
Abstract
Abstract
Purpose:
We investigated whether an optimized combination of oral and topical levofloxacin would lead to higher levofloxacin concentrations in aqueous humor.
Methods:
Fifteen patients with cataracts in both eyes began topical treatment at 1 week before the first surgery and oral treatment at 1 day before the first surgery. On the day of surgery, they received oral and topical levofloxacin at 4 h and 1 h before surgery, respectively. Two days after the first operation, we performed cataract surgery on the second eye with the same drug administration protocol.
Results:
Postsurgery concentrations of levofloxacin in the aqueous humor of the first and second eyes were 2.87±0.89 μg/mL (mean±standard deviation, n=15) and 3.76±1.32 μg/mL, respectively; the levofloxacin level in the second eye was significantly higher than that in the first eye (P=0.0085).
Conclusions:
Our protocol to achieve high aqueous humor concentrations of levofloxacin may be favorable in preventing endophthalmitis after eye surgery.
Introduction
In a previous study, the aqueous humor concentration of levofloxacin was measured after administration of postoperative topical drops; this may have resulted in different levels of penetration compared with preoperative topical drops; the concentration reached a peak at 60 min after the last postoperative drop. 8 This suggests that topical administration of levofloxacin at 60 min before surgery may be the most efficient means of ensuring that maximal levels of levofloxacin are present in the aqueous humor at the time of surgery.
Levofloxacin has been also reported to have excellent penetration into the aqueous humor after systemic administration.9–12 Oral administration of levofloxacin led to 90% minimum inhibitory concentration (MIC90) levels in aqueous humor against a majority of ocular pathogens.9,10 Pea et al. demonstrated that levofloxacin concentrations in aqueous humor and plasma peaked 4–4.5 h after the last oral administration. 11 In this study, patients received two 500 mg oral doses at 10 h apart before undergoing cataract surgery (9 p.m. the previous evening and 7 a.m. on the morning of surgical intervention). Surgical intervention was performed within a time interval ranging from 1.5 to 6.0 h after the second oral administration of levofloxacin. This suggests that oral administration of levofloxacin at 4 h before surgery is the most efficient time to deliver the drug to the aqueous humor. Penetration of levofloxacin into the aqueous humor of the human eye after intravenous administration was also examined; aqueous humor levels were similar to those found after oral administration 12 and thus intravenous administration has no added benefit.
Although previous studies of combinations of topical and oral levofloxacin administration showed an additive effect on the concentration in aqueous humor,6,13,14 to our knowledge, an effective design for combined administration has not been discussed previously. An established, efficient protocol to deliver levofloxacin into aqueous humor using common oral and topical doses would enable safer cataract surgery without increasing the overall drug dosage. In the present study, we assessed the aqueous humor levofloxacin levels of patients undergoing cataract surgery at 1 h after the last topical administration and 4 h after the last oral administration. Further, we compared the levofloxacin levels of the first and second eyes to undergo surgery to determine the differences in penetration efficiency.
Patients and Methods
Patients
A total of 15 patients who underwent cataract surgery from February to March 2010 were included. Of the 15 patients, 11 were women and 4 were men. The patients' average age was 70.7±9.5 years (range: 58–89 years). The study protocol was approved by the internal review board of our institution, and informed consent was obtained from all patients before study entry. Exclusion criteria were all other ocular diseases, previous ocular surgery, and topical or systemic antibiotic treatment within the month prior to cataract surgery. No adverse effects were detected in the enrolled patients.
Patients were given 0.5% levofloxacin eye drops (Santen Pharmaceutical Company, Osaka, Japan) and 500 mg levofloxacin oral tablets (Daiichi Pharmaceutical Company, Tokyo, Japan) in accordance with the schedule in Fig. 1. Levofloxacin eye drops (0.5%) were administered starting at 1 week before surgery on the first eye 4 times per day and then 1 h before surgery. One 500 mg levofloxacin tablet per day was administered in the morning starting a day before the first surgery and continued for 1 week. A 500 mg levofloxacin tablet was also administered at 4 h before surgery on the operation day.

Timetable for oral and topical administration of levofloxacin. Levofloxacin eye drops (0.5%) 4 times per day were started at 1 week before surgery on the first eye and 1 h before surgery on the day of the operation. A daily oral dose of 500 mg of levofloxacin was administered in the morning beginning a day before surgery for 1 week and at 4 h before surgery on the day of the operation.
