
Abstract
The ketogenic diet (KD) has long been used in the treatment of drug-resistant epilepsy, demonstrating significant beneficial health effects. Various modifications of the KD have been introduced as alternatives to the classical, more restrictive form, aiming to improve patient’s adherence while maintaining therapeutic efficacy. Among these adaptations, the Mediterranean ketogenic diet (MedKD) has been primarily implemented in populations in the Mediterranean region. The MedKD integrates elements of the traditional Mediterranean diet, with olive oil as the primary fat source, leveraging its unique properties. This narrative review examines the possible connections between olive oil and the mechanisms of KD, proposing the extra virgin olive oil-rich MedKD as a healthier option with the potential for reduced adverse effects.
INTRODUCTION
Epilepsy is a common cause of neuronal dysfunction, leading to seizures that impact behavior, learning, and memory. 1 The ketogenic diet (KD), effective in treating drug-resistant epilepsy, reduces seizure frequency and severity, while improving cognition, behavior, and quality of life. 2,3 The KD is a high-fat, low-carbohydrate, adequate-protein dietary pattern that mimics fasting. 4 Its effectiveness is linked to ketone bodies (KBs)—mainly β-OH butyrate (BHB), acetone, and acetoacetate—produced in the liver, providing an alternative energy source for the brain. 5,6 Additional therapeutic effects of KD include changes in glucose metabolism, enhanced mitochondrial function (e.g., increased ATP production and reduced reactive oxygen species [ROS]), and the inhibition of mammalian target of rapamycin activity. This dietary pattern also activates peroxisome proliferator-activated receptors (PPARs) (PPARα and PPARγ) through increased polyunsaturated fatty acids intake (PUFAs), contributing to reduced neuronal excitability and seizure control. 7
KD-induced changes in gut microbiota may also contribute to seizure reduction by activating the “gut-brain axis.” 8 Animal and clinical studies suggest that microbial populations and their metabolites can influence brain functions by reversing gut dysbiosis. The gut microbiome may thus mediate KD’s beneficial effects in drug-resistant epilepsy, as well as in neurodegenerative disorders like Parkinson’s and Alzheimer’s disease (AD). 9
Despite its beneficial health effects, a major limitation of the KD is its low compliance rates, due to difficulties patients encounter to meet the high lipids and low carbohydrates requirements. The classical KD typically has a 4:1 or 3:1 lipid-to-protein and carbohydrate ratio, though other ratios (e.g., 2:1, 1:1) have also proven effective. Alternative diets such as the Modified Atkins Diet, the medium chain triglycerides (MCT) diet, and the low glycemic index therapy are less restrictive, allowing more carbohydrates and proteins, with better compliance rates while maintaining efficacy. 10 –13
In addition to adherence challenges, the KD can cause short-term side effects, such as nausea, vomiting, and constipation, and long-term health problems, mainly hyperlipidemia, nephrolithiasis, and stunted growth. 10 Parents and caregivers often experience increased stress stemming from the prolonged implementation of KD, due to daily management difficulties, social restrictions, and economic concerns. 14 This stress can negatively impact compliance, leading to diet discontinuation. Low compliance rates, often cited as the main reason for KD discontinuation, may also be related to the taste issues and the inadequate education and communication with health care providers. 15
The Mediterranean version of the ketogenic diet (MedKD) has recently been proposed as an alternative to traditional KD for epileptic or metabolically deranged patients. This approach combines many beneficial effects while addressing some of the limitations of the standard KD. 16 –19 The traditional Mediterranean diet (MedDiet) pattern has been widely studied and is associated with numerous positive health outcomes. Strong evidence from large clinical trials and observational studies relates MedDiet to a lower incidence of cardiovascular disease (CVD), diabetes, obesity, metabolic syndrome, neurodegenerative diseases such as Alzheimer’s, and several types of cancer. 20 Under this perspective, MedDiet emphasizes the abundance of plant-based foods, that is, fruits, vegetables, legumes, whole grains, seeds, and plant oils (especially olive oil), along with moderate amounts of dairy products such as cheese and yogurt. It also includes moderate amounts of fish and poultry, limited red meat amounts, and low-to-moderate wine consumption with meals. 4 MedKD provides a more palatable and sustainable alternative while preserving the therapeutic benefits of the traditional ketogenic approach.
