilitation and stands as one of the pillars within the Enhanced Recovery After Surgery (ERAS) protocol. 5 Notably, given that up to 40% of surgical patients require nutritional intervention, the European Society of Parenteral and Enteral Nutrition (ESPEN) recommends a minimum of 7 days of nutritional treatment before planned surgical procedures. Concurrently, the restriction of fasting duration, coupled with individualized postoperative management, not only reduces the risk of postoperative complications but also improves long-term outcomes. 3,4,6
In accordance with the ERAS protocol, patients identified as malnourished or at risk of malnutrition should be supported with oral nutritional supplements (ONSs) as a component of surgical complication prevention. ONSs protect the gastrointestinal (GI) tract during fasting, stabilize intestinal microflora, and facilitate faster refeeding immediately following surgical intervention. Nonetheless, the specific guidelines regarding ONS treatment, including the optimal single dose, daily intake, and overall duration of supplementation, remain subjects of ongoing discussion. 7
The efficacy of therapy is determined by the concentration of dissolved ingredients, particularly proteins and calories, and the relative proportions of nutrients, along with the addition of immunomodulators. Another issue worth considering is the timing of oral supplementation initiation following surgery and the effectiveness of enteric absorption during the postoperative phase. Intestinal resections and anastomoses decrease bowel motility, ultimately compromising the patient's tolerance to ONS. 8,9
The aim of the study was to evaluate the effectiveness of ONS in the prevention of postoperative malnutrition and to assess the impact of such supplementation on metabolic recovery.
MATERIALS AND METHODS
A prospective randomized study was carried out at the authors' clinic from 2018 to 2021, involving a cohort of 84 patients (52 women and 32 men), with ages ranging from 23 to 85 years, who underwent elective open segmental resection of the intestine with at least one anastomosis. Eligibility criteria included full oral feeding capacity, a body mass index (BMI) of ≥20, and a Nutritional Risk Screening (NRS) 2002 score of less than 3. In all patients, the clinical, radiological, and/or endoscopic examination confirmed the full efficiency of the GI tract. In turn, preoperative malnutrition and comorbidities limiting the ability of enteral food absorption as well as early postoperative complications significantly restricting oral nutrition constituted exclusion criteria from the study. A comprehensive list of exclusion criteria can be found in Table 1.
Exclusion Criteria from the Study
BMI, body mass index; ONS, oral nutritional supplement; SBS, short bowel syndrome.
The indications for surgery were locally advanced colorectal cancer (≤T2 in the TNM classification), diverticular disease (inflammatory tumor), GI reconstruction after Hartmann's procedure, low-output enterocutaneous fistula, and intestinal adhesions requiring segmental bowel resection. On the first postoperative day, all patients were administered clear fluids orally and incomplete parenteral nutrition (ready-to-use concentrate) with a volume of 1000 mL. On postoperative days 2 and 3, they transitioned to a full liquid diet based on soups and pulps, extended to include solid foods from the fourth day.
To prevent malnutrition, postoperative nutritional supplementation was initiated for 56 patients. Of these, 28 patients (Group I) received a low-osmotic supplement for a period of 1–14 days following the procedure, while the remaining 28 patients (Group II) were prescribed a high-osmotic preparation. Both types of ONS were administered at a dosage of 200 mL twice a day. Group III, consisting of 28 patients who did not receive oral supplementation, served as the control group in the study. Detailed characteristics of both types of ONS are provided in Table 2.
Characteristics of High and Low Osmotic Oral Nutritional Supplements
The metabolic effects were assessed by measuring body weight 1 day (−1 day) before the surgery, and then on days 2, 4, 7, 14, and 28 after the procedure. The relative change in body weight (Δkg), representing weight gain or loss between the measurement days, was calculated. The duration of hospitalization postsurgery and the tolerance of ONS in Groups I and II were also analyzed. To assess tolerance, a survey was administered on the second postoperative day, before the introduction of a full diet based on solid foods, as outlined in the questionnaire (Table 3).
