
Abstract
Abstract
Purpose:
The purpose of this study was to evaluate the safety and efficacy of intravitreal bevacizumab in treatment-naive patients with choroidal neovascularization (CNV) secondary to pathologic myopia over a 2-year interval.
Methods:
Patients diagnosed with myopic CNV who had not received previous treatment were given intravitreal injections of bevacizumab (2.5 mg/0.1 mL). All patients were retrospectively evaluated using best-corrected visual acuity (BCVA) and central macular thickness (CMT) measured with optical coherence tomography (OCT).
Results:
Twenty-six eyes of 26 patients aged 15–81 years (mean, 42.6 years) were enrolled. OCT images demonstrated that the mean CMT±standard deviation (SD) significantly changed from 270±47 μm at baseline to 228±35, 218±35, 212±25, 210±29, and 209±30 μm in the 1st, 3rd, 6th, 12th, and 24th post-treatment months, respectively (P<0.001 for all). The BCVA in logarithm of the minimum angle of resolution±SD significantly changed from 0.75±0.43 at baseline to 0.57±0.44, 0.42±0.44, 0.39±0.47, 0.41±0.44, and 0.42±0.41 in the 1st, 3rd, 6th, 12th, and 24th post-treatment months, respectively (P<0.001 for all). The mean number of injections was 1.69 (range, 1–4) within the 24-month period. The follow-up period ranged from 24 to 35 months (mean, 28 months). No other ocular or systemic adverse effects were observed.
Conclusions:
Although the present study lacked a control group, the results in this small series of patients over the 2-year follow-up period indicate that intravitreal injection of 2.5 mg bevacizumab is effective and safe in patients with myopic CNV.
Introduction
Methods
All patients in this study were diagnosed with CNV secondary to pathologic myopia and were naive to treatment for CNV. Patients with systemic diseases involving the retina were excluded. The study was carried out in adherence to the tenets of the Declaration of Helsinki. No institutional review board approval was required because of the retrospective study design. Patients included were treated between May 2007 and September 2008 at the Chang-Gung Memorial Hospital, Kaohsiung, Taiwan. The inclusion criteria were (1) spherical equivalent refractive error of −6 diopters (D) or more in phakic eyes, an axial length of >26.5 mm as measured by A-mode ultrasonography in pseudophakic cases, or retinal signs of pathological myopia; (2) subfoveal or juxta-foveal location of the CNV as indicated by fluorescein angiography (FA); and (3) clinical follow-up of at least 24 months after the initial IVB treatment. The exclusion criteria included (1) patients with features suggesting that the CNV was secondary to age-related macular degeneration (AMD), angioid streaks, uveitis, trauma, or hereditary diseases in the studied or nonstudied eye; (2) a history of PDT, TTT, laser photocoagulation, or vitrectomy in the studied eye; (3) a history of triamcinolone acetonide sub-Tenon or intravitreal injection; (4) presence of a severe cataract; (5) cataract surgery during follow-up; (6) the presence of other serious posterior segment complications such as retinal detachment or foveoschisis; and (7) follow-up of <24 months after the initial IVB. Including bevacizumab in the treatment protocol was strictly based on physician and patient preference after thorough discussion of the nature of off-label use of bevacizumab and its potential side effects, particularly the possibility of thromboembolic events. Patients with uncontrolled hypertension or recent history of myocardial infarction or cerebral vascular accident were not offered bevacizumab. Alternative regimens offered were elaborately discussed, and the definitive decision was made by the patient.
