
Abstract
Abstract
Purpose:
Brimonidine, an alpha-2 adrenoceptor agonist, is an effective and safe medication that is widely used in glaucoma treatment. Although it is known that it is quickly taken up by the cornea following topical administration and that the cornea has alpha-2 adrenoceptors, there are only few studies available on the impact brimonidine has on the cornea.
Methods:
Twenty healthy test persons (12 female and 8 male subjects)—mean age about 33 years (22 to 38 years)—were tested in a double-blind, prospective, randomized study. Intraocular pressure as well as epithelial, stromal, and endothelial thickness was measured before, at 25 days while, and at 5 days after administration of brimonidine 0.1% eye drops twice daily. To check the impact of this medication, placebo (proper solution of preservative) eye drops were administered to the other eye twice daily.
Results:
Administration of brimonidine 0.1% resulted in a reduction of intraocular pressure from an initial value of 14 to 9 mmHg after 5 days (P=0.001) as well as an increase in total corneal thickness from 556 μm from the time of the baseline examination to 578 μm (P=0.001), an increase of epithelial thickness from 58 to 66 μm (P<0.001), and stromal thickness from 488 to 502 μm (P=0.008) after 2 days each. Another 2 days later, total corneal thickness was 559 μm (P=0.276), epithelial thickness 56 μm (P=0.561), and stromal thickness 493 μm (P=0.315), which means that the values had returned more or less toward the initial values measured. In contrast, endothelial thickness did not vary following administration of brimonidine 0.1% (P=0.965). With treatment with brimonidine 0.1%, mean intraocular pressure in thin corneas (<556 μm) was lower than in the thick corneas (>556 μm, P=0.018).
Conclusions:
Topical administration of brimonidine 0.1% results in a reversible increase in corneal thickness. The question whether this increase is of clinical significance and whether it is the result of epithelial and/or endothelial receptor stimulation cannot be finally answered at the present time.
Introduction
This is all the more amazing, because proof of the presence of alpha-2 adrenoceptors in corneal epithelial and endothelial cells has been furnished. The stimulation of these adrenoceptors by brimonidine resulted in a decrease in intracellular cAMP concentration and thus reduced proteinkinase A (PKA) activity.6,7 Blocking of corneal beta adrenoceptors, which also comes along with a reduction of intracellular cAMP concentration and a reduction of PKA activity, resulted in a measurable increase in central corneal thickness.6–8
The aim of the present study was to find out (1) whether topical administration of brimonidine results in interaction with corneal alpha-2 adrenoceptors in terms of an increase in corneal thickness and (2) whether there is any difference between the response of corneal epithelium, stroma, and endothelium to this interaction.
Methods
Twenty healthy test persons (12 female and 8 male subjects)—mean age 33 years (22–38 years)—were tested in a double-blind, prospective study. All test persons had a normal ophthalmologic history. Persons with serious medical or neurologic conditions and/or regular use of local or systemic medications were excluded from the study. All test persons gave consent to participate in this study and were informed about the purpose of and procedure applied to the study and also about the fact that they could stop participating at any time without stating any reason for stopping. The requirements postulated in the Declaration of Helsinki were strictly observed (Clinical Trails Registration Reference No. NCT01250236).
Baseline examination of the test persons was carried out at 08:00 h and included taking their individual medical histories as well as a vision test plus slit-lamp micro-ophthalmoscopy, funduscopy, spectral optical coherence tomography (SOCT) of the anterior eye section, and at last, intraocular pressure testing. Then these were followed by randomized administration of brimonidine 0.1% eye drops (Alphagan P; Allergan, Irvine, CA; brimonidine tartrate 0.1%, PURITE 0.005% as a preservative, sodium carboxymethylcellulose, sodium borate, boric acid, sodium chloride, potassium chloride, calcium chloride, magnesium chloride, purified water, and hydrochloric acid and/or sodium hydroxide), a commercial medication used in glaucoma treatment, to 1 eye (n=20) and administration of placebo eye drops (Cellufresh; Allergan, Irvine, CA; PURITE 0.005% as a preservative and sodium carboxymethylcellulose) to the other eye (n=20). SOCT and intraocular pressure testing were repeated 10 min later. The test persons were requested to continue to take both eye drops for 25 days twice daily (08:00 and 20:00 h). Follow-up SOCTs and intraocular pressure testing were carried out in the morning hours of all subsequent 30 days. All tests and checks as well as the analyses of the SOCT scans were performed by only 1 examiner.