The Subjective Scale of Assessment of Tolerance After Consumption of Oral Nutritional Supplements
Characteristics of the Performed Procedures
RESULTS
Surgical interventions in our study primarily targeted colorectal cancer, accounting for 51 patients, while nononcological indications, notably GI reconstruction following Hartmann's procedure and diverticular disease, were predominant in other cases. A single anastomosis was performed in 80 cases, while four patients required two anastomoses. The choice of surgical technique favored stapled sutures in 67 cases and handmade anastomoses in 21 patients.
Mean body weight increased temporarily on the second postoperative day, followed by a decline in the majority of patients within the initial 14 days postsurgery. Over the next 2 weeks, body weight either stabilized or returned to the baseline. However, the mean value in all groups at the end of the observation period was slightly lower than before the procedure (Fig. 1). Notably, patients who received ONS demonstrated a more pronounced weight gain between days 14 and 28, with the most substantial increase observed in the low-osmotic ONS group (Fig. 2). Furthermore, the low-osmotic ONS group exhibited the highest proportion of patients who achieved a body weight of at least equivalent to their preprocedure weight by the 28th postoperative day (Fig. 3).

Mean body weight measured in the following days after the procedure in patients receiving a low or high osmotic ONS and in the control group. ONS, oral nutritional supplement.
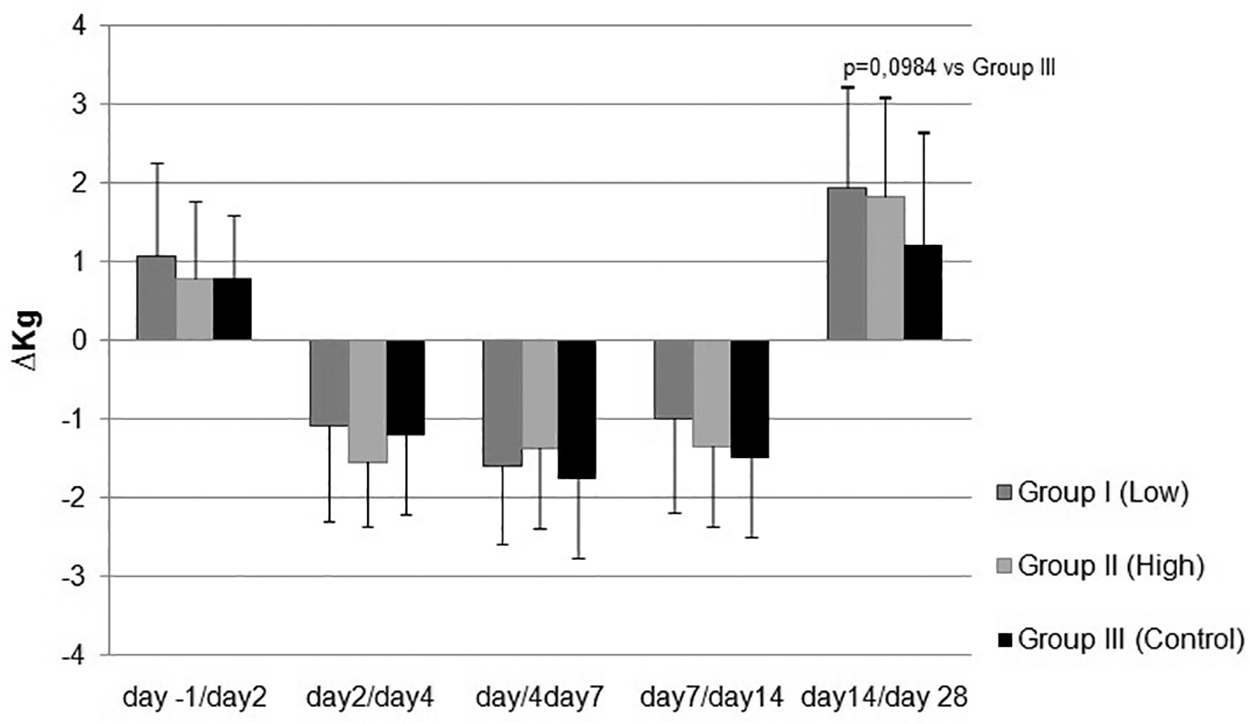
Relative change in mean body weight (Δkg) measured in the following days after the procedure in patients receiving a low or high osmotic ONS and in the control group.