A detailed chart review was performed with special attention to best-corrected visual acuity (BCVA; measured by Landolt C visual acuity charts), intraocular pressure (IOP; measured by Goldmann applanation tonometry), fundus photography, FA, and macular scan with third-generation optical coherence tomography (OCT-3; Carl Zeiss Meditec, Dublin, CA) at baseline and all follow-up periods. Evidence of an active CNV on the basis of leakage on FA and intraretinal or subretinal fluid on OCT was required to initiate treatment. FA was repeated whenever the physician suspected a recurrence or persistence of CNV, if any deterioration of OCT findings occurred, or if visual symptoms were seen. The need for repeated IVB was assessed if there was evidence of fluorescein leakage on FA, persistence of apparent subretinal or intraretinal fluid in OCT (indicating activity), and a minimal dosing strategy was used instead of frequent fixed-dose regimens.
Central macular thickness (CMT) was measured for all eyes using OCT-3. This map was created from six 6-mm individually and sequentially acquired high-resolution radial B scans that intersected at the fovea. The OCT software measured CMT automatically. Experienced technicians did all OCT examinations at baseline and all follow-up periods.
IVB injection
Patients received 2.5 mg/0.1 mL of bevacizumab (Avastin; Genentech, Inc., South San Francisco, CA) using the standard protocol of Chang Gung Memorial Hospital, Kaohsiung. In the surgery room, topical anesthesia was applied, povidone–iodine 5% eye drops were applied several times, and a sterile lid speculum was placed over the eye. Bevacizumab was injected into the vitreous cavity using a 27-gauge needle at 3.5 and 4.0 mm posterior to the limbus in pseudophakic and phakic eyes, respectively, after anterior chamber paracentesis to avoid drug reflux during injection and prevent elevation of IOP. The injection site was pressed with a sterile cotton swab to prevent leakage. After IVB, vision was immediately checked to confirm retinal perfusion; this required visual acuity sufficient to detect at least hand movements. Following this, tobramycin and dexamethasone ointment (Tobradex™; Alcon, Inc., Hunenberg, Switzerland) was immediately applied.
All patients were instructed to return to department for checkup at 1 week, 1 month, 3 months, and every 3 months thereafter after IVB injection and anytime if patients experienced sudden visual deterioration or any systemic or ocular adverse events. At every visit, the patients were specifically questioned for the appearance of systemic adverse events (acute elevation of blood pressure, signs of cerebrovascular accidents, myocardial infarctions, and/or ischemia), and ocular adverse events (pain, floaters, and reduced visual acuity).
Statistics
The visual acuity measurements were converted to the logarithm of the minimum angle of resolution (logMAR) 14 at baseline and at repeated intervals thereafter for statistical analyses. The Wilcoxon signed-rank test was used for statistical analysis. A P value of <0.05 was considered statistically significant.
Results
Forty-two eyes were followed up for more than 24 months after the initial IVB treatment during the study period. Sixteen eyes were excluded according to the study criteria: 3 eyes received PDT, 5 eyes had a history of intravitreal triamcinolone acetonide, 2 eyes had a severe cataract, 2 eyes received cataract surgery during the study follow-up period, and 4 eyes had foveoschisis. Finally, this consecutive, retrospective, nonrandomized clinical interventional study included 26 eyes of 26 patients (17 women and 9 men) treated with 2.5 mg bevacizumab for active, subfoveal (13 eyes), or juxta-foveal (13 eyes) CNV secondary to pathological myopia. Patients averaged 42.6 years of age [standard deviation (SD), 13.0 years; range, 15–81 years]. The duration of symptoms ranged from 2 weeks to 8 months (mean±SD, 2.12±2.32 months). The mean spherical equivalent refractive error was −10.4±3.6 D (range, −6.25 to −16.75 D) in 21 phakic eyes, and the mean axial length was 28.51±1.8 mm (range, 28.18 to 29.71 mm) in 5 pseudophakic eyes. The follow-up period ranged from 24 to 35 months (mean, 28.0 months; Table 1).
IVB, intravitreal bevacizumab; CNV, choroid neovascularization; FA, fluorescein angiography.
