
Abstract
Abstract
Purpose:
To study the effect of intravitreal bevacizumab injection in recurrent central serous chorioretinopathy (CSC).
Methods:
Retrospective case series. Patients followed at the Yale Eye Center with a diagnosis of recurrent CSC who were treated with intravitreal bevacizumab from January 2007 to January 2009 were studied. Intravitreal injections of bevacizumab were given once every 4 weeks until sub-retinal fluid resolved. We collected preinjection visual acuity, optical coherence tomography (OCT), fluorescein angiography imaging, number of injections administered, OCT data after each injection, and visual acuity after each injection. Each patient was followed for a minimum of 6 months.
Results:
Three patients met the inclusion criteria. All patients were men and aged from 39 to 46 years. All patients had recurrent disease. None had received prior treatment. Mean preinjection visual acuity was logMar 0.30, with a median of 0.30. Mean postbevacizumab visual acuity was 0.03, 0.07, and 0.03 at 1, 3, and 6 months, respectively. Median postbevacizumab acuity was 0, 0.10, and 0 at 1, 3, and 6 months, respectively. Baseline preinjection central macular thickness (CMT) by OCT imaging ranged from 320 to 500 μm, with a mean of 388 μm and a median of 344 μm. Mean CMT at month 1 was 248 μm, with a median of 190 μm. Mean CMT at month 3 was 252 μm, with a median of 281 μm. Mean CMT at month 6 was 273 μm, with a median of 187 μm.
Conclusions:
Bevacizumab may be an effective treatment option for patients with recurrent CSC. Although long-term efficacy is unknown, it is a relatively low-risk treatment option that may improve visual acuity and CMT.
Introduction
Recurrent CSC is particularly challenging and can lead to a permanent decrease in central acuity and to foveal atrophy. Neurosensory detachments persistent for as little as 4 months have been noted to cause permanent photoreceptor atrophy, 9 and therefore, early intervention seems prudent for visual recovery. We report a series of 3 patients with recurrent disease, characterized by granular sub-retinal deposits, which signify disease duration of 1 month or longer, and also paucifocal or multiple areas of retinal pigment epithelial (RPE) disturbance,9,10 who had improvement with intravitreal injections of bevacizumab (Avastin, Genentech).
Methods
A retrospective review was performed on the charts of patients who were followed at the Yale Eye Center with a diagnosis of CSC who had been treated with intravitreal bevacizumab from January 2007 to January 2009. In addition to demographic data, we collected preinjection visual acuity, preinjection optical coherence tomography (OCT; Stratus, Humphrey-Zeiss) central macular thickness (CMT), preinjection fluorescein angiography imaging, number of injections administered, OCT data after each injection, and also visual acuity after each injection. Visual acuities were collected as Snellen acuities and then converted to logMar. Each patient was followed for a minimum of 6 months. The study was approved by the Yale University Human Investigation Committee.
Results
Case reports
Patient 1
Patient 1 is a 46-year-old Asian man with a history of chronic myelogenous leukemia, in remission for the past 6 months, who reported a 4-week history of blurry vision in his left eye. He experienced a similar episode over 10 years ago, and had never received prior treatment. His logMar visual acuity was 0.30 on presentation. The fluorescein angiogram showed a smokestack pattern of leakage superonasal to the fovea with pooling centrally. OCT confirmed a neurosensory serous detachment with CMT 500 μm (Fig. 1). Treatment options were discussed and the patient elected to try an intravitreal injection of bevacizumab. About 1.5 mg of bevacizumab was injected. Four weeks later, the patient noted no significant change in vision with corrected visual acuity of 0.40, even though there was decreased sub-retinal fluid (SRF) and decreased CMT to 366 μm. The patient received a 2nd bevacizumab injection. Four weeks later, vision had improved to 0.18 and CMT was stable at 355 μm. A 3rd bevacizumab injection was given and 4 weeks later, the patient reported subjective improvement in vision, and acuity showed improvement to 0.10. CMT had decreased to 299 μm. A 4th bevacizumab injection was given, and 4 weeks later, vision improved to logMar 0, with OCT revealing complete resolution of SRF with CMT of 162 μm (Fig. 1). The patient was then followed every 4 weeks for 2 more visits. The vision remained stable at logMar 0 without any return of SRF, confirmed by OCT imaging. His last visit was 6 months from the last injection and vision remained logMar 0 and OCT imaging showed no SRF with CMT of 174 μm.
