
Abstract
Abstract
Purpose:
To report a case of acute renal failure after topical fortified gentamicin and vancomycin eyedrops in the treatment of endophthalmitis.
Methods:
A 67-year-old lady with diabetes mellitus was treated for bleb-related endophthalmitis. After intravitreal antibiotics, she was given oral ciprofloxacin, fortified gentamicin, and vancomycin eyedrops. She developed acute renal failure a few days after therapy. Blood tests and ultrasound of the urinary system were performed to investigate for the cause of the renal failure.
Results:
No apparent cause of renal failure could be identified in our patient. Autoimmune markers and ultrasound of the urinary system were unremarkable. Fortified gentamicin and vancomycin eyedrops were stopped on day 9 and 13, respectively. The renal function recovered dramatically. The gentamicin level was checked 2 days after it had been stopped, and the serum level was 0.34 mg/L. Renal function improved on supportive management without dialysis. Serum creatinine level completely normalized 2 months later.
Conclusions:
This is the first article that demonstrated a detectable level of serum gentamicin level after usage of topical eyedrops. This is also the first article demonstrating that nephrotoxicity of topical fortified gentamicin and vancomycin eyedrops was found. The acute renal failure in our patient recovered completely after cessation of the eyedrops.
Case Report
Aqueous and vitreous tapping of the left eye was performed, and intravitreal antibiotics (Amikacin 0.4 mg and Vancomycin 1 mg) were given. Postoperatively, she was treated with 750 mg BD of oral ciprofloxacin, topical fortified gentamicin (14 mg/mL), and fortified vancomycin (31 mg/mL) hourly.
She reported nausea and poor appetite since postoperative day 4 with vomiting on day 6. Acute kidney injury (AKI) was found after performing blood tests and recording the urine output. Her renal function, which had been normal in the past, was found to be severely deranged with serum urea 27.2 mmol/L and serum creatinine 551 μmol/L. She was also found to have oliguria of 250 mL in 24 h on day 7. According to the RIFLE classification for AKI, 1 she suffered from acute kidney failure.
Ultrasound of urinary system was unremarkable. Repeated urinalysis showed no evidence of nephritic or nephrotic syndrome. Urine output was normalized after intravenous fluid, but her renal function further deteriorated with metabolic acidosis. Other laboratory tests for causes of acute renal failure such as hepatitis markers, autoimmune markers, and paraproteins were found negative.
Her systemic medications were also reviewed for any possible adverse effect on renal function. Earlier, she had been on 7.5 mg BD of glibenclamide, 500 mg TDS of metformin, and a combination of 5 mg of amiloride with 50 mg of hydrochlorothiazide daily. The first 2 medications were given for only 3 days, as she was switched to an insulin sliding scale due to poor oral intake. The antihypertensive was given for only 2 days, as her blood pressure was not high. These medications were believed to have no significant nephrotoxic effect on her and their duration was short. There were no nonprescription or herbal medicines, as she was treated as in-patient and she denied any intake of herbal medicines.
Her renal function continued to deteriorate with 39.3 mmol/L of serum urea and 748 μmol/L of serum creatinine on day 9. In view of poor renal function, oral ciprofloxacin and topical fortified gentamicin were stopped on day 9. Interestingly, the renal function started to recover in the next 2 days with the serum creatinine level down to 668 μmol/L on day 11. AKI caused by gentamicin was retrospectively suspected, and the gentamicin level was checked 2 days after it had been stopped. Its serum level was 0.34 mg/L (Reference trough level <2.1 mg/L). Her recovery of renal function was slow in the next few days with serum creatinine level maintained at around 650 μmol/L. However, after the cessation of fortified vancomycin on day 13, her renal function further improved dramatically (see Fig. 1). The vancomycin level that was checked on the day it was stopped was <0.6 mg/L (Reference trough level: 10.1 mg/L). She declined renal biopsy. Her renal function improved on supportive management without dialysis and was completely normalized 3 months postoperatively with serum creatinine returned to 96 μmol/L.