The mean CMT±SD significantly changed from 270±47 μm at baseline to 228±35, 218±35, 212±25, 210±29, and 209±30 μm in the 1st, 3rd, 6th, 12th, and 24th post-treatment months, respectively (P<0.001 for all; Table 2 and Fig. 1). The BCVA in logMAR±SD significantly changed from 0.75±0.43 at baseline to 0.57±0.44, 0.42±0.44, 0.39±0.47, 0.41±0.44, and 0.42±0.41 in the 1st, 3rd, 6th, 12th, and 24th post-treatment months, respectively (P<0.001 for all; Table 2 and Fig. 2). A representative patient is shown in Fig. 3.

Mean values±SDs of central macular thickness (CMT; measured by optical coherence tomography) over time (in months) in choroidal neovascularization in pathologic myopia that was treated with intravitreal bevacizumab. A significant decrease in thickness over time (P<0.001) is observed. SD, standard deviation.
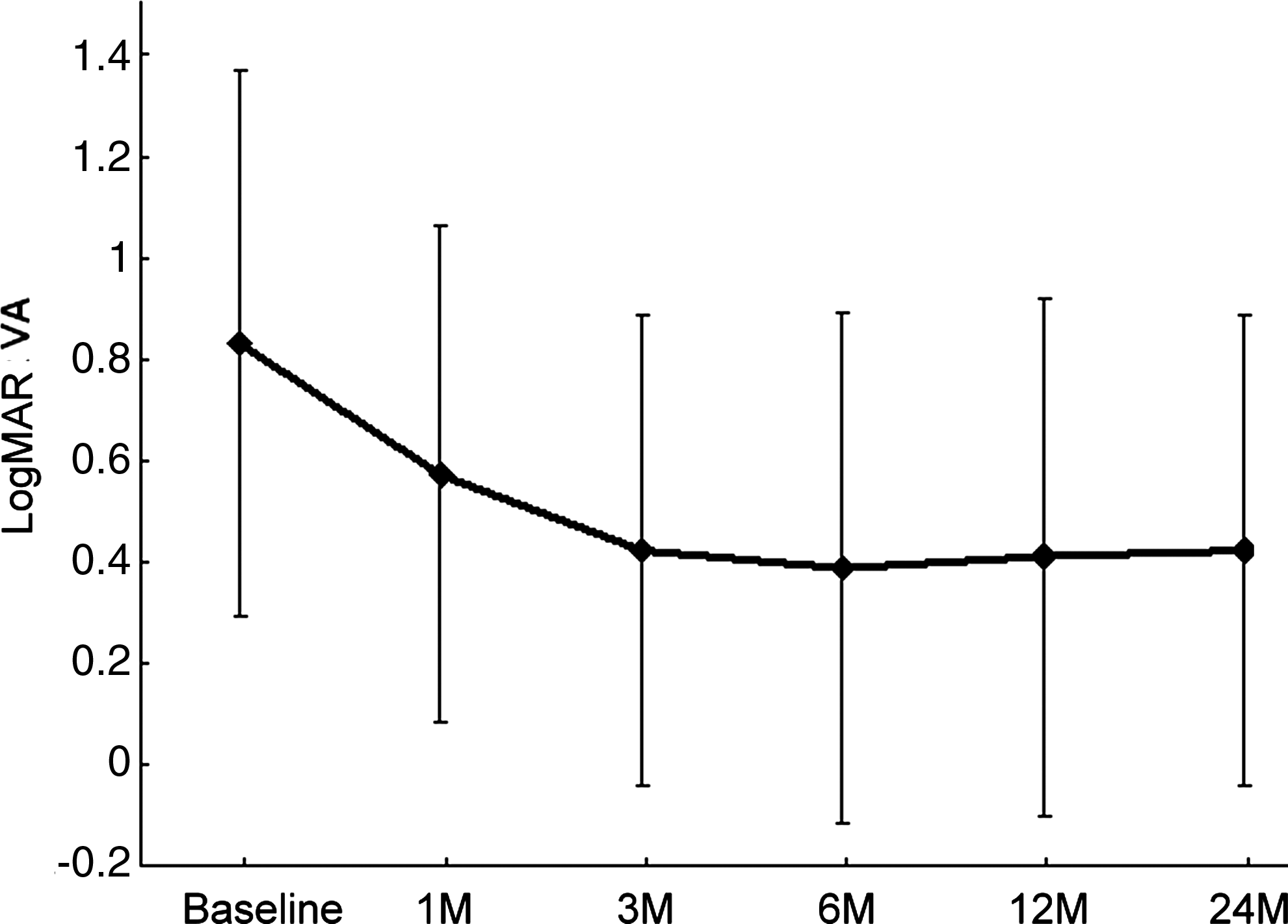
Mean values±SDs of best-corrected visual acuity in logarithm of the minimum angle of resolution value (logMAR BCVA) over time (in months) in choroidal neovascularization in pathologic myopia that was treated with intravitreal bevacizumab. A significant improvement of visual acuity (P<0.001) is observed. SD, standard deviation.
