
Abstract
Abstract
Purpose:
The aim of this study was to compare the efficacy of bimatoprost 0.03% with brimonidine 0.2% in preventing intraocular pressure (IOP) elevations after neodymium:yttrium–aluminum–garnet (Nd:YAG) laser posterior capsulotomy.
Methods:
In this prospective, randomized, double-masked study, 195 eyes of 195 consecutive patients who had YAG laser capsulotomy for posterior capsule opacification were recruited. Eyes received either 1 drop of bimatoprost 0.03% (98 patients) or brimonidine 0.2% (97 patients) at 1 h before laser surgery. A masked observer measured IOP by Goldmann applanation tonometry before treatment and after treatment at 1 h, 3 h, 24 h, and 7 days. Inflammation was evaluated after surgery. Formation of cystoid macular edema was assessed by measuring the macular thickness before and after laser surgery.
Results:
The average peak of postoperative IOP elevation was 2.2 ± 3.9 mm Hg in the bimatoprost 0.03% and 3.6 ± 3.1 mm Hg in the brimonidine 0.2% group. The difference was statistically significant (P < 0.001). Postoperative IOP elevations of 10 mm Hg or more occurred in 1 eye (1.56%) in the bimatoprost 0.03% group and 5 eyes (7.35%) in the brimonidine 0.2%. This difference was statistically significant (P < 0.001). Macular edema and anterior chamber reaction were not observed related to bimatoprost. No clinically significant side effects were noted in either group.
Conclusions:
Our results indicate that prophylactic use of bimatoprost 0.03% is more effective than brimonidine 0.2% in preventing IOP elevation immediately after YAG laser capsulotomy. Bimatoprost 0.03% as a prostamide analog may provide new option for preventing IOP elevation after YAG laser capsulotomy.
Introduction
The prostaglandin analogs are a widely used class of medication, often as first-line therapy, for the treatment of glaucoma and ocular hypertension. Bimatoprost 0.03% (Lumigan; Allergan) is a highly efficacious ocular hypotensive agent that provides good diurnal control of IOP in glaucoma and ocular hypertensive patients.13–15 Bimatoprost is a synthetic molecule that is structurally and pharmacologically similar to prostamide F2α and appears to mimic the activity of the prostamides. Bimatoprost is the most efficacious ocular hypotensive agent currently available for the treatment of glaucoma.13–15 Clinical studies have shown that even a single dose of bimatoprost causes a significant reduction in IOP.13,14
To our knowledge, so far there are no published reports of the effectiveness of bimatoprost 0.03% as a prostamide analog in preventing IOP elevation after YAG laser capsulotomy. This study evaluated the effectiveness and safety of bimatoprost 0.03% versus brimonidine 0.2% as the current drug of choice in preventing IOP elevation after YAG laser capsulotomy.
Methods
This prospective, randomized, double-masked clinical trial enrolled 195 patients having YAG laser posterior capsulotomy at the İstanbul Bilim University Ophthalmology Department between February 2006 and October 2008. Study enrollment was comprised of consecutive clinic patients. Patient data included age, sex, and race. Only 1 eye in each patient was enrolled for study. Patients were randomized to receive brimonidine 0.2% (n = 97) or bimatoprost 0.03% (n = 98) at ∼1 h before laser surgery. Randomization was performed using the order of entrance in the study, with alternate assignment to bimatoprost 0.03% and brimonidine 0.2% groups.
The research followed the tenets of the Declaration of Helsinki, and all patients signed informed consent after they received an explanation of the nature and possible consequences of the procedure. Institutional review board approval was also obtained.
All patients had complete baseline eye examinations including best corrected Snellen visual acuity, slit lamp biomicroscopy, and fundus examination. The baseline IOP was measured by Goldmann applanation tonometry at ∼3 h before the laser procedure. Formation of cystoid macular edema was assessed by measuring the macular thickness before and after laser surgery. Macular thickness was measured by optical coherence tomography (SLO-OCT, Oti, Canada). Patients were excluded if they had previous ocular laser treatment and surgery. Patients were also excluded if they had glaucoma, had active inflammation or infection, had unstable cardiovascular disease, were <21 years of age, were taking systemic clonidine or topical apraclonidine or brimonidine, systemic or topical prostaglandin analogs, and nonstreoid anti-inflammatory drugs.