To determine corneal thickness and thickness of its individual layers, central axial scans of SOCT (Copernicus; EyeTec, Lübeck, Germany), which measure corneal thickness with an accuracy of 5 μm, were used. 9 Foveal fixation was used for centering the scan and automatic corneal mapping was used to prove centering. Two manual measurements were taken at 1-min intervals. Intraocular pressure was measured with a Goldmann applanation tonometer. Again, 2 measurements were taken at 1-min intervals. The mean value of the 2 SOCT and tonometry measurements was used for statistical evaluation. Jump (SAS, Cary, NC) was used to calculate and visualize the values measured for corneal thickness and intraocular pressures. Statements regarding their significance were made using the ANOVA test.
Results
Regular administration of brimonidine 0.1% eye drops twice daily resulted in a consecutive increase of central corneal thickness from 556±6 μm (range: 543–560 μm) during the period from the baseline examination to 578±13 μm at the follow-up examination at 2 days later (P=0.001). Compared with the placebo group, this corresponds to an increase in central corneal thickness in the active drug group by 4% (P<0.001). However, in the course of the subsequent 2 days, central corneal thickness returned to 559±9 μm, which is almost the same value measured at the time the baseline examination was carried out (P=0.276). On the other hand, corneal thickness on administration of placebo eye drops did not vary from the time the baseline examination with a measured value of 553±17 μm was carried out to the last examination at 30 days later with a measured value of 555±26 μm (P=0.944; Fig. 1).

Central corneal thickness before (day −1), while (days 0–25), and after (days 26–30) application of brimonidine 0.1% (verum) eye drops in 1 eye (n=20) and placebo eye drops in the partner eye (n=20).
Assessment of the corneal epithelium alone also revealed an increase in thickness from 58±6 μm at the time of the baseline examination to 66±5 μm on the second day (P<0.001) on regular administration of brimonidine 0.1% eye drops twice daily. In the course of the subsequent 2 days, epithelial thickness again returned to almost the same level as the initial value measured (56±6 μm; P=0.561). Mean increase in epithelial thickness was 14% (P<0.001) in the active drug group compared with the placebo group. In contrast, epithelial thickness did not vary during the period from the time of the baseline examination with a measured value of 56±4 μm to the last examination at 30 days later with a measured value of 54±3 μm (P=0.118) on administration of placebo eye drops (Fig. 2).

Epithelial thickness before (day −1), while (days 0–25), and after (days 26–30) application of brimonidine 0.1% (verum) eye drops in 1 eye (n=20) and placebo eye drops in the partner eye (n=20).
Corneal stroma also showed an increase in thickness from 488±10 μm at the time of the baseline examination to 502±10 μm at 2 days later (P=0.008) on regular administration of brimonidine 0.1% eye drops twice daily. Another 2 days later there was only a marginal variance with a measured value of 493±11 μm (P=0.315) compared with the baseline examination. The increase in stromal thickness on the second day was 3% in the active drug group compared with the placebo group (P<0.001). The latter showed no variance on administration of placebo eye drops during the period from the baseline examination with a measured value of 488±15 μm to the last examination at 30 days later with a measured value of 492±24 μm (P=0.725; Fig. 3).

Stromal thickness before (day −1), while (days 0–25), and after (days 26–30) application of brimonidine 0.1% (verum) eye drops in 1 eye (n=20) and placebo eye drops in the partner eye (n=20).