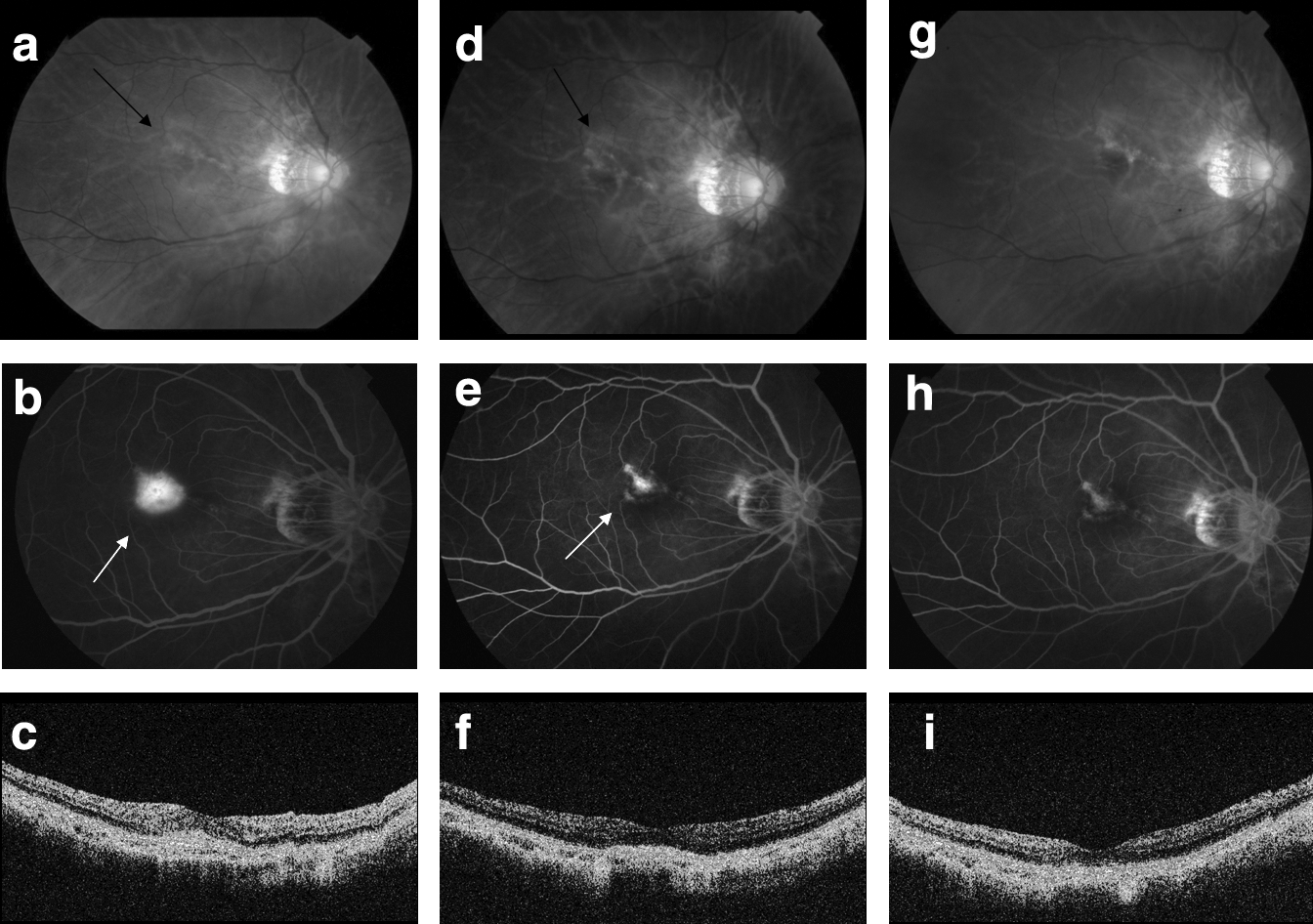
Right eye of a 57-year-old Chinese woman with myopia −9.25 diopters.