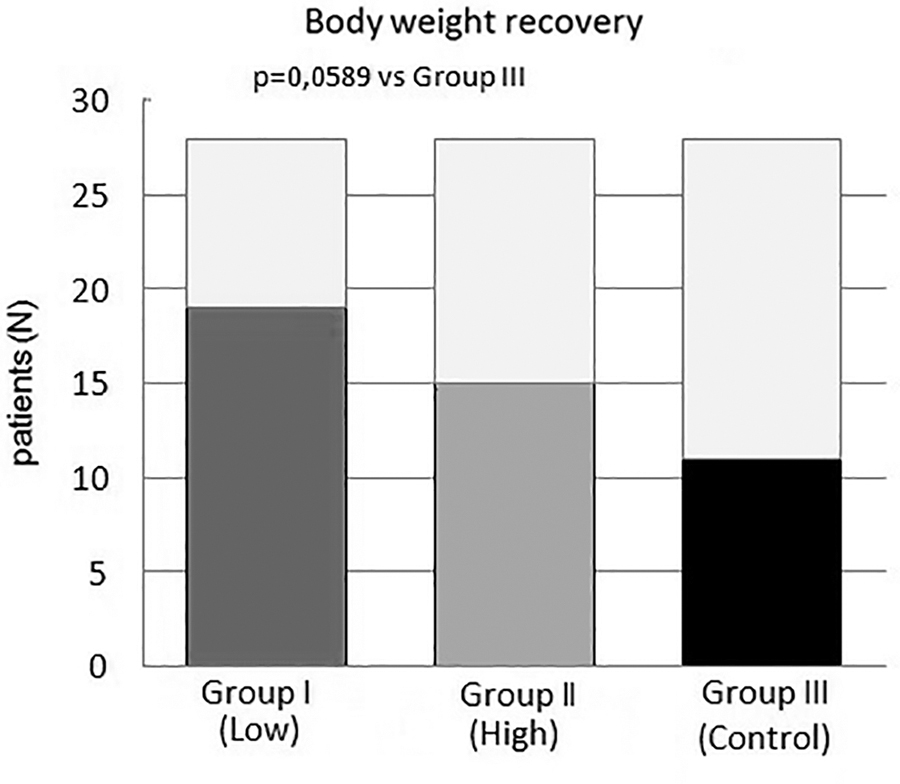
Percentage of patients whose body weight on day 28 after surgery was the same or greater than the weight before surgery (day −1).
The low-osmotic ONS had the best tolerance and minimal rate of patient complaints after consumption. Complaints such as nausea or flatulence were least frequently reported by patients in Group I (Figs. 4 and 5). In addition, patients in Group I reported fewer objections regarding the taste, usually assessing it as good or neutral (Fig. 6).
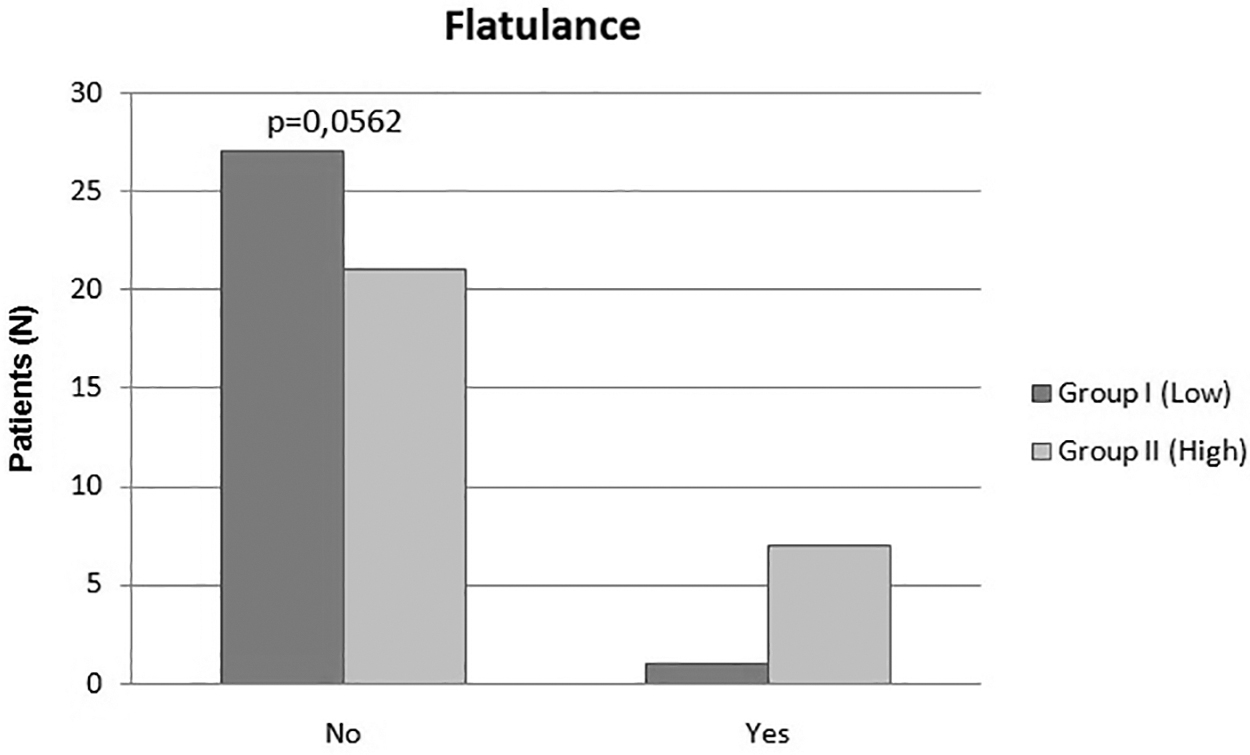
Subjective assessment of tolerance of a low-osmotic (Group I) and high-osmotic (Group II) ONS in relation to a diet not enriched with supplements (Group III)—flatulence evaluation.

Subjective assessment of tolerance of a low-osmotic (Group I) and high-osmotic (Group II) ONS in relation to a diet not enriched with supplements (Group III)—nausea evaluation.

Subjective assessment of tolerance of a low-osmotic (Group I) and high-osmotic (Group II) ONS in relation to a diet not enriched with supplements (Group III)—taste evaluation.
Most patients were discharged from the hospital on the sixth or seventh day postsurgery, irrespective of their chosen nutritional strategy. There were no significant differences in the duration of postoperative hospitalization among the groups under study.
DISCUSSION