Corneal endothelium showed no increase in thickness, neither on regular administration of brimonidine 0.1% eye drops twice daily (P=0.479) nor on administration of placebo eye drops (P=0.684). In addition, there was no difference between the active drug group and the placebo group (P=0.965; Fig. 4).
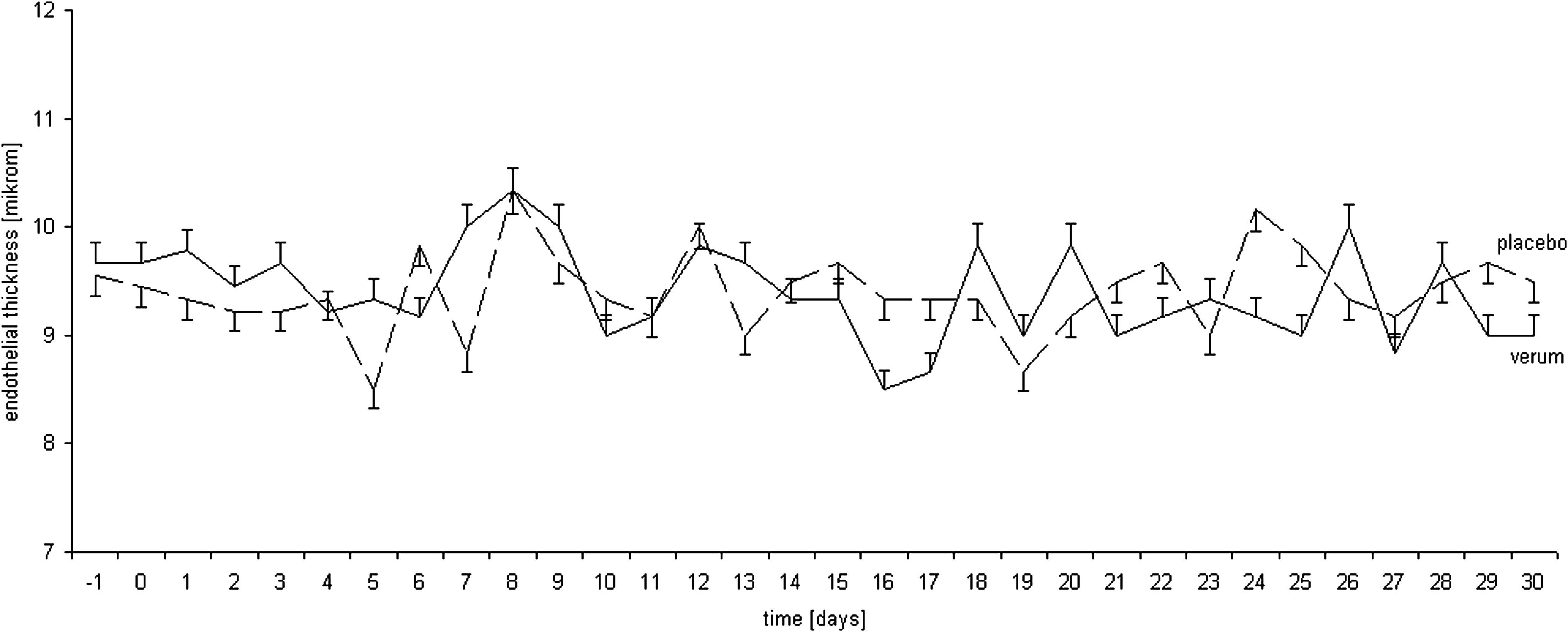
Endothelial thickness before (day −1), while (days 0–25), and after (days 26–30) application of brimonidine 0.1% (verum) eye drops in 1 eye (n=20) and placebo eye drops in the partner eye (n=20).
