
Abstract
Abstract
Purpose:
The aim of the study was the quantitative pharmacokinetic evaluation of drug release from pretreated amniotic membrane (AM) in vitro.
Methods:
Cryopreserved AM pieces soaked in 3% ofloxacin ophthalmic solution were mounted in vertical Franz-diffusion cell system equipped with autosampler. In vitro release of ofloxacin was determined by quantitative absorbance measurement carried out with a UV spectrophotometer (wavelength 287 nm). Three groups were created according to the duration of soaking: 60 (Group 1), 120 (Group 2), and 180 (Group 3) minutes. Released amount of ofloxacin pro 1 cm2 of AM (μg/cm2) was calculated in the period of 1 to 450 min.
Results:
Ofloxacin was detectable in the acceptor phase 1 min after mounting in all groups. Until 120 min, rapid increase of released ofloxacin could be observed. From 120 to 450 min, the amount of released ofloxacin showed a slower increasing pattern. Released ofloxacin in Group 1 was significantly lower than in Group 2 after 90 min (19.4±10.4 μg/cm2, 51.6±20.7 μg/cm2, respectively, P=0.044). In Group 3, cumulative drug release was higher than in Group at all timepoints. No significant difference could be demonstrated between Groups 2 and 3 at only 1 min timepoint.
Conclusion:
Significant ofloxacin reservoir capacity of a single human amniotic layer could be demonstrated in vitro. AM acted as an ofloxacin slow release device for upto 7 h in vitro, depending on the duration of pretreatment of AM. Individual pretreatment of AM could increase beneficial effects of AM transplantation, especially in infectious keratitis.
Introduction
Besides ocular penetration of topically administered medicaments, 9 AM permeability has been recently published. In vitro and animal experiments showed that AM comprises a dual pharmacokinetic impact on topically administered ofloxacin: barrier and drug reservoir function. Kim et al. 10 pointed out the concept of using AM as a slow-release drug reservoir of ofloxacin in an animal model; they investigated AM, tear film, corneal, and aqueous levels of ofloxacin in rabbit eyes after AM transplantation. In our previous works, we described an in vitro model for pharmacokinetic examination of AM. 11 The objective of our study was to quantify the drug reservoir function of human AM applying the model developed for transamniotic pharmacokinetics of ofloxacin, a frequently used broad-spectrum topical antibiotic in ocular surface disease. 12
Methods
AM preparation
The research was approved by the Institutional Human Experimentation Committee and adhered to the tenets of the Declaration of Helsinki. AM obtained by elective Cesarean section was separated from the chorion as soon as possible, but latest 1 h after delivery by blunt dissection and rinsed with phosphate-buffered solution (PBS pH: 7.24). AM pieces of 25 mm in diameter (with the epithelial side up) were placed on Porafil cellulose acetate membrane filters of the same size (Machenerey-Nagel, GmbH & Co KG) with a pore diameter of 0.45 μm. AM pieces on filter membranes were frozen at −20°C. Neither antibiotic nor preservative was added to the medium.
In vitro drug permeability studies
In vitro permeability studies were performed with a vertical Franz-diffusion cell system (Hanson Microette TM Topical & Transdermal Diffusion Cell System; Hanson Research Corporation) containing 6 cells, as described earlier.11,13 AM pieces were separated from the membrane filters and soaked in 10 mL of 3% commercially available ofloxacin ophthalmic solution (Floxal eye drops, Dr. Mann-Pharma) in petri dishes for 60 (Group 1), 120 (Group 2), and 180 (Group 3) minutes. After soaking, AM pieces were placed on new membrane filters soaked in PBS for 20 min. AM pieces with the new membrane filter were mounted in a vertical Franz-diffusion cell system equipped with an autosampler. The effective diffusion surface was 1.767 cm2. PBS was used as an acceptor phase. Rotation of stirbar was set to 450 rpm. Experiments were performed at 37°C±0.5°C.
Samples of 0.8 mL were taken from the acceptor phase by the autosampler (Hanson Microette Autosampling System; Hanson Research Co.) and replaced with fresh receiving medium. Autosampling was performed at 1, 10, 15, 20, 25, 30, 40, 50, 60, 90, 120, 150, 210, 270, 330, 390, and 450 min. In vitro release of soaked AMs was determined by quantitative absorbance measurement carried out with a UV spectrophotometer (Unicam Heλios α Thermospectronic UV-spectrophotometer v4.55) at a wavelength of λ=287 nm. Untreated AM and membrane filter soaked in PBS served as negative control. Released amount of ofloxacin pro 1 cm2 of AM (μg/cm2) was calculated.
Statistical analysis
Drug release of cryopreserved AMs in 3 groups were compared with each other and with the control. Independent samples t-tests were performed by applying Excel software. Differences with P≤0.05 were regarded as significant.