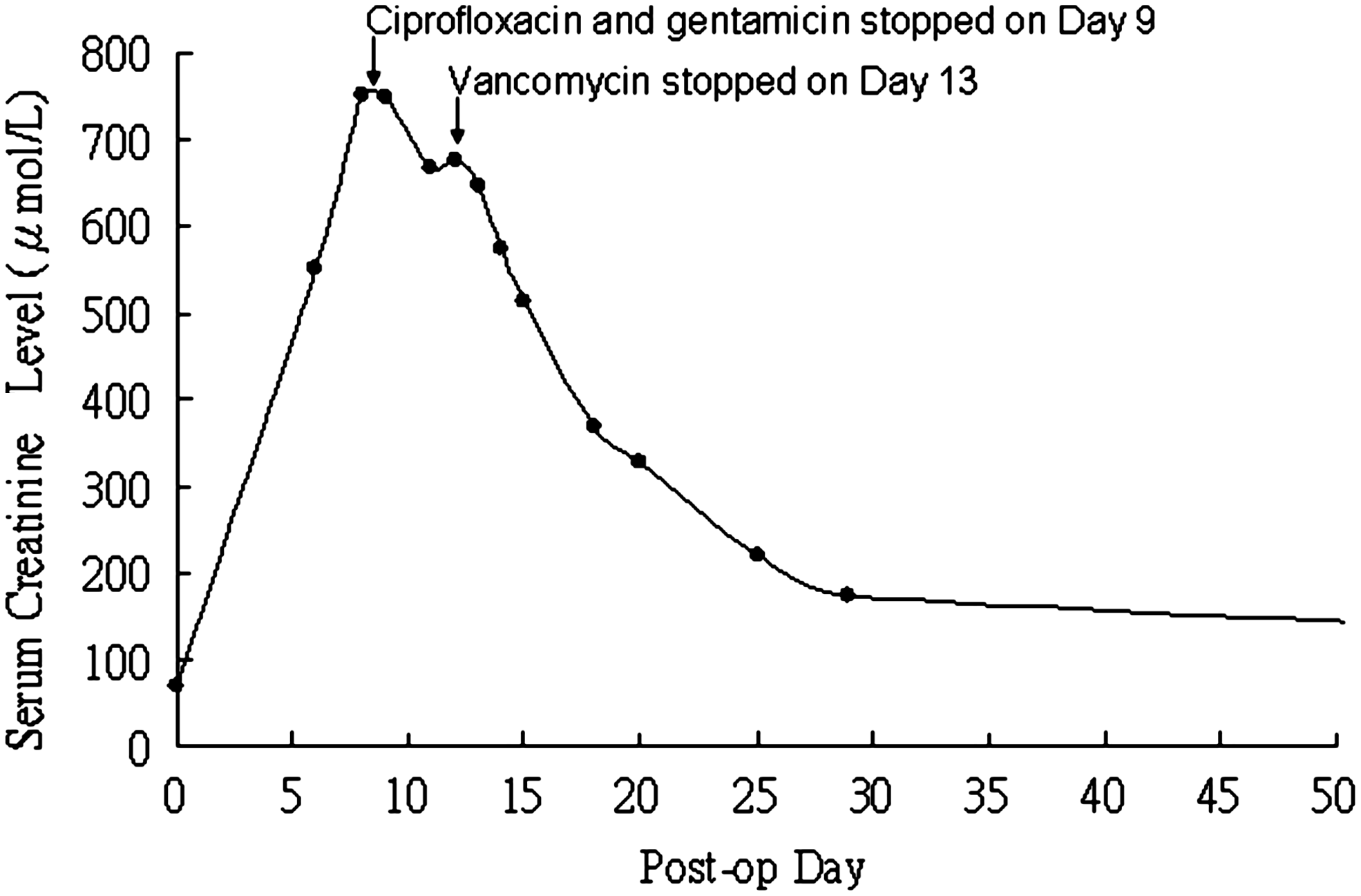
Curve showing the relationship between the serum creatinine level and the postoperative day after intravitreal antibiotics. Oral ciprofloxacin, topical fortified gentamicin eyedrops, and fortified vancomycin eyedrops were started after the operation. The time of their cessation is indicated by the arrows.
Discussion
The cause of AKI was investigated in our patient. Ultrasound, blood tests, and urinalysis failed to identify any renal or postrenal causes. It is, therefore, suspected that the AKI was caused by drug toxicity. Acute renal failure after ciprofloxacin has been reported, but review shows that it is actually rare. The rate of all kinds of urinary tract-related adverse reactions of ciprofloxacin ranged from 0.2% to 1.3% only. 2 The nephrotoxicity of ciprofloxacin appears to be an idiosyncratic response in a susceptible individual, rather than a general phenomenon which is seen in gentamicin. Our patient did not have eosinophilia on blood test or crystalluria in urinalysis, as seen in some reported cases of renal failure after ciprofloxacin. Therefore, the likelihood of ciprofloxacin-induced nephrotoxicity is low. Besides, we can observe a double-peak pattern in the creatinine curve (Fig. 1). The second peak of serum creatinine level that drops after cessation of topical vancomycin eyedrops could not be explained by the toxicity of oral ciprofloxacin alone. A strong temporal relationship of renal function recovery after cessation of topical gentamicin and vancomycin eyedrops was observed. These agents, being well-known to be nephrotoxic if given systemically, were likely to play a significant role.
Although reports on topical gentamicin causing acute renal failure do exist,3,4 there has not been any report relating to topical gentamicin or vancomycin eyedrops and acute renal failure. The attempt to demonstrate high serum levels of either gentamicin or vancomycin in our patient also failed. Nevertheless, this does not rule out the possibility of nephrotoxicity caused by them. Serum half-life of gentamicin has been reported to vary greatly from 0.4 to 24 h in different individuals. 5 Therefore, a level much higher than our measured value can be expected before gentamicin eyedrops were stopped. Besides, studies have shown that the toxic effect of gentamicin was dependent on the nonlinear accumulation of the drug in the renal cortex which can be saturated, as represented by the area under curve rather than the trough or peak serum level.5–7 Therefore, a high dosing frequency of topical gentamicin may produce a low but sustained serum level, which can be paradoxically more nephrotoxic than expected.
It is also worth pointing out that in contrary to a previous small-scale study by Trope et al., 8 which concluded that gentamicin eyedrops cause an undetectable serum level, we did identify a significant systemic drug level. Similarly, systemic absorption of gentamicin eardrops has also been reported in literature. 9 Other risk factors contributing to increasing the susceptibility of gentamicin nephrotoxicity in our patient include dehydration, female sex, old age, and concomitant use of aminoglycoside with vancomycin. 10
In conclusion, systemic absorption of gentamicin and vancomycin eyedrops can be significant, and nephrotoxicity is possible in susceptible patients. They are frequently used in the treatment of severe ocular infections.11,12 Clinicians should be aware of the early symptoms of azotemia in a patient given intensive nephrotoxic antibiotic eyedrops, and they should monitor renal function if necessary.
Footnotes
Author Disclosure Statement
The author has no financial interest in any product mentioned in this article.