Olive oil, a key component of the MedDiet, offers well-established health benefits. 21 Using olive oil as the primary fat in a KD may enhance therapeutic effects due to its unique constituents. The MedKD for drug-resistant epileptic patients, who often require long-term KD treatment, could potentially reduce adverse effects, such as hyperlipidemia.
To our knowledge, there is limited evidence examining the role of olive oil in epileptic patients following KD therapy. In this narrative review, we aim to explore the benefits of MedKD in epileptic patients, emphasizing how olive oil components are involved in specific mechanisms of the KD applied.
HEALTH EFFECTS OF THE MEDKD
The MedKD aims to incorporate elements from the traditional MedDiet, offering positive health effects, and has been proposed for various patient populations (Table 1). In a pilot interventional study, a 6-week MedKD with phytoextracts was tested on 106 adults with a BMI >25 kg/m2, resulting in weight loss and improved lipid profiles. 22 Another interventional study on 40 obese adults with a BMI >36 kg/m2 tested a Spanish version of the MedKD, which included 30 mL of virgin olive oil, 30 g of carbohydrates from vegetables, and 200–400 mL of red wine daily. This 12-week diet, with no restrictions on calories or protein, led to significant weight loss and improvements in blood pressure, fasting glucose, and lipid levels. 23 The MedKD also showed positive effects on adults with metabolic syndrome and non-alcoholic fatty liver disease. 24,25
Implementation of the Mediterranean Ketogenic Diet (MedKD) Across Various Populations
AD, Alzheimer’s disease; CSF, cerebrospinal fluid; KD, ketogenic diet; LDL, low density lipoprotein; NAFLD, non-alcoholic fatty liver disease; SGOT, serum glutamic oxaloacetic transaminase; SGPT, serum glutamic pyruvic transaminase; TG, triglycerides.
The combined Mediterranean and KD has been proposed for patients with multiple sclerosis, with benefits attributed to their anti-inflammatory and antioxidant properties. This dietary regime recommends low glycemic index carbohydrates, moderate caloric restriction, and a ratio of dietary ω3/ω6 fatty acids 1:4, comprising 15% saturated fatty acids (SFAs), 25% monounsaturated fatty acids (MUFAs), and 60% PUFAs, covering in total 80% of total energy intake. 28
A group of 17 older adults at risk for AD was studied in a randomized crossover double-blinded trial: patients were advised to follow either a MedKD or the American Heart Association Diet (AHAD), and changes in gut microbiota, short-chain fatty acids (SCFAs), and cerebrospinal fluid AD markers were evaluated. 18,19 The MedKD consisted of meals containing less than 20 g of carbohydrates daily, with a high-fat content, emphasizing olive oil and minimizing saturated fat sources. Both diets altered the gut microbiome in cognitively normal adults and adults with mild cognitive impairment, while the MedKD was associated with improvement in AD markers, lipid profile, and glucose metabolism. 19
These findings highlight the potential of combining Mediterranean and KDs for therapeutic benefits in neurological conditions, like multiple sclerosis and AD. The emphasis on olive oil and the careful balance of dietary fats are key components of these protocols, providing a healthier approach with fewer adverse effects.
The MedKD for epilepsy
The potential effects of a MedKD diet in epilepsy was tested in a study of 389 children with drug-resistant epilepsy in Turkey: patients were suggested to follow an olive-oil-based KD with olive oil providing 80–85% of the fat content in each meal, excluding other oils 17 (Table 1). The results of this trial indicated that the MedKD remained highly effective in reducing seizures and improving behavior in 83.1% of 160 patients who completed 12 months on KD. This increased responsiveness was associated with high compliance, possibly attributed to the use of olive oil as a more palatable fat source in the local recipes provided to the patients.
