
Abstract
Abstract
Purpose:
The aim of this study was to evaluate the efficacy and safety of bimatoprost in Japanese patients with normal-tension glaucoma (NTG) who showed insufficient response to latanoprost.
Methods:
A prospective, nonrandomized study was conducted in patients with NTG, with ≤20% intraocular pressure (IOP) decrease from pretreatment baseline with latanoprost monotherapy who had been switched to bimatoprost. The IOP was measured at 4, 8, and 12 weeks after the switch to bimatoprost. In 12 weeks after the switch to bimatoprost, efficacy and safety were evaluated.
Results:
Postswitch to bimatoprost, IOP was significantly reduced at every visit. Bimatoprost produced significantly greater mean% IOP reduction rate from pretreatment than that of latanoprost at week 12 (P<0.01). There was a significant correlation between% IOP reduction of bimatoprost and that of latanoprost (Pearson r2=0.374; P=0.007). No significant difference was observed in the mean scores of conjunctival hyperemia and corneal epithelial disorder between bimatoprost-treated eyes and latanoprost-treated eyes.
Conclusions:
Significant additional IOP lowering was achieved by switching to bimatoprost in Japanese patients with NTG with insufficient response to latanoprost. Bimatoprost treatment was safe and well tolerated.
Introduction
The Tajimi study, which is one of the largest glaucoma epidemiology studies in Japan, showed that the glaucoma prevalence rate in Japanese older than 40 years of age is 5.0%, and the rate of open-angle glaucoma is 3.9%.15,16 The study also reported that almost 90% of the open-angle glaucoma consisted of normal-tension glaucoma (NTG). The NTG is a clinical entity characterized by glaucomatous optic nerve damage and visual field defects with an IOP in the statistically normal range. The IOP is, however, a part of the pathogenic process in NTG, and IOP lowering is effective in reducing the progression of glaucomatous damage. 17 Although latanoprost is commonly used as first-line therapy in the treatment of NTG, there are some cases that show insufficient response to latanoprost. 18
The purpose of this study was to evaluate the efficacy and safety of bimatoprost in eyes with insufficient response to latanoprost in Japanese patients with NTG.
Methods
This clinical trial was conducted at the following 3 investigational sites. December 2009 to December 2010: Department of Ophthalmology, Kagawa University Faculty of Medicine, Social Insurance Ritsurin Hospital, and Ueda Eye Clinic (Kagawa, Japan). All the aspects of the study were in compliance with the Declaration of Helsinki, and all the patients gave their consent on being sufficiently informed by an investigator.
Examinations of visual acuity, refraction, both central and peripheral fields, slit-lamp examination, and gonioscopy were performed on all the patients. The eligibility criteria were age ≥20 years; bilateral or unilateral NTG: glaucomatous optic disc abnormalities and corresponding glaucomatous visual field defects, normal open angle, and IOP (measured using Goldmann applanation tonometer) of 21 mmHg or lower without medication; ≤20% IOP decrease from pretreatment baseline at least 12 weeks of treatment with latanoprost 0.005% (Xalatan®; Pfizer, New York, NY) monotherapy. Exclusion criteria were the subjects being with active ocular diseases in either eye except glaucoma; with retinal disease that has a potential risk of progression; with experience of ocular surgery or lazer treatment; with regimen for systemic or local administration of steroid during this study; with corneal disease in either eye that poses a problem for veracious IOP measurement.
A total of 18 patients who fit the study criteria were enrolled in this study. The study consisted of 4 scheduled visits over 12 weeks (day 0 and weeks 4, 8, and 12). At day 0 (preswitch), eligible patients who had used latanoprost 0.005% were switched to bimatoprost 0.03% (Lumigan®; Allergan, Inc., Irvine, CA) treatment. The administration time of bimatoprost had been set to just around the same time before administration of latanoprost.