Results
Ofloxacin was detectable in the acceptor phase 1 min after mounting in all groups. Table 1 summarizes cumulative released ofloxacin. In all groups, rapid increase of released ofloxacin could be observed from 1 min until 120 min (Table 1). From 120 to 450 min, the amount of released ofloxacin showed a slower increasing pattern.
Difference was considered significant, P<0.05 (t-test). Group 1: soaking time: 60 min. Group 2: 120 min, Group 3: 180 min.
Released ofloxacin in Group 1 was significantly lower than in Group 2 after 90 min (19.4±10.4 μg/cm2, 51.6±20.7 μg/cm2, respectively, P=0.044). In Group 3, cumulative drug release was higher than in Group at all timepoints. Between Groups 2 and 3, no significant difference could be demonstrated only at 1 min timepoint (11.2±2.4 μg/cm2, 22.1±7.5 μg/cm2, P=0.033).
The impact of AM soaking time was also evaluated by analyzing the released ofloxacin per cm2 in 1 min (Fig. 1) Drug release was the highest in the first 15 min of the experiment. In Group 1, drug release per minute decreased faster than in Groups 2 and 3. Further gradual decrease of drug release was observed after 15 min, but even at the end of the observation period, some drug release could be demonstrated: 0.0031 μg/cm2/min, 0.0069 μg/cm2/min, and 0.013 μg/cm2/min, respectively. In the acceptor phase of the control group, no ofloxacin could be detected.
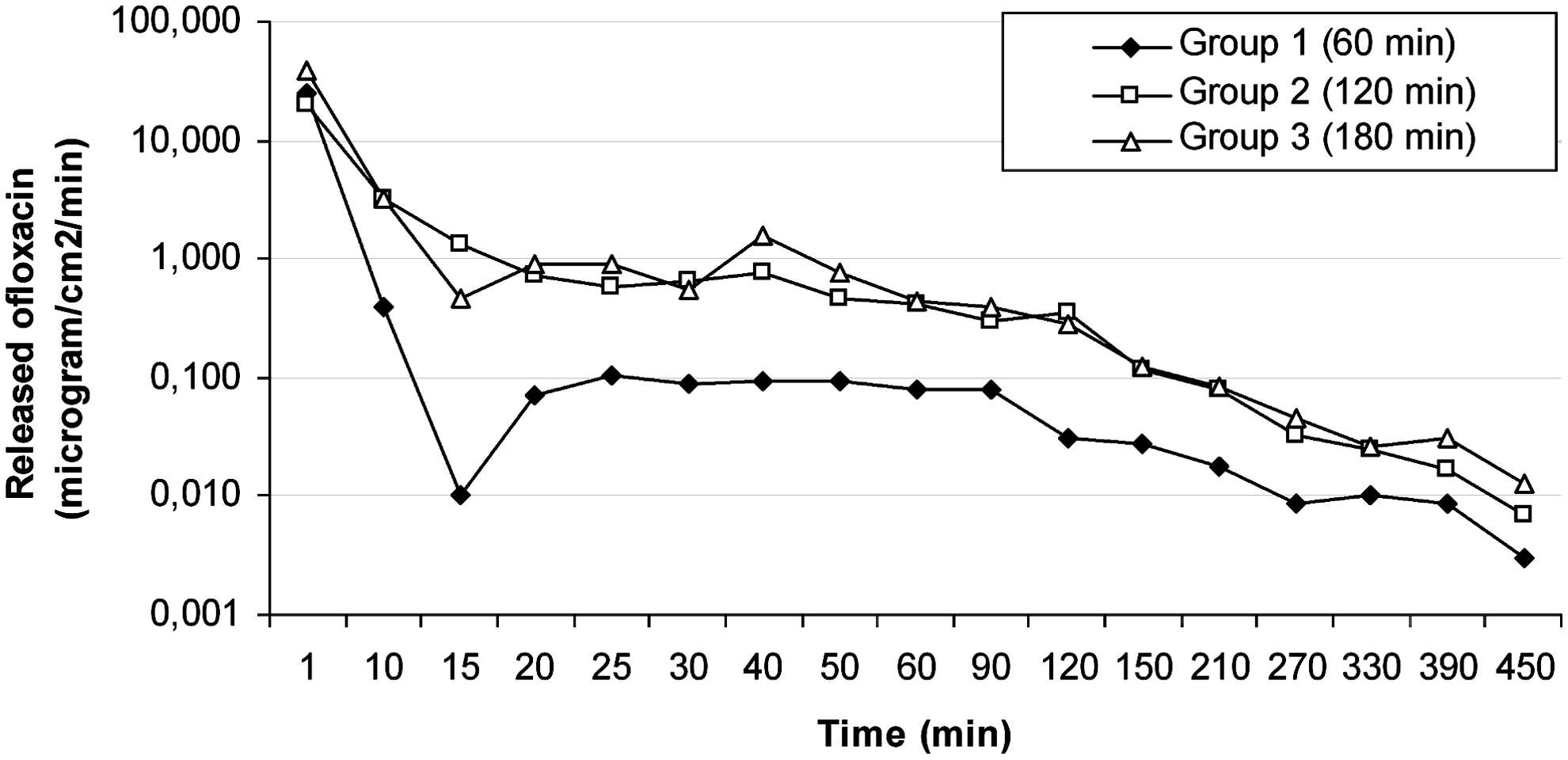
Logarithmic graph of Released Amounts (μg) of ofloxacin via 1 cm2 Amniotic Membrane in 1 min. Note significant difference of Groups 2 (from 90 min) and 3 (from 10 min) from Group 1 (t-test P<0.05). No difference between Groups 2 and 3.