However, in a subset of 121 children, the diet led to an increase in the blood levels of total cholesterol, low-density cholesterol (LDL), and triglycerides, despite the high olive oil content. 26 Another cohort of 52 children from the same study showed no negative effects on carotid intima thickness, even with elevated blood lipids, suggesting that MedKD may have cardioprotective effects through other mechanisms in children with drug-resistant epilepsy. 27
OLIVE OIL: COMPOSITION AND PROPERTIES
Olive oil, one of the most studied dietary fats, is derived from the fruit of the olive tree (Olea europaea L.) and is one of the main components of the MedDiet. It is primarily produced in Mediterranean countries, Spain, Greece, and Italy, where it plays a central role in both dietary habits and culture. Olive oil is categorized into three types based on quality, production processes, organoleptic characteristics, and acidity: virgin olive oil (VOO), extra virgin olive oil (EVOO), and lampante oil. EVOO has the highest quality, with a unique flavor and acidity of less than 0.2 g/100 g. 29
Olive oil is primarily composed of triglycerols, making up 97–99% of its content, while the remaining 2% consists of bioactive compounds like polyphenols, sterols, tocopherols, and carotenes. 30 The main fatty acid in olive oil is oleic acid (C18:1), which accounts for 70–85% of the MUFAs. Oleic acid, along with phenolic compounds such as hydroxytyrosol and oleuropein, contributes to the unique nutrient profile of olive oil and its health benefits. 29,31
Recent metabolomic studies highlight olive oil’s mechanisms in anti-inflammatory, antimicrobial, and antioxidant pathways 30 (Fig. 1). Its components, namely hydroxytyrosol and oleuropein, protect cells from ROS, helping prevent chronic diseases such as cardiovascular issues, neurodegenerative disorders, diabetes, and cancer. 32 Olive oil phenolics also prevent LDL oxidation. 33
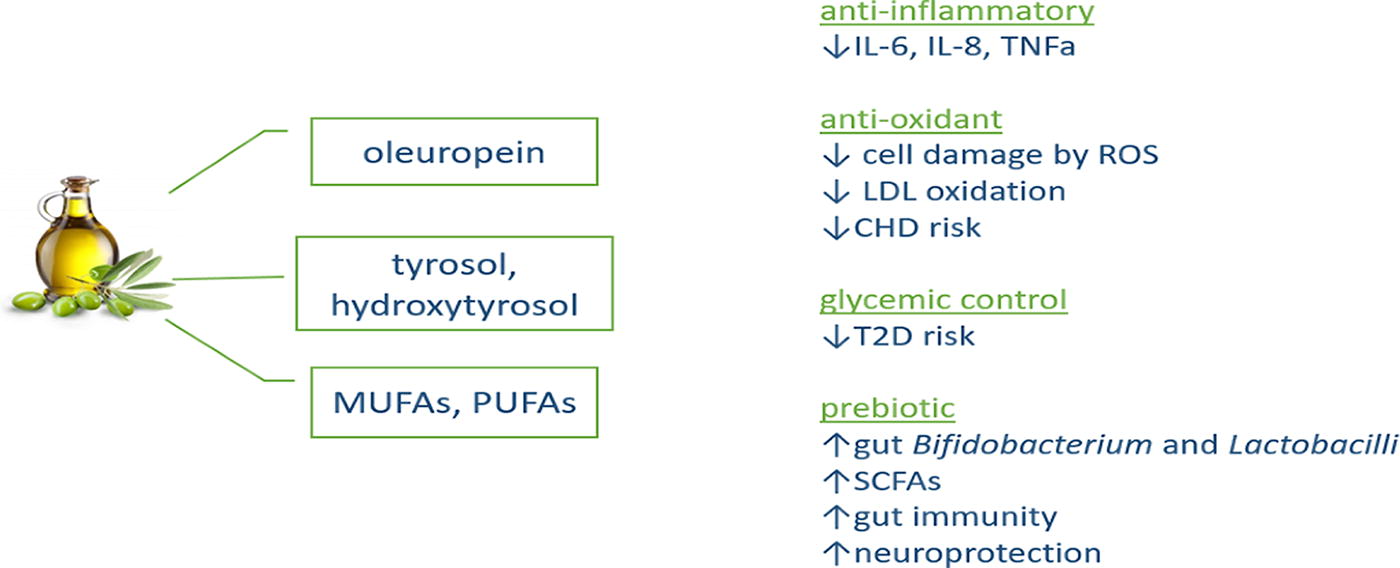
Olive oil properties. IL-6/IL-8, interleukin 6/8; LDL, low-density lipoprotein; MUFAs: monounsaturated fatty acids; ROS, reactive oxygen species; SCFAs, short-chain fatty acids; T2D, type 2 diabetes; TNFa, tumor necrosis factor a.