Measurements of IOP, best-correlated visual acuity, and biomicroscopic examinations were conducted at each visit. The IOP was measured at the same time period during the administration of latanoprost with Goldmann applanation tonometer by using the same procedure at all centers. The outcome due to primary efficacy was the main change in IOP at week 12 from preswitch.
Biomicroscopy was performed by using a slit-lamp examination without pupil dilation. The examination included an assessment of the lid/lashes, conjunctiva, anterior chamber, cornea, iris, and lens. Conjunctival hyperemia was assessed by a single observer by using a 5-point hyperemia grading scale using 5 different photographs for hyperemia matching: 0=none, 0.5=trace, 1=mild, 2=moderate, and 3=severe. Corneal epithelial disorders were recorded by using an A (area) D (density) grading scale by a slit-lamp examination. 19
The study outcome for efficacy was based on the conditions of the patients' eyes with the higher IOP at the eligibility visit. If IOP was same in both eyes, we analyzed the right eye. Descriptive statistics for mean IOP, mean IOP change, and% IOP change from pretreatment were calculated. Statistical significance was assessed by using paired t test. The degrees of conjunctival hyperemia and corneal epithelial disorder were analyzed by using an averaged score of both eyes' values. Evaluation of the degrees of conjunctival hyperemia and corneal epithelial disorder was analyzed by using a Wilcoxon signed-rank test. The correlation mean% IOP change from pretreatment between eyes treated with latanoprost and eyes treated with bimatoprost was analyzed by using a Pearson's correlation coefficient test. All the statistical analyses were performed by using SPSS for Windows, Version 11.5 (SPSS, Inc., Chicago, IL). A P value of 0.05 or less was considered statistically significant. Data are presented as mean±standard deviation.
Results
There were 4 men and 14 women (mean age, 68.2±15.3 years), who had the mean refractive error of −2.3±4.9 diopters. All subjects completed the study. No significant changes in visual acuity were detected throughout follow-up (data not shown).
The IOP data were as follows: pretreatment=17.3±1.6 mm Hg; preswitch=16.0±1.3 mm Hg; 12 weeks=14.1±1.7 mm Hg. At week 12, IOP was significantly lower than both the pretreatment IOP (P<0.01) and the preswitch IOP (P<0.01) (Fig. 1). Although the mean% IOP reduction from pretreatment to preswitch (latanoprost) was −7.5%±5.6%, the mean% IOP reduction from pretreatment to 12 weeks (bimatoprost) was −18.7%±8.9% (Fig. 2). At week 12, 7 patients showed ≥20% IOP decrease, and 2 patients showed ≥30% IOP decrease from pretreatment (Fig. 3). There was a significant correlation between% IOP reduction of bimatoprost and that of latanoprost (Pearson correlation coefficient r 2 =0.374; P<0.01) (Fig. 3).

Reduction in mean IOP after a switch to bimatoprost. Data express the mean±SD. *P<0.05 versus pretreatment (paired t test). #P<0.05 versus preswitch (paired t test). IOP, intraocular pressure; SD, standard deviation.

Mean% IOP reduction from pretreatment to preswitch (Latanoprost) and at week 4, 8, and 12 (Bimatoprost). The mean% IOP reduction rate of bimatoprost was significantly greater than that of latanoprost (*P<0.01, paired t test). Data express the mean±SD.