Regular administration of brimonidine 0.1% eye drops twice daily resulted in a reduction of intraocular pressure from an initial value of 14±3 to 13±2 mmHg (day 0, P=0.026), 12±3 mmHg after 1 day (P=0.005), 12±3 mmHg after 2 days (P=0.002), 11±3 mmHg after 3 days (P=0.001), 11±3 mmHg after 4 days (P=0.001), and 9±1 mmHg after 5 days (P=0.001). Mean pressure reduction was 36% (P<0.001) in the active drug group compared with the placebo group. After administration of brimonidine 0.1% was stopped on day 26, intraocular pressure returned to almost the same level as the initial value measured (day 30, 13±1 mmHg, P=0.661). In contrast, there was no variance in intraocular pressure on administration of placebo eye drops twice daily (P=0.962; Fig. 5).
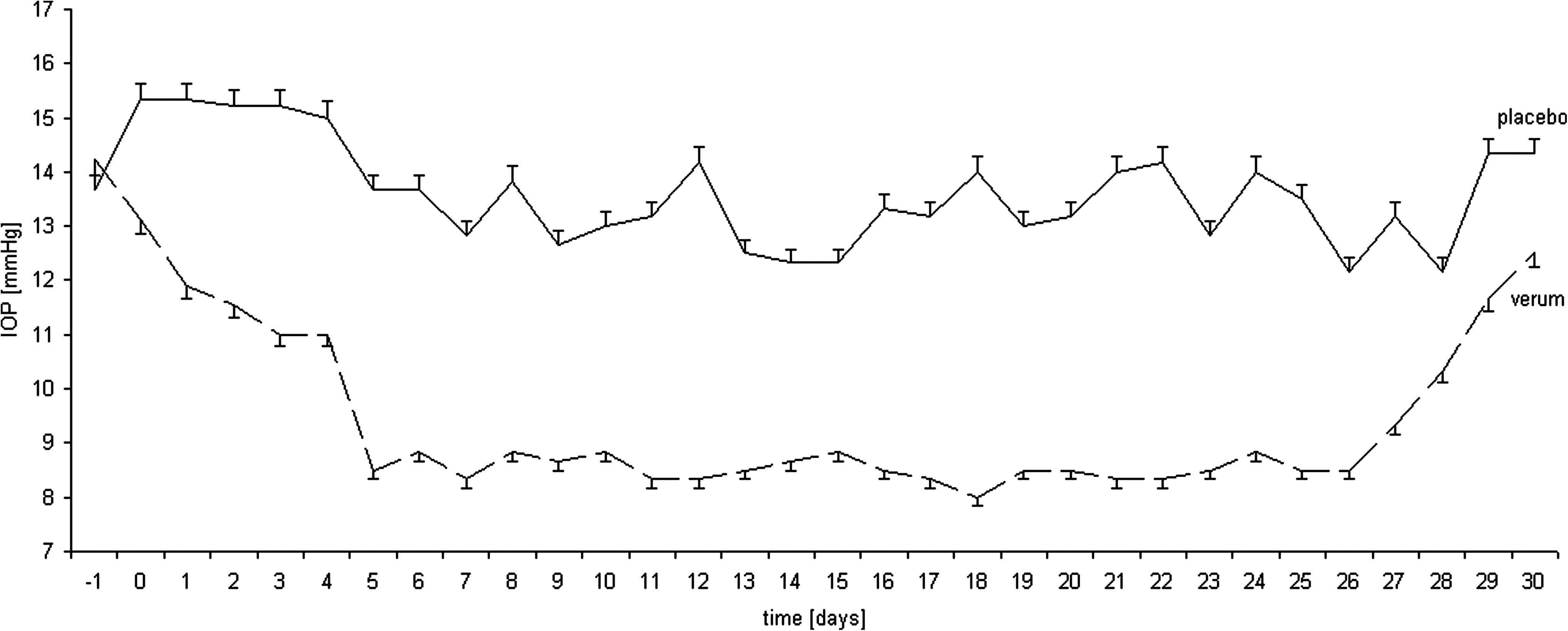
Intraocular pressure before (day −1), while (days 0–25), and after (days 26–30) application of brimonidine 0.1% (verum) eye drops in 1 eye (n=20) and placebo eye drops in the partner eye (n=20).