The PREDIMED study provides strong evidence that the consumption of olive oil, as part of the MedDiet, contributes to a reduction in cardiovascular risk. 34 In this multicenter, parallel-group, randomized 5-year trial, adult participants at high risk for CVD who adhered to a MedDiet supplemented with EVOO or nuts experienced a significantly lower risk of serious cardiovascular events compared with those following a low-fat diet. 34 This finding underscores the importance of specific components of the MedDiet in promoting its effectiveness.
Olive oil polyphenols help control glycemia and prevent type 2 Diabetes as observed in clinical and preclinical studies. 35,36 Additionally, olive oil’s polyphenols and MUFAs reduce inflammatory cytokines such as interleukin-6 (IL-6) and IL-8. 37 –39
The prebiotic and antimicrobial actions of MUFAs and phenolic compounds of olive oil are associated with the increased abundance of bifidobacteria and lactobacilli and the SCFAs produced in the colon, affecting mucosal immunity and exerting neuroprotection and cognitive improvement via the “gut-brain-axis.” 40
THE POTENTIAL ROLE OF OLIVE OIL AND ITS CONSTITUENTS IN THE OBSERVED EFFECTS OF THE MEDKD
Clinical evidence for the beneficial effects of a MedKD approach is limited. Nonetheless, olive oil’s unique properties and its attributed health effects may potentially interact with the mechanisms of KD (Fig. 2).
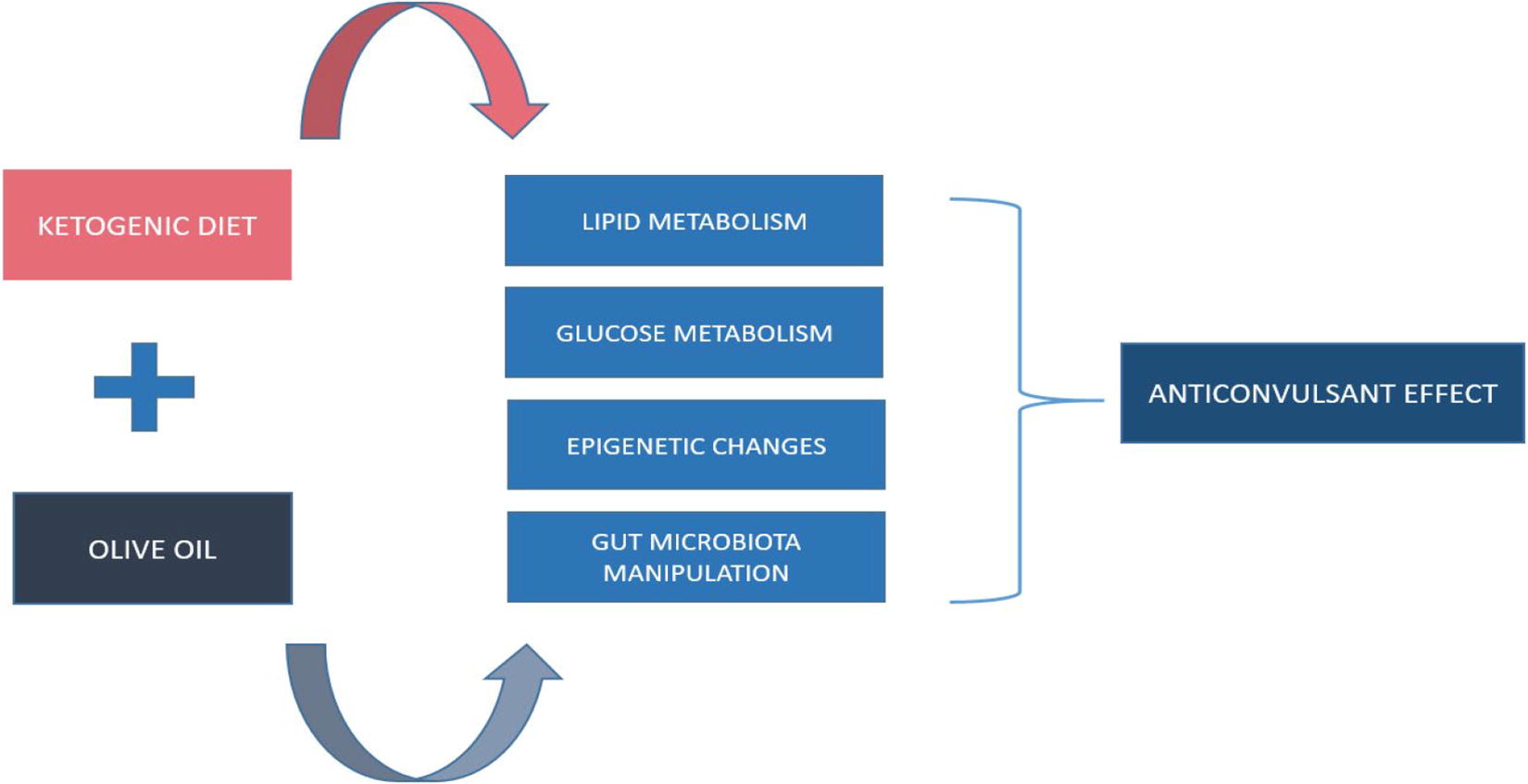
Potential olive oil involvement in ketogenic diet mechanisms in epilepsy.
KBs: production and actions
A high-fat KD favors fatty acid beta-oxidation and liver ketogenesis, producing KBs, such as BHB, acetoacetate, and acetone as an alternative to glucose energy substrate. These KBs can be used by the brain and other tissues for energy through oxidative phosphorylation. 