Values given are mean±standard deviation.
CMT, central macular thickness; logMAR BCVA, best-corrected visual acuity in logarithm of the minimum angle of resolution.
After 24 months (all patients were examined at a final follow-up visit), the BCVA improved more than 3 lines in 16 eyes (62%), remained unchanged (including improvement of <3 lines) in 7 eyes (27%), and lost more than 1 line in 3 eyes (11%). Further, 14 eyes (54%) had a BCVA equal to or better than 20/40. The mean number of IVB injections during the 24-month follow-up was 1.69 (range, 1–4); 12 eyes received 1 injection (46%), 10 eyes received 2 injections (38%), 3 eyes received 3 injections (11%), and 1 eye received 4 injections (4%). In 12 of 14 patients requiring multiple injections, the second injection was administered within the first 6 months; in the other 2 patients, it was administered between 7 and 12 months. Three patients required a third injection and 1 required a 4th injection between 13 and 18 months. No injection was administered to any patient during the 19–24 months after the initial treatment.
In our study, none of the patients in our study reported any major systemic complications related to IVB. Also, no major ocular adverse events, including infectious endophthalmitis, drug-related inflammation, vitreous hemorrhage, or retinal detachment, were observed on all study eyes during the follow-up periods.
Discussion
Before the development of antivascular endothelial growth factor drugs, PDT was considered the main treatment option for myopic CNV. The VIP study is the largest to examine the efficacy and safety of PDT with verteporfin in the treatment of subfoveal CNV associated with myopia. 15 At 12 months, 72% of verteporfin-treated eyes had a visual loss of <8 letters compared with 44% of placebo-treated eyes. Visual improvement of 5 letters (1 line) was noted in 40% of PDT-treated patients versus 13% of those in the placebo group after 24 months. 5
Currently, IVB injection therapy is a treatment option for CNV resulting from various causes including AMD, idiopathic causes, and myopic CNV.10–13,16,17 However, IVB injection may carry potential risks because of the route of delivery. The safety profile of IVB for various retinal conditions has been recently investigated. The results of these studies showed that IVB is a relatively safe treatment, and no serious adverse events were observed.18–21
In this study, anterior chamber paracentesis was carried out before injection to avoid drug reflux during injection and prevent sudden elevation of IOP under the use of higher dosage of 0.1 mL/2.5 mg bevacizumab. Theoretically, paracentesis might carry some risks of infection. However, the incidence of these complications is very low if the procedure is carried out cautiously.