To qualify for YAG capsulotomy, they had to have visually significant
IOP, heart rate, blood pressure, and any adverse reactions were recorded at 1 h, 3 h, and 24 h, and 1 week after the laser treatment. Postlaser measurements of IOP were done by the physician who measured the IOP prelaser. The patient and the physician measuring the IOP were unaware of the treatment assignment. If at any point an unacceptable IOP elevation was observed, the patient would have received other IOP-lowering medication(s) as needed and would have been removed from the study. A postoperative IOP elevation was considered unacceptable if it was thought to be potentially harmful for that patient's degree of optic nerve cupping or degree of visual field loss. IOP outcome measures were grouped into the following categories: postlaser IOP elevation of 5 to <10 mm Hg, and postlaser IOP elevation of 10 mm Hg or more. IOP elevation of <5 mm Hg was not considered a clinically significant change. The rate of uveitis flares was calculated before and after the initiation of bimatoprost therapy. Inflammation was graded using the evaluation system as defined by Foster and Vitale for the anterior chamber cells and flare, 0–4 in gradations of 0.5; 0.5 or less was considered inactive. 16
Statistical analysis was performed using SPSS software for Windows version 15.0 (SPSS, Chicago, IL). Results were expressed as mean ± standard deviation. Statistical analyses included Student's t-test and chi-square (or Fisher exact) test where appropriate. Multiple-comparison correction (Bonferroni correction) was used. Results were significant if P < 0.05; P values were for 2-sided tests. Sample size calculations revealed that this study had >95% power to detect a 4 mm Hg difference in IOP between the 2 groups.
Results
The 2 groups were not statistically different in terms of demographics. The mean age was 68.6 ± 12.4 years in the bimatoprost 0.03% group and 66.2 ± 12.2 years in the brinzolamide 0.2% group (P = 0.5). There were 52 women and 46 men in bimatoprost 0.03% group, and 49 women and 48 men in the brimonidine 0.2% group. The mean amount of energy used for YAG capsulotomies was 44.3 ± 18.4 mJ in the bimatoprost 0.03% group and 40.7 ± 21.4 mJ in the brimonidine 0.2% group. The difference between groups was not statistically significant (P = 0.2).
Between the bimatoprost 0.03% and the brimonidine 0.2% groups, the baseline and all subsequent IOPs measured at each follow-up were not statistically different. The mean IOP before surgery on the day of the procedure was 15.4 ± 3.2 mm Hg in the bimatoprost 0.03% group and 14.8 ± 4.0 mm Hg in the brimonidine 0.2% group (P = 0.8). Changes in IOP after laser treatment were measured. The average postoperative peak IOP elevation was 2.2 ± 3.9 mm Hg in the bimatoprost 0.03% group and 3.6 ± 3.1 mm Hg in the brimonidine 0.2% group. This difference was statistically significant (P < 0.001). The mean IOP changes from baseline were shown in 2 groups at 1 h, 2 h, 3 h, and 7 days (Fig. 1). In all 195 patients in both groups, postoperative IOP elevations occurred in 132 of 195 patients (67.6%). Of the 132 patients who had postoperative IOP elevations, 64 patients were treated with bimatoprost 0.03% and 68 patients were treated with brimonidine 0.2%. Their peak postoperative IOP elevations occurred at 1 h in 32.5% (43/132), at 3 h in 25% (33/132), at 24 h in 21.2% (28/132), and at 1 week in 21.2% (28/132). Table 1 shows the overall incidence of IOP elevations over the entire length of follow-up.
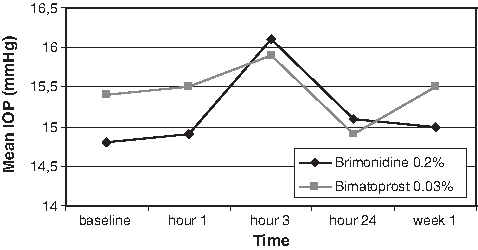
Mean intraocular pressure (IOP) changes over time.