7 KBs also enhance gamma-aminobutyric acid (GABA) synthesis in the brain, providing an anticonvulsant effect, as GABA is the primary inhibitory neurotransmitter. 41 Additionally, increased ATP production from KBs in the tricarboxylic acid cycle raises adenosine levels, which activate the inhibitory A1 receptor in the hippocampus and cerebral cortex, further contributing to anticonvulsant action. 42
The activation of PPARs is another mechanism contributing to the KD’s anti-seizure effects. PPARs are neuroprotective transcription factors involved in regulating anti-inflammatory, antioxidant, and mitochondrial genes. 43 Fatty acids from fat oxidation during KD serve as natural agonists for PPARs, particularly increasing PPARγ in the brain, which has anticonvulsant effects. 43
While KD is believed to be effective regardless of diet type or fatty acid composition, recent evidence suggests that fat type plays a significant role in KD efficacy. 7,43 MCT diets have been proven effective, and other fats, including olive oil, have shown clinical benefits in epileptic patients. 16,44 –46
Emphasizing olive oil and beyond epilepsy, Farràs et al. showed that oleic acid and the amount of olive oil polyphenols are linked to increased PPARγ expression in prehypertensive or hypertensive individuals. 47 In a recent review summarizing the effects of nutritional factors on PPAR expression, in vitro studies with olive oil underline the association of olive oil effect on inflammatory markers such as IL-1, tumor necrosis factor a, and nuclear factor kappa-B (NF-κB) and insulin regulation in patients with diabetes through PPARγ pathways. 48 –50 Hydroxytyrosol may also promote mitochondrial biogenesis through increased PPAR gene expression in obese and diabetic subjects. 51 Consequently, olive oil, by promoting PPAR expression, could serve as the main fat substrate in a KD, enhancing its anticonvulsant action through the PPAR pathway.