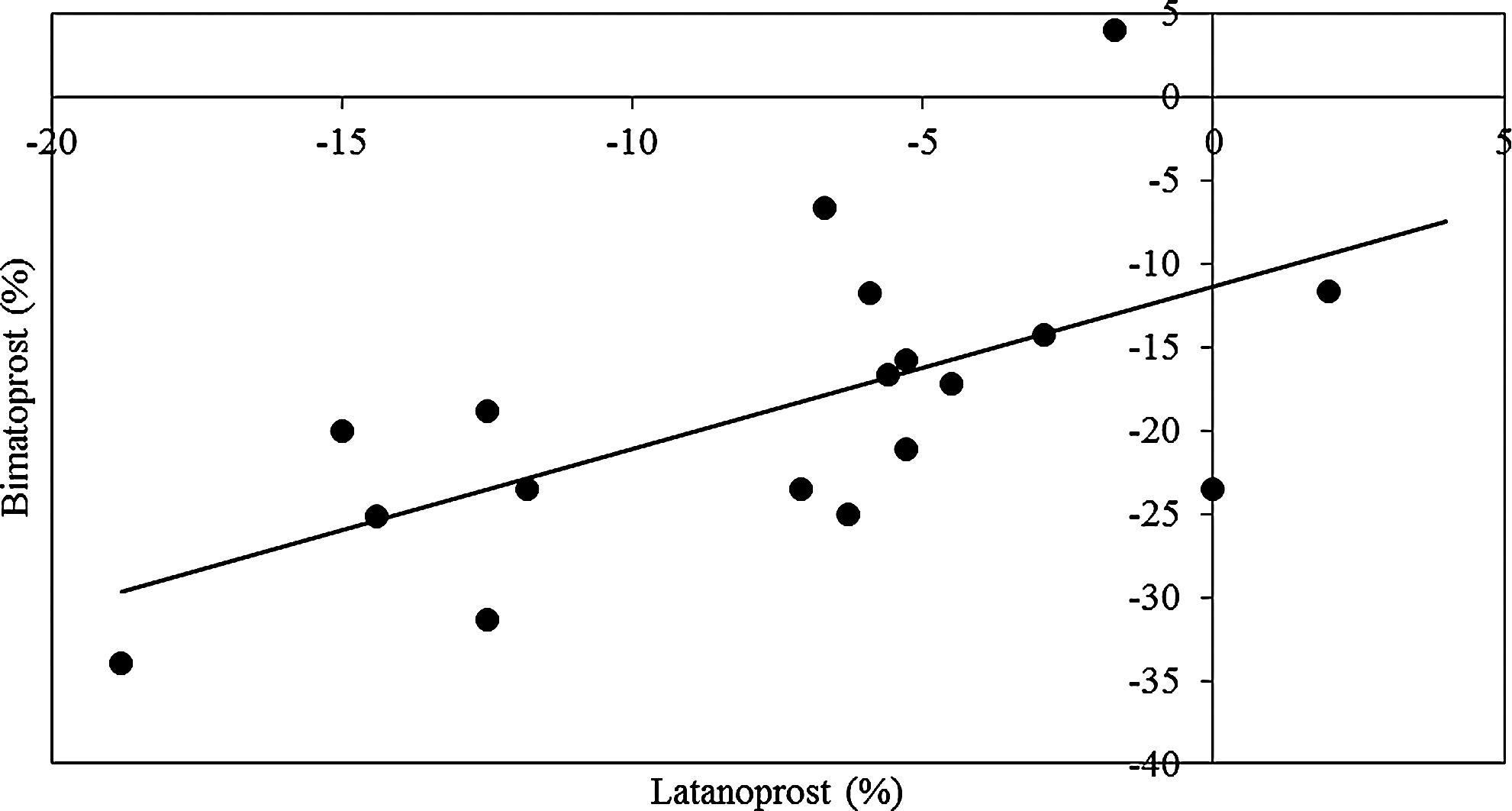
Correlation between% IOP reduction rate of bimatoprost and latanoprost. % IOP reduction rate of bimatoprost was significantly correlated with that of latanoprost. (Pearson correlation coefficient R2=0.374; P=0.007).
The mean hyperemia scores at preswitch and week 12 were 0.31±0.35 and 0.56±0.54 (P=0.27), respectively (Table 1). The mean corneal epithelial disorder scores at preswitch and week 12 were 0.67±0.97 and 0.67±0.97 (P>0.99), respectively (Table 1).