The majority of studies on prehabilitation confirm that preoperative malnutrition may increase the risk of complications, thereby exerting a detrimental impact on the surgical treatment's ultimate outcome. 10 Nonetheless, the metabolic consequences associated with surgical trauma and the temporary suspension of oral nutrition remain subjects of research, as does the inquiry into postoperative nutritional strategies aimed at mitigating the potential for malnutrition. 10 The extent of injury related to surgical techniques, coupled with the secondary dysfunction of other organ systems, influences the metabolic efficiency of the GI tract and dictates the magnitude of nutritional deficits. A delayed diagnosis or an inappropriate treatment regimen leads to prolonged hospitalizations, escalated health care expenditures, and an elevated risk of recurrence in subsequent months.
Currently, the gold standards in perioperative management are grounded in the ERAS protocol. This protocol advocates the monitoring of nutritional status and the identification of patients at risk of metabolic complications. Particular emphasis is placed on the avoidance of unwarranted preoperative fasting by patients and the promotion of early initiation of oral nutrition and physical activity during the postoperative phase. 10,11 Recommendations regarding dietary management predominantly apply to patients who have undergone extensive GI procedures, such as gastrectomy or pancreatic resection. 12 However, it is worth noting that a significant number of abdominal surgeries elicit short-term but profound malnutrition immediately following the day of the operation.