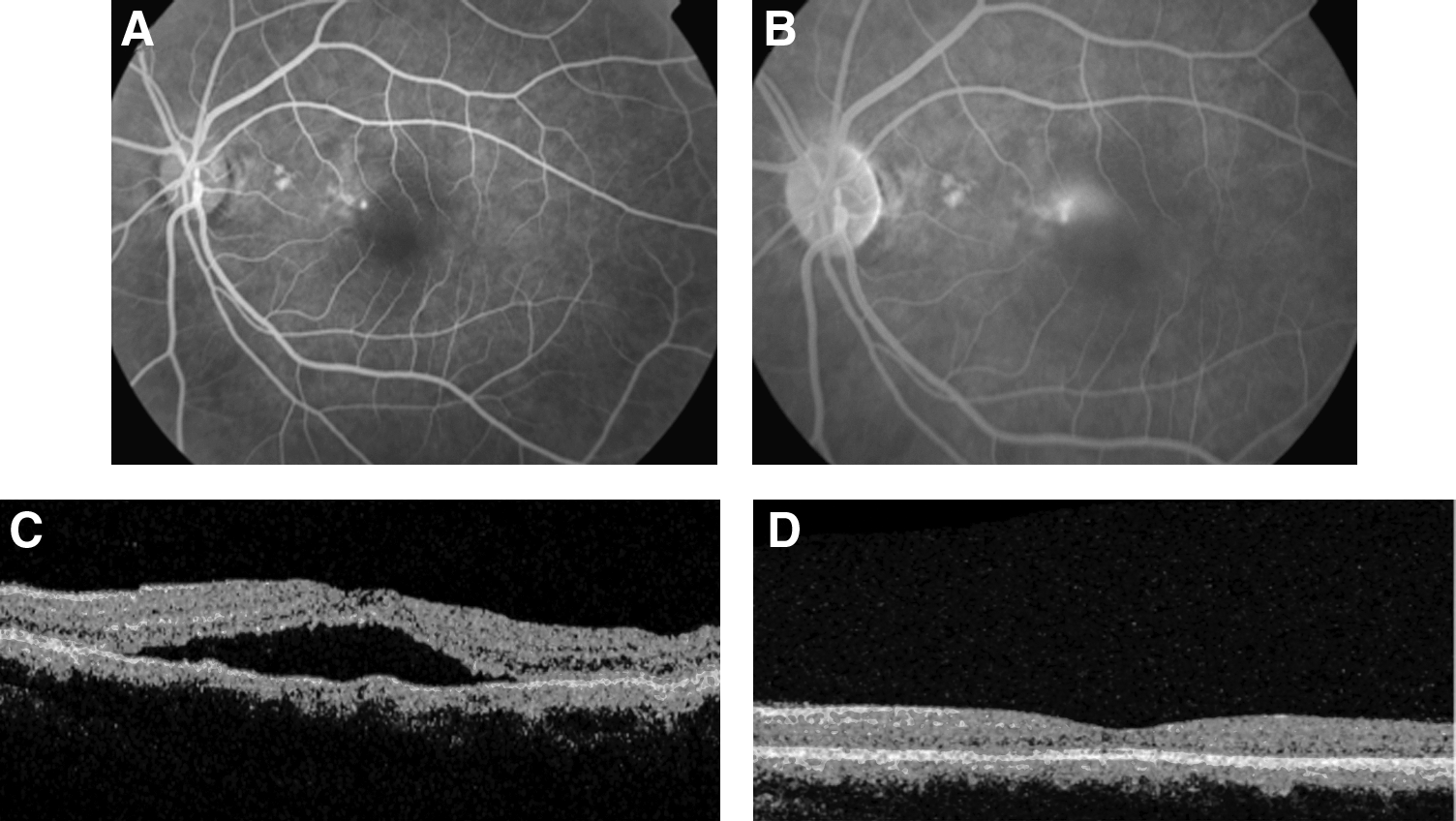
Patient 1. Fluorescein angiogram and optical coherence tomography (OCT) before bevacizumab treatment
Patient 2
Patient 2 is a 45-year-old Hispanic man who complained of 4 months of persistent blurring of vision in his left eye. His medical history was notable for hypercholesterolemia and also a history of CSC 1 year prior that had resolved without treatment. LogMar visual acuity on presentation was 0.30. Fluorescein angiography revealed an expansile dot pattern of leakage temporal to the disc and also smaller areas of leakage superotemporal and inferior to the fovea. OCT confirmed a neurosensory serous detachment with CMT of 344 μm (Fig. 2). Treatment options were discussed and the patient elected intravitreal bevacizumab injection, 1.5 mg. Four weeks later, vision improved to 0.10 and OCT revealed complete resolution of SRF with CMT of 190 μm (Fig. 2). Four weeks later, vision was stable at 0.10 and OCT showed no return of SRF. The patient returned for follow-up 4 months later (6 months after last bevacizumab injection) complaining of decreased vision in the left eye. Visual acuity was 0.10. OCT imaging showed no return of SRF with CMT of 187 μm.