The mean baseline intraocular pressure was not different when comparing subjects with thick or thin corneas or when comparing the eyes to be treated with brimonidine 0.1% eye drops versus placebo eye drops within the 2 groups (Table 1). With treatment with brimonidine 0.1% eye drops, mean intraocular pressure in the thin cornea group (9±2 mmHg) was lower than in the thick cornea group (10±2 mmHg, P=0.018; Table 1). Mean intraocular pressure of contralateral placebo-treated control eyes was not significantly different between subjects with thin (13±2 mmHg) or thick (14±2 mmHg) corneas (P=0.241; Table 1).
Values given in the table are means±SEM.
ANOVA comparing the thin versus thick cornea group.
CCT, central corneal thickness; IOP, intraocular pressure.
No structural changes of the entire cornea or its individual layers were detected, neither on regular administration of brimonidine 0.1% eye drops nor of placebo eye drops.
Discussion
Since the introduction of brimonidine in 1996, it has clearly found its way as a selective alpha-2 adrenoceptor agonist in glaucoma treatment and treatment of ocular hypertension and is considered to be a safe and well-tolerated medication.10–12 In addition to the ciliary body—the genuine site where brimonidine shows its impact 1 —it is especially the retina, which has edged ever closer to the spotlight of brimonidine research under the aspect of neuroprotection. 3 Although it is known that, following topical administration, brimonidine is quickly taken up by the cornea 2 and that active alpha-2 adrenoceptors have been found to be present in the corneal epithelium and endothelium,6,7,13 there are only few data available regarding the impact of brimonidine on the cornea. Although it has been reported that almost all other glaucoma medications do have an effect on corneal thickness,14–20 the effect of brimonidine on corneal thickness has so far not been the focus of scientific studies.
Johnson et al. 4 suggested that central corneal thickness may affect the efficacy of some ocular hypotensive medications. The present study also could demonstrate that eyes with thinner corneas had a lower intraocular pressure while on treatment with brimonidine 0.1% than eyes with thicker corneas, even though intraocular pressure was statistically similar before treatment (Table 1). The authors of the OHTS 5 analyzed the effect of central corneal thickness on the reduction of intraocular pressure by ocular hypotensive medication. They found that the efficacy of ocular hypotensive drug treatment significantly correlated inversely with central corneal thickness and identified 3 mechanisms to account for these findings: (1) limited drug penetration through thicker corneas, (2) trends in differences in baseline intraocular pressure, and (3) the effect of central corneal thickness on intraocular pressure measurement. Unlike some previous studies,5,21–23 our study did not demonstrate a statistically significant positive correlation between baseline intraocular pressure and central corneal thickness and the effect of corneal thickness on Goldmann applanation tonometry may be small in the present study, as total corneal thickness has only a narrow range (543–560 μm). Thus, our findings indicate that differential pharmacokinetics may explain the negative correlation between the efficacy of brimonidine and central corneal thickness.
Corneal transparency is dependent on regulation of the hydration of the corneal stroma. Water is driven into the cornea across the epithelial and endothelial cell layers by the stromal swelling pressure. This fluid leak into the cornea is counterbalanced by the corneal fluid pump, which is predominantly attributed to the ion and fluid transport capacity of the endothelial cell layer. Primary and secondary active transport mechanisms are responsible for generating a net ion flux from the stromal to anterior chamber site of the endothelium. 24 Both the epithelium and endothelium prevent corneal swelling by functioning as diffusion barriers to the fluid and by acting as sites of active ion transport. 25 Although this pump-leak hypothesis was postulated several decades ago, the mechanisms underlying regulation of the balance between the pump and leak functions remain largely unknown. 26 Two important signaling pathways have been demonstrated in corneal epithelium and endothelium: (1) the phosphatidyl inositol pathway, activated by stimulation of muscarinic m5 cholinoceptors 27 and alpha-1-adrenoceptors (unpublished data), and (2) the cAMP proteinkinase A pathway, activated by stimulation of beta-adrenergic receptors 7 and inhibited by stimulation of muscarinic m4 cholincoeptors 28 and alpha-2-adrenergic receptors. 7 Chu and Candia 13 have shown that corneal epithelial Cl− ion transport is regulated by the interaction between the positive effects of beta- and alpha-1 stimulation and the negative influence of alpha-2 stimulation. Thus, corneal beta-receptor stimulation could activate primary and secondary active transport mechanisms resulting in deswelling of the stroma and a decrease of corneal thickness, and corneal alpha-2 adrenergic stimulation could counteract this mechanism by inhibiting these systems, resulting in swelling of the stroma and an increase of corneal thickness. As shown by the present study, stimulation of corneal alpha-2 adrenoceptors resulted in a quick yet reversible increase in corneal thickness (Fig. 1).
What is interesting in this context is the fact that the maximum increase in corneal thickness was reached after 2 days already and that corneal thickness returned to almost the same level as the initial value within another 2 days. It is assumed that this is due to receptor desensitization by the agonist itself, typically seen in alpha and beta adrenoceptors.29–31 However, because desensitization does not only depend on time factors but also on the dosage, the question whether a varied concentration of the active ingredient might also result in a time delay of this effect remains unanswered at the present time. Taking also into account that corneal homeostasis probably is the result of stimulation or blockage of most different receptors,32–34 it should also be discussed that other receptors that counteract the effect of alpha-2 adrenoceptor stimulation by brimonidine are increasingly activated from the second day on.
A comparable study showed that blocking of corneal beta adrenoceptors by timolol also resulted in an increase of central corneal thickness. 8 Because no differentiation could then be made between the individual layers because of the method used, corneal thickness was measured by means of SOCT in the present study. As expected, the most definite change was detected in the corneal stroma (Fig. 3). However, because the stroma does not have any alpha-2 adrenoceptors of its own,6,7 this effect must be considered to be a secondary one. As regards beta receptor blockers, an adverse effect on the endothelial pump-leak mechanism has been discussed 8 ; accordingly, activation of endothelial alpha-2 adrenoceptors might also result in a shift of the inflow/outflow ratio. No change of corneal endothelium was demonstrable by the present study (Fig. 4). However, it is not possible to draw any conclusion regarding the activity or function of endothelium from this, because neither its activity nor function can be assessed by endothelial thickness alone. Other studies could not demonstrate any endothelial change either, although variances in central corneal thickness were sometimes found to be present.8,14,15,18,20
What is more interesting is the fact that distinct thickening was also demonstrable in the corneal epithelium for 2 days, which then returned toward the same level as the initial value in the course of another 2 days (Fig. 2), though. The question whether this the result of a shift of fluid from outside to inside or, more likely, whether this is a (receptor-mediated?) response to pronounced stromal swelling cannot be answered based on the present study.
In an electron microscopic study, Polat et al. were able to demonstrate only mild ultrastructural changes of the corneal epithelium and endothelium on administration of beta adrenoceptor antagonists and alpha adrenoceptor agonists. 35 Broader and also microscopically visible changes were not detected. Although the quality of an SOCT scan cannot compare with a histologic or even better electron microscopic study, the present study could not demonstrate any structural change of the cornea as a result of the administration of brimonidine.
In summary, we can say that similar to other glaucoma medications topical administration of brimonidine also has a significant impact on central corneal thickness. The question whether this effect is due to epithelial and/or endothelial alpha-2 adrenoceptors cannot be finally answered at the present time. In addition, the question whether the reversible increase in corneal thickness on topical administration of brimonidine is of clinical significance remains unanswered. Further studies on this subject are currently in the stage of preparation.
Footnotes
Author Disclosure Statement
The authors have no proprietary interest in any of the products used in the study. No competing financial interests exist.