Discussion
The incidence rate of latanoprost nonresponders is reported at 28.1% and was highest in patients with NTG in Japan. 18 The reduction of IOP in patients with lower baseline IOP may be more difficult. 20 Several studies revealed that the IOP-lowering effect of bimatoprost was even equal to or higher than that of latanoprost.2,11–14
Bimatoprost was difficult to be converted to its free acid form in human eyes, and free acid was slightly detected at the site of action in the eye.8,21,22 In contrast, latanoprost is a prodrug that needs de-esterification to yield a pharmacologically active free fatty acid. Due to this, the pharmacological effect of bimatoprost is difficult to be attenuated because of its metabolism compared with latanoprost. Gandolfi and Cimino 14 previously reported that most of the subjects with glaucoma or OH who showed no significant IOP response to latanoprost were successfully treated with bimatoprost. They speculated that the lack of response to latanoprost was associated with poor de-esterification of the prodrug to the pharmacologically active free fatty acid. In early studies, the additional IOP-lowering effect of bimotoprost was seen in patients who responded poorly to latanoprost, thus suggesting a superior IOP-lowering effect of bimatoprost, compared with latanoprost.14,23 Mean IOP before the switch to bimatoprost, however, was approximately 23 mm Hg in their study.14,23 Our study suggests that the decrease of IOP also occurred with switching to bimatoprost in Japanese patients who are insufficient responders to latanoprost even though pretreatment IOP is low.
In this study, we showed that the mean IOP reduction rate of bimatoprost was significantly correlated with the mean IOP reduction rate of latanoprost. Bimatoprost showed a trend to enhance the potency of latanoprost. Prostaglandin F2α (FP) prostanoid receptors are G-protein coupled receptors that mediate the actions of PG F2α, which is confirmed to be an alternative splice variant of the human FP (altFP) prostanoid receptor gene. 24 Since bimatoprost interacts not with PG FP receptor but with prostamide receptor, bimatoprost is likely to have a pharmacologically inherent receptor.7,8 It has been reported that bimatoprost may interact with the FP-altFP receptor heterodimer to induce alterations in second-messenger signaling. 25 FP-altFP complexes may represent the underlying basis of bimatoprost pharmacology. 25 Since prostamide and FP receptors may be encoded by the same gene, the lowering effects on IOP of bimatoprost might correlate with those of latanoprost.
Conjunctival hyperemia was the most commonly reported side effect of bimatoprost and the most frequently observed biomicroscopic finding in several studies.2,3,14 Conjunctival hyperemia occurs more frequently with bimatoprost than with latanoprost. 26 There were, however, no significant differences in the mean score of conjunctival hyperemia between bimatoprost-treated eyes and latanoprost-treated eyes in this study. The switch from latanoprost to bimatoprost in the glaucoma therapy was associated with less conjunctival hyperemia than that measured in patients in whom bimatoprost was used as first-line therapy. 27 One of the limitations of this study is that there was no control group. There is the possibility that some patients who had conjunctival hyperemia caused by latanoprost may continue after withdrawal. Ocular surface hyperemia occurs by endothelial-derived nitric oxide-mediated vasodilatation and is not associated with intraocular inflammation. 28 Even though there is a trend toward exacerbation during the switching phase, no patients withdrew from the treatment. In addition, the deepening of eyelid sulcus due to bimatoprost has been reported. 29 Although 1 patient complained of the deepening of eyelid sulcus, the patient continued the treatment.
Low ocular perfusion pressure is an established risk factor in glaucoma. 30 Quaranta et al. 31 recently reported that in previously untreated patients with NTG, both latanoprost and bimatoprost reduced the IOP from untreated baseline, to a similar extent, over a 24-h curve. Latanoprost was associated with slightly improved ocular diastolic perfusion pressure over 24-h but similar absolute perfusion levels to those of bimatoprost. 31
In conclusion, bimatoprost provided a significant reduction in IOP for at least 12 weeks for Japanese patients with NTG who showed insufficient response to latanoprost.
Footnotes
Author Disclosure Statement
No competing financial interests exist.