Alterations in glucose metabolism—KATP channels activation
As KD involves lowering dietary carbohydrates with a parallel decrease in blood glucose levels, it is supported that the regulation of glucose metabolism plays a role in KD action. Glucose restriction, together with lipid abundance during KD, promotes the selective activation of ATP-sensitive potassium (KATP) channels in neurons, which act as metabolic regulators and affect seizure activity. 7
Olive oil oleuropein and hydroxytyrosol have been found to participate in the secretion and action of insulin in studies in adult populations, offering an antidiabetic effect, so it could be advantageous in the context of KD, helping to control glucose homeostasis. 32,52
Epigenetic changes
Epigenetic alterations mediated by KD offer a new anti-epileptogenic potential of this diet. 53 In particular, changes in DNA methylation, histone acetylation, and non-coding RNA may affect gene expression in patients with epilepsy and are regulated by factors such as diet. 54 KD promotes the adenosine signaling in the brain, blocking DNA methylation, resulting in an antiepileptic effect, and the central role for these epigenetic alterations is attributed to KBs and especially BHB action. 42,55
Although KBs are produced during KD implementation independently from the type of fat, it could be important to examine the possibility of choosing olive oil as the main fat of the KD regime. Olive oil and its phenolic compounds are independently associated with epigenetic alterations through their anti-inflammatory, anti-cancer, and antioxidant actions in the context of chronic diseases in several human and animal studies. 56 Thus, olive oil could potentially be among the natural dietary elements targeting the epigenome of epileptic patients and acting synergistically with KD toward its anti-epileptogenic and anti-seizure effects.
KD PUFAs supply
The high-lipid content of the KD has long been debated since it may serve as a risk factor for CVD and metabolism disorders. KD lipid is derived from various food sources depending on the population’s dietary habits. In a Western diet, SFA form the main lipid content and are linked to a higher risk of CVD by affecting oxidative and inflammatory markers, endothelial cell functions, and gut microbiota. 57 In contrast, PUFAs, particularly n − 3 PUFAs, have been shown to improve brain health, supporting neuronal structure and function with neuroprotective and anti-inflammatory effects. 58
One of the mechanisms for KD action is the supply of PUFAs, which offer neuroprotection and lower neuron excitability through voltage-gated potassium channel opening. 59 It could be supposed that by offering more PUFAs with KD or even only PUFAs as a supplement, seizures would be reduced. This hypothesis has been the question in several animal and human studies with conflicting results. 60 –62 Therefore, PUFAs could be suggested as part of a KD rather than a supplement, helping to reduce the total amount of ingested SFA. Thus, a KD with a Mediterranean approach could benefit the number of seizures and cognition and behavior parameters, as already seen in several neurodegenerative disorders. 63
Olive oil, a key component of the MedDiet, contains PUFAs and offers additional benefits together with its phenolic compounds and MUFAs, contributing to KD’s anti-inflammatory, antioxidant, antidiabetic, and antimicrobial effects. 30
KD’s antioxidant and anti-inflammatory properties
Epileptogenesis, the process by which a normal brain can generate spontaneous recurrent seizures, is associated with the production of ROS and pro-inflammatory mediators. 64 These factors contribute to neuroinflammation, oxidative stress, and alterations in neuronal excitability and synaptic activity, increasing the likelihood of seizures. ROS can damage cellular structures and disrupt ion channel function. At the same time, pro-inflammatory cytokines can affect neurotransmitter systems, glial activation, and blood-brain barrier integrity, further exacerbating the pro-seizure environment. This complex interplay enhances brain excitability and fosters seizure development and maintenance. 65
The KD has been associated with reduced oxidative stress achieved by several mechanisms. KBs, especially BHB, mediate nuclear factor erythroid-derived 2-related factor 2 (Nrf2) activation and glutathione biosynthesis, and modulate the nicotinamide-adenine dinucleotide (NAD+/NADH) ratio. These actions reduce ROS production, protect mitochondria from oxidative stress, and provide general neuroprotection in epileptic patients. 54,66
Given the strong connection between epilepsy and inflammation, it is important to note that KD also has anti-inflammatory properties. It inhibits NF-κB and NOD-, LRR- and pyrin domain-containing protein 3 (NLRP3) inflammasome activation and activates PPARs. 5,43,66 –69
Olive oil and its components also exhibit anti-inflammatory and antioxidant properties. A recent review by Butt et al. details the neuroprotective role of oleuropein, highlighting its effects not only in epilepsy but also in other mental disorders such as Alzheimer’s, Parkinson’s, stroke, depression, and anxiety. 70 In an animal study using pentylenetetrazole-induced epilepsy in mice, oleuropein demonstrated antiepileptic effects, including anti-inflammatory action (reduction in IL-1b levels) and antioxidant capacity (free radical scavenger). 71 Thus, olive oil could serve as a natural adjunct to pharmacotherapy and KD in patients with epilepsy to prevent or reduce oxidative stress and neuroinflammation related to epilepsy.