Abbreviation: IOP, intraocular pressure.
Including all time points after laser treatment, postoperative IOP elevations of 5 to <10 mm Hg occurred in 17.18% of eyes (n = 11) in the bimatoprost 0.03% group and 19.11% of eyes (n = 13) in the brimonidine 0.2% group. This was not statistically different (P = 0.6). Of the 24 patients who had postoperative IOP elevations of 5 to <10 mm Hg, 6 (25.0%) had their peak postoperative IOP elevations at 1 h, 10 (41.6%) at 3 h, 2 (8.3%) at 24 h, and 6 (25.0%) at 1 week. IOP elevations of 10 mm Hg or more on at least 1 postoperative IOP measurement throughout the study occurred in 1 eye (1.56%) in the bimatoprost 0.03% group and 5 eyes (7.35%) in the brimonidine 0.2% group. The difference was statistically significant (P < 0.001). Of the 6 patients who had postoperative IOP elevations of 10 mm Hg or more, 1 (16.6%) had their peak postoperative IOP elevations at 1 h, 3 (50%) at 3 h, 1 (16.6%) at 24 h, and 1 (16.6%) at 1 week. Macular thickness changes from baseline were also not statistically significant in either group at any time (Fig. 2). The average postoperative increase of macular thickness was 7.0 ± 3 μm in the bimatoprost 0.03% group and 10 ± 5 μm in the brimonidine 0.2% group (P = 0.9). The bimatoprost 0.03% and brimonidine 0.2% treatments were not associated with noticeable change in intraocular inflammatory response. Anterior chamber reaction was scored 0–0.5 in either group. No eye had an IOP elevation higher than 24 mm Hg. No patient had a postoperative IOP elevation that was high enough to warrant either treatment or removal from the study. There were no local allergies or side effects including those reported by any patients in either group.

Mean macular thickness changes over time.
Discussion
PCO can be effectively treated with a YAG laser capsulotomy. 2 However, this procedure can result in significant morbidity arising from postoperative complications. These include transient immediate postoperative IOP elevation, new onset of glaucoma, and worsening of preexisting glaucoma. The acute IOP elevation that follows YAG laser capsulotomy procedure is relatively common and may be harmful.2–5
This study compared 1 drop of bimatoprost 0.03% with 1 drop of brimonidine 0.2% given at ∼1 h before laser treatment. This study evaluated IOP elevation after laser surgery at around 3 h because numerous studies have shown that IOP elevation after laser procedures commonly occur in the first 3 h.7–10 Because the maximal effect of brimonidine 0.2% and bimatoprost 0.03% is at about 1–4 h, the maximum effect of the premedication should coincide with the peak IOP elevation after laser surgery.7–9,13,14 Of the 24 patients who had postoperative IOP elevations of 5 to <10 mm Hg, 10 (41.6%) patients had their peak postoperative IOP elevations at 3 h. Of the 6 patients who had postoperative IOP elevations of 10 mm Hg or more, 3 (50%) had their peak postoperative IOP elevations within 3 h. The number of eyes with an IOP increase higher than 5 or <10 mm Hg was not significant at any examination in either group. But the number of eyes with an IOP increase higher than 10 mm Hg was significantly higher in the brimonidine 0.2% group. The systemic changes in this study were not clinically significant in that no patient fainted or needed treatment for blood pressure changes.