Early refeeding offers a dual advantage: first, it provides natural food products, and second, it promotes a trophic effect on the intestinal mucosa. In addition to a high-calorie diet, ONS benefits patients with increased metabolic demands, particularly during the early postoperative phase. 9 Furthermore, these laboratory-prepared emulsions, whether single- or multi-ingredient, should also be considered for patients experiencing temporary digestive dysfunction due to obstruction or intestinal microbiota dysfunction. Postoperative peritoneal irritation and transient anastomotic insufficiency diminish intestinal motility and intraluminal absorption, resulting in diminished appetite, abdominal distension, nausea, or diarrhea. Therefore, the metabolic advantages of ONS depend not solely on the total caloric or protein intake but also on GI tolerance. 13,14
Clinical practice has proven that ONSs with lowered osmolarity, corresponding to physiological fluids, minimize the number of adverse reactions. This correlation applies especially to patients with GI insufficiency, including those after surgical procedures. The osmolarity of commonly available ONSs ranges from about 350 to even 700 mOsm/L and is directly proportional to the amount of dissolved nutrients. It is symptomatic that ONSs with the highest osmolarity, containing even 2 kcal/mL, although they could ideally cover the metabolic demands, are often poorly tolerated and most often excluded from use. 14,15 Single-ingredient low-osmotic supplements, although nutritionally incomplete, better support oral diet, and protein supplements because of their neutral taste, relatively low osmolality, and limited composition reflect the needs of the surgical patient.
The quality of ONS is further elucidated by considerations such as the source of protein and the extent of its hydrolysis, as well as the overall dietary fiber content. In turn, the presence of simple carbohydrates can restrict the use of certain ONSs in patients with conditions such as diabetes or other disorders characterized by glycemic instability. Recent investigations also underscore the favorable impact of immunomodulatory constituents, such as L-arginine or L-glutamine, which serve to enhance blood microcirculation and fortify immune responses. 16,17 Moreover, the practical efficacy in everyday therapeutic application is contingent upon factors such as the formulation of the supplement (e.g., liquid, powder, or pudding), the feasibility of integration with other dietary components, and the stability at elevated temperatures. 18
In addition to laboratory tests, body weight and BMI serve as valuable diagnostic tools for assessing malnutrition and monitoring the efficacy of the implemented treatment strategy. 3 Gradual weight loss during the postoperative period corresponds to reduced energy intake and is a consequence of the discontinuation of oral nutrition along with temporary dysfunction of the digestive tract. Simultaneously, some researchers investigate the relationship between rapid postprocedural weight gain and disturbances in fluid balance. 19,20 This may be associated with mandatory fluid therapy, especially following extensive abdominal procedures, or it may result from excessive fluid retention, such as that occurring in cases of circulatory insufficiency, acidosis, or sepsis. Furthermore, a substantial increase in body weight has also been observed in patients experiencing postoperative complications and those with prolonged hospital stays. 20 –22
To ensure the maintenance of appropriate body weight, it is imperative to stimulate the patient's food consumption, which, in turn, depends on the taste and aroma of the diet. Alarmingly, as many as 55% of surgical patients, including those undergoing orthopedic procedures, report a partial or complete loss of appetite during the initial 2–4 weeks following surgery. 23,24 This outcome not only leads to reduced nutrient absorption but also gives rise to hypoalbuminemia and a heightened likelihood of fluid retention. Subsequent tissue edema further increases body weight and hampers postoperative rehabilitation, thereby amplifying the risk of postoperative mortality. 20
In conclusions, surgical patients, due to their exposure to trauma and temporary GI dysfunction, constitute a particularly vulnerable group susceptible to metabolic deficits and weight loss. Consequently, if oral feeding is feasible, the consideration of ONS is warranted, particularly within the initial 14 days following surgery. This is especially relevant when utilizing high-protein, low-osmotic formulations enriched with immunomodulators. 8,25 It remains an open question whether the enhancement of metabolic parameters in patients receiving ONS is attributable solely to the consumed supplement or if it also stems from the supplement's beneficial impact on enteric absorption and intestinal microbiota. It is probable that improved tolerance of low-osmotic compounds could enhance nutrient assimilation, subsequently increasing meal volume and frequency during the postoperative phase.
Footnotes
AUTHORs' CONTRIBUTIONS
J.C.: Conceptualization, data curation, formal analysis, methodology, and visualization. A.C.: Formal analysis, writing—original draft, and visualization. B.K.: Formal analysis, writing—original draft, and writing—review and editing. W.Z. and H.C.: Data curation, writing—review and editing, and visualization. T.B. and J.P.: Methodology and supervision.
ETHICAL STATEMENT
The study was performed in accordance with the hospital standards and good medical practice. Patients provided informed written consent before all medical procedures. After reviewing the study protocol, the regional bioethics committee decided that a special consent for the study was not necessary.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.