Drug concentration measurements
At the beginning of surgery, a sample of intraocular fluid from the anterior chamber (∼0.1 mL) was collected by paracentesis. All of the samples were stored at −80°C. Measurements of levofloxacin in the aqueous humor samples were performed using high-performance liquid chromatography by an independent laboratory (Sekisui Medical Company, ADME & Tox Research Institute, Ibaragi, Japan). A high-performance liquid chromatography system consisting of an LC-10AD binary pump (Shimadzu, Kyoto, Japan), an RF-10AXL fluorescence detector (Shimadzu), and a Class LC-10 chromatography workstation (Shimadzu) was used. Elution was performed using an ODS-80 column (Tosoh, Tokyo, Japan) at 30°C with a mobile phase of THF, 50 mM phosphate buffer (pH 2.0), and 1 M ammonium acetate (8/92/1, v/v/v). The flow rate was 1.0 mL/min and detection was performed using a fluorescence detector (excitation 296 nm and emission 503 nm). Drug concentrations were determined using a calibration curve constructed from known aqueous drug concentrations ranging from 10 to 10,000 ng/mL. Drug concentrations were calculated from the peak area and expressed as nanograms of drug per milliliter of aqueous humor. The detection limit of the analysis was 10 ng/mL.
Statistical analysis
All patients enrolled in the study were included in the statistical analysis. All results are shown by a box-and-whisker plot. Statistical significance was determined by 2-sided paired t-test. Differences with P<0.05 were considered to be significant.
Results
The levofloxacin concentrations that we found in the aqueous humor of the first and second eyes that underwent surgery are shown in Table 1 and Fig. 2. Levofloxacin levels in the aqueous humor of the first and second eyes were 2.87±0.89 μg/mL (mean±standard deviation, n=15) and 3.76±1.32 μg/mL, respectively. The difference in levofloxacin levels between the first and second eyes was highly significant (P=0.0085).
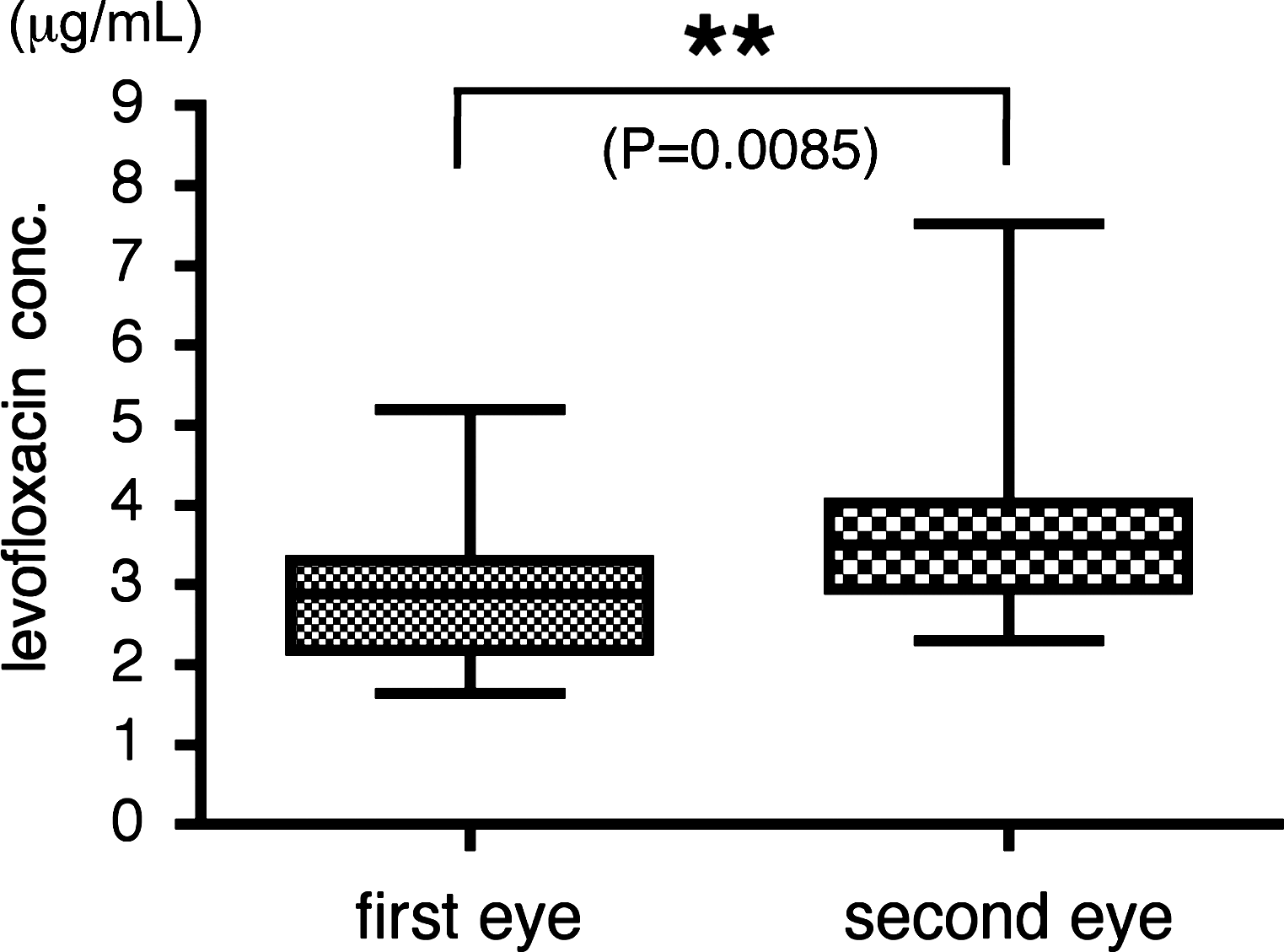
Levofloxacin concentrations in the aqueous humor in the first and second operated eyes. The aqueous humor levels of levofloxacin in the first and second eyes to undergo surgery were 2.87±0.89 μg/mL (mean±standard deviation, n=15) and 3.76±1.32 μg/mL, respectively. The difference in levofloxacin levels between first and second eyes was very significant (**P=0.0085).