The importance of prophylaxis for IOP spike attributable to YAG laser capsulotomy can be seen when reviewing YAG laser capsulotomy complications in the peer-reviewed literature.2–12 The current drugs of choice for prophylaxis of postoperative IOP rise are brimonidine 0.2% and apraclonidine 0.5% and the medications appear to have almost equal efficacy.8–11 Brimonidine is more selective for α-2 versus α-1 receptors than apraclonidine.8–10,12 Thus, side effects are presumably related to α-1 activity such as mydriasis, eyelid retraction, conjunctival blanching, ciliary asoconstriction, decrease in conjunctival oxygen tension, and dry nose and mouth, which occur minimally during brimonidine medication.9,10,17 Therefore, these features provide the rationale for treating IOP spike after YAG laser with brimonidine 0.2% as a first choice versus apraclonidine 0.5%. Nonetheless, there have been reports of systemic adverse effects of brimonidine 0.2%, including apparent central nervous system depression.16,17 Further, brimonidine 0.2% has a potential side effect on pupil size.18,19 Brimonidine 0.2% solution stimulates prejunctional α-2 agonist receptors, resulting in a reduction of norepinephrine release in the synapse. Norepinephrine contraction of the dilator muscles through an α-1 receptor is subsequently decreased, resulting in miosis.20–22 One drop of brimonidine 0.2% in the normal eye effectively decreased scotopic pupil size within 30 min. This decrease of 1.0 mm or more has the potential to alleviate some vision problems in dim lighting and darkness after laser surgery. 20 This has led clinicians to search for a more effective prophylaxis alterative that is less likely to cause side effects.
Bimatoprost 0.03% is a synthetic prostamide analog.23–30 Bimatoprost, unlike latanoprost, does not require conversion to an active metabolite to exert its pharmacologic activity. Its IOP-lowering activity is related to enhancement of both uveoscleral and trabecular outflow.13,14,23–30 The prostamide F2α analog bimatoprost 0.03% is the most efficacious ocular hypotensive agent currently available for the treatment of glaucoma.13–15,23–30 Clinical studies have shown that even a single dose of bimatoprost causes a significant reduction in IOP.13,24,25 Brimonidine 0.2% also reduces IOP by reducing aqueous production and increasing uveoscleral outflow. However, the uveoscleral outflow effect occurs only with prolonged treatment.8,9,11 Some meta-analysis reported that highest reduction of IOP was achieved by bimatoprost, followed by latanoprost, travoprost, and timolol–dorsolamide fix combination.29,30 Macular edema, eye infections, and allergic reactions are rare but potentially serious side effects of bimatoprost. And yet, in our study, we did not encounter any side effect possibly related to bimatoprost 0.03%, including hyperemia, allergic reactions, or macular edema. A recent published study suggested that bimatoprost is an effective IOP-lowering agent even in patients with uveitic glaucoma. 31 Another current published study was conducted to determine the efficacy of bimatoprost 0.03% drops given preoperatively in preventing IOP rise following phacoemulsification cataract surgery. Prophylactic use of 1 drop of bimatoprost before phacoemulsification cataract surgery was found effective in preventing IOP rise without any side effect. 32 Thus, it would be expected that bimatoprost 0.03% may also be an effective and safe prophylactic agent in preventing IOP spike. In concordance with this prescience, the results of our study show that the average peak of postoperative IOP elevation was significantly lower in the bimatoprost 0.03% than the brimonidine 0.2% group. Further, bimatoprost 0.03% is more effective than brimonidine 0.2% in preventing IOP spike, especially >10 mm Hg, secondary to YAG laser posterior capsulotomy. The difference failed to reach statistical significance in IOP spike <10 mm Hg. This difference of lowering effect can be explained by the IOP-lowering effect of bimatoprost, which may be more pronounced at high pressures than brimonidine. Moreover, instillation of these drugs did not completely prevent postlaser IOP spikes. No incidents of significant ocular and systemic side effects were noted in either group. In the present study, prophylactic use of bimatoprost 0.03% was found to be very effective in lowering IOP in patients who underwent YAG laser capsulotomy.
To the best of our knowledge, our study is the first prospective, comparative study to indicate the effectiveness of bimatoprost as a synthetic prostamide analog in preventing IOP spike after YAG laser capsulotomy. Our results also reveal that bimatoprost 0.03% may provide a new option for preventing IOP elevation associated with YAG laser capsulotomy without significant side effects. A larger prospective study should be done to better define the effectiveness of bimatoprost.
Footnotes
Author Disclosure Statement
The authors have no financial or proprietary interest in any material or method mentioned in this article.