Recently, lower doses (1 and 1.25 mg) of IVB were found to have favorable results at 6 months and at 1- and 2-year follow-up intervals.12,13,22–28 However, the frequency of IVB injections required to achieve increase in visual acuity has been an important topic of discussion. In contrast to CNV in AMD, in which a treatment protocol of 3 injections at monthly intervals was shown to be superior to a single injection, no clear evidence exists that this procedure can be beneficial for patients with myopic CNV.16,17
We used a reinjection treatment strategy based on changes in the OCT and FA findings instead of frequent fixed-dose regimens. The reason for using the 2.5 mg dose of bevacizumab, as opposed to 1 or 1.25 mg, was to achieve a sufficient therapeutic concentration of the drug in the larger volume of the vitreous chamber of a highly myopic eye. Studies of IVB treatment in AMD have shown improvement in visual acuity using higher doses that required less frequent reinjection.14,29 Hernandez-Rojas et al. reported a short-term beneficial effect of using a 2.5 mg IVB treatment for myopic CNV, which included a significant decrease in foveal thickness and improvement in BCVA within 3 months without producing any local or systemic side effects. 11
At 24 months after the initial IVB treatment, our results showed that the mean injection rate of 1.69 was lower compared with previous studies using a 1 or 1.25 mg dose [eg, Ikuno et al. (1 mg, 12 months, 2.4 injections), Gharbiya et al. (1.25 mg, 12 months, 4 injections), Chan et al. (1.25 mg, 12 months, 3.6 injections), Ruiz-moreno et al. (1.25 mg, 12 months, 3.7 injections), and Voykov et al. (1.25 mg, 24 months, 2.9 injections)].23–24,30,31 In our study, 12 eyes (46%) received only 1 injection and 10 eyes (38%) received 2 injections. We assume that the longer half-life of the larger dose of bevacizumab may help decrease the frequency of reinjection. Our results suggest that infrequent dosing (1–2 doses) of bevacizumab (2.5 mg) is beneficial for the regression of myopic CNV and that a high frequency of injections, which holds a high risk of retinal tears or detachment, is not necessary in patients with myopia.
Previous studies have demonstrated that age is a critical factor for prognosis in myopic CNV. The natural course of myopic CNV is highly dependent on age at onset and final visual acuity is also dependent on age at initial treatment.7,32–34 For example, Axer-Siegel et al. 7 reported a significant final visual improvement in 33% of younger patients (<60 years) and in only 6% of older subjects (>60 years); similarly, significant visual worsening was recognized in 8% of younger subjects and in 50% of older subjects. Also, Montero and associates divided subjects who received PDT for myopic CNV into 2 groups, a younger group (<55 years) had a significant better visual outcome than an older group (>55 years). 32 Patients' age in our study (mean, 42.6 years old) was younger than that in previous studies (mean, 48.9–60.1).24,30,31 Therefore, we assume that patient's age may also play a role in the reduced number of injections.
In the present study, 58% of the patients attained significant visual improvement (better than 3 lines), 31% had an unchanged BCVA, and 54% had a BCVA equal to or better than 20/40 at 24 months after IVB. In contrast, 12% of the patients attained significant visual improvement (equal to or better than 3 lines), and 30% had a BCVA equal to or better than 20/40 at 24 months after PDT. 5
At present, the optimal dose and interval of IVB treatment for myopic cases are unknown. The potential clinical benefit of IVB will only be known after performing careful long-term studies specifically designed to evaluate the safety profile and efficacy of this therapeutic approach. The results of the present study demonstrated that infrequent injections (1 to 2 injections) of 2.5 mg bevacizumab may be beneficial to patients with myopic CNV over the course of a 2-year follow-up period without any side effects. OCT and/or FA-based IVB may be useful in determining whether reinjection is necessary.
The strength and novelty of this study is a relatively longer follow-up period of 2 years using a relative higher dose of 2.5 mg bevacizumab. The limitations of the study are its retrospective, noncomparative, and nonrandomized study design. However, all these patients had well-documented clinical data. A prospective future study with a larger number of patients, controls, different dosage of IVB, and a longer follow-up period may reveal the efficacy of IVB for the treatment of myopic CNV.
Footnotes
Author Disclosure Statement
The authors have no proprietary interest in this work.