Discussion
Beneficial effects of AM transplantation can be optimized with adequate pretreatment and postoperative topical treatment. 1 Application of the appropriate topical antibiotics is the choice of treatment of bacterial keratitis. 10 Postoperative treatment should start as early as possible to ensure stable concentration of drugs in tear and ocular tissues. To achieve efficient concentration, which is essential in the treatment of microbial keratitis, frequent application of eyedrops is necessary. 14 Beck 15 has shown in patients undergoing cataract surgery that the highest concentrations of fluoroquinolones were measured after the mode of application in which one drop had been given every 15 min before operation. The prepared liposomal hydrogel by Hosny enhanced the transcorneal permeation of ofloxacin 7-fold more than the aqueous solution. 14
Kim 10 and coworkers have supposed that AM might have a slow-release drug reservoir function, which can promote the ocular penetration of ofloxacin. Our group has developed an in vitro model in Franz diffusion cells combined with UV spectrophotometry. 11 With the method, transamniotic penetration of AM could be quantified. In penetration experiments, AM was not pretreated, but ofloxacin was filled in the donor compartment.
Our current study has some limitations. First of all, in this study, a simple diffusion model was applied, which is not exactly modeling the position of the AM on the corneal surface. AM is a compressible membrane on the surface of the eye with tears (and with topical drugs) bathing only one side (donor compartment). Recipient compartment in vivo is not a liquid substance, but corneal tissue. In addition, eyelids might have an effect of compression of AM by blinking and squeezing fluid out of the swollen reservoir. Blinking also does not allow long exposure times.
In the current experiment, AM was pretreated and soaked in ofloxacin for different durations (1, 2, and 3 h). The clinically relevant question was the determination of the minimal period, which provides the best reservoir capacity of AM.
Our experiments demonstrated that the reservoir capacity is dependent on the duration of soaking. It could be shown that AM can store, in general, more ofloxacn, when soaking time is increased from 1 to 2 h. Further, increase of soaking period to 3 h did not result in further significant increase of the released drug amount, in general. If 2 and 3 h results are compared, we can assume that released ofloxacin is greater than in 1 h group, but difference is significant from 90 min only at 2 h, but already at 10 min in 3 h group. Results of 1 h soaking is quite similar to our previous experiments, when 0.3 mL ofloxacin was added to the untreated AM.
Efficacy of ocular surface disease treatment could be improved by an effective slow-release material, such as hydrogels 16 or therapeutic contact lens. 17 The ocular tolerance of these artificial substances, however, can be problematic, but AM is well tolerated and absorbed or integrated by corneal tissues. 18
Hosny et al. 14 prepared a topically effective in situ thermosensitive prolonged release liposomal hydrogel for ofloxacin. AM, similar to in situ thermosensitive ofloxacin liposomal hydrogel, ensures steady and prolonged transcorneal permeation, which can improve the ocular bioavailability, minimizes the need for frequent administration, and decreases the ocular side effect of ofloxacin.
We conclude that significant ofloxacin reservoir capacity of a single human amniotic layer could be demonstrated in vitro in a Franz-diffusion cell system. AM acted as an ofloxacin slow-release device for upto 7 h in vitro. Drug release was dependent on the duration of pretreatment of AM. Two hours of pretreatment with ofloxacin was found to be necessary for the complete fillup of the reservoir capacity of AM. Clinical relevance of our findings might be that individual pretreatment of AM could increase the beneficial effects of AM transplantation, especially in infectious keratitis.
Footnotes
Acknowledgment
This work was supported by TAMOP-4.2.1/B-09/1/KONV-2010-0005 project.
Author Disclosure Statement
None of the authors have any interest in any instruments or materials used in this study.