Gut microbiota manipulation
Gut health highly depends on nutritional and environmental factors, with intestinal homeostasis playing a crucial role in disease response. The “gut-brain axis” mediates changes in brain metabolites following alterations in gut microbiota induced by specific diets or nutrients. 72 –74 Antibiotic treatment in drug-resistant epileptic patients has shown seizure freedom and subsequent recurrence after the cessation of treatment, highlighting the potential gut microbiota role in epilepsy management. 75 Additionally, anti-seizure medications appear to influence, or to be influenced by various gut microbial populations, as demonstrated in clinical and preclinical studies. 76,77
The KD efficacy in drug-resistant epileptic patients has been linked to changes in their gut microbiota, confirming the study contacted in mice by Olson et al. where certain gut populations act as mediators to the KD anti-seizure effects. 8,45,76,78 –81
High-fat diets have been shown to negatively influence the diversity and richness of gut microbiota, affecting the Firmicutes/Bacteroidetes (F/B) ratio toward dysbiosis. 82 Not only the quantity but also the quality of fat impacts gut microbiota populations. In mice given different fat types, such as palm oil, flaxseed/fish oil, and olive oil, it was demonstrated that olive oil and its MUFAs had a positive impact on commensal bacteria with a greater abundance of Bacteroidaceae compared with palm oil and flaxseed/fish oil fed groups. 83 Another study in mice resulted in favorable conclusions regarding olive oil’s beneficial effects on the gut microbiome compared with butter and their relation to parameters associated with metabolic syndrome. 84 In human studies, high-fat and SFAs diets have been shown to reduce microbiota diversity, while diets with lower amounts of total fats and more PUFAs are preferred for better metabolic health. 85
SCFAs, especially acetate, propionate, and butyrate, are important gut metabolites that influence neurotransmitter levels, blood-brain barrier integrity, and neural functions. 86,87 Although the high-fat content of KD can reduce SCFA production, adding foods like nuts, berries, and vegetables has been shown to increase SCFA levels. 88 Adding olive oil could be a further step toward this SCFA gut enrichment direction.
EVOO enhances beneficial gut populations, leading to reduced inflammation, increased antioxidant activity, improved immune function, and better intestinal integrity. These benefits are linked to positive outcomes for cardiovascular, metabolic, and cognitive health. 39,40 Polyphenols in EVOO modulate intestinal epithelium homeostasis, primarily through absorption in the small intestine and biotransformation by colonic bacteria, influencing microbiota composition in a dose-dependent manner. 38
Thus, using olive oil as the primary fat in KD could contribute to the control of epilepsy-related inflammation by preserving intestinal integrity and shaping gut microbiota, subsequently affecting neurotransmitter action through the “gut-brain axis.”
CONCLUSIONS
Olive oil and its unique constituents have been shown to offer multiple health benefits. Despite the limited reports about the association between olive oil and epilepsy, it appears that olive oil and the KD, in the context of the MedKD, could act synergistically to achieve antiepileptic effects. Οlive oil also offers the alternative of a fat type admitted to be healthier than other fats that are rich sources of SFA, such as those widely used in KD regimes.
The promising field of gut microbiota manipulation by specific foods, such as olive oil, presents a future perspective for adopting MedKD for epilepsy. Further clinical studies are required to investigate the precise role of olive oil and its components in anti-epileptogenesis and seizure protection when implementing KD, or as a natural non-pharmacological supplement for epileptic patients, with clearly defined dose recommendations. At the moment, olive oil could be part of KD regimes following the Mediterranean style, not only for populations with existing Mediterranean dietary habits but also for those who can access it and benefit from its properties.
Footnotes
AUTHORS’ CONTRIBUTIONS
S.Z.: Conceptualization, writing—original draft. M.Y.: Methodology, writing—review and editing; A.A.: Methodology, supervision. S.F.: Methodology, supervision. E.K.M.: Editing. A.K.: Methodology, supervision. A.D.: Supervision.
AUTHOR DISCLOSURE STATEMENT
All authors declare no conflict of interest.
FUNDING INFORMATION
There is no external funding for this review.