P=0.0085, mean difference in levofloxacin concentrations between the first and second eyes to undergo surgery.
L, left eye; R, right eye; SD, standard deviation.
Discussion
Previous studies have described the pharmacokinetics of levofloxacin.8,11 We used this information to design and test a strategy to maximize levofloxacin concentrations in aqueous humor by oral and topical administration. Interestingly, we found that the aqueous humor level of levofloxacin in the second eye to undergo surgery was significantly higher in the first eye to be operated upon.
Because most cases of endophthalmitis are likely caused by the patients' own external flora, 15 it seems reasonable to assume that higher antibiotic concentrations in aqueous humor offer better protection against infection. The mean aqueous humor concentrations of levofloxacin shown in the present study were greater than the MIC90 of levofloxacin against common pathogens that cause postoperative endophthalmitis, including methicillin-resistant Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pneumoniae, and Propionibacterium acnes (Table 2).4,9,16 To the best of our knowledge, the mean levofloxacin concentration that we found in the aqueous humor of the second eye to undergo surgery was higher than that reported for any previously published study. Pea et al. showed that the median value of levofloxacin in the aqueous humor of patients receiving a final 500 mg oral dose at 4 h before cataract surgery was 3.29 μg/mL. 11 In other studies, the reported mean concentrations in aqueous humor yielded by topically applied levofloxacin were 0.73±0.66, 1 0.60±0.28, 2 0.37±0.55, 3 1.14±0.72, 5 0.69±0.47, 16 and 1.00±0.48 μg/mL. 17 Our higher levofloxacin level is most likely due to increased penetration of levofloxacin from the combination of oral and topical administration.
In the present study, we found significantly greater concentrations of levofloxacin in the second eye to undergo surgery in all patients; to our knowledge, this high mean increase in levofloxacin (0.89 μg/mL) between the first eye and second eye has not been described elsewhere in the literature. Pea et al. demonstrated that levofloxacin concentrations in aqueous humor increased almost parallel to those in plasma after oral administration, but decreased more slowly than plasma levels. 11 According to our unpublished data (analyzed by Daiichi Pharmaceutical Company), levofloxacin plasma levels measured at 24 h after each oral administration of 500 mg of levofloxacin did not show cumulative increases in Japanese adult males (data not shown). We hypothesize the following pharmacokinetics: Topical levofloxacin penetrates into the anterior chamber through the cornea, but most of the levofloxacin tends to leave the anterior chamber through trabecular outflow or uveoscleral pathways after a relatively short period of time. This makes it difficult to show a cumulative effect on levofloxacin concentration in the anterior chamber following topical administration. However, oral administration of levofloxacin penetrates into the eye globe through the ciliary process as aqueous humor is produced. Via this route, all of the orally administered levofloxacin is introduced into the vitreous cavity. As the vitreous cavity is a “dead-end space,” dispersion of levofloxacin from this location may be delayed. Repeated oral levofloxacin administration may have a cumulative effect on the concentration in the anterior chamber because of this delayed dispersion; we speculate that this is why significantly higher concentrations of levofloxacin were found in the second eye to undergo surgery, compared with the first eye.
In summary, the present study demonstrates that our strategy of combined oral and topical administration of levofloxacin achieved high concentrations of levofloxacin in aqueous humor at the time of surgery, which may contribute to prevent postoperative endophthalmitis in a variety of surgeries.
Footnotes
Author Disclosure Statement
No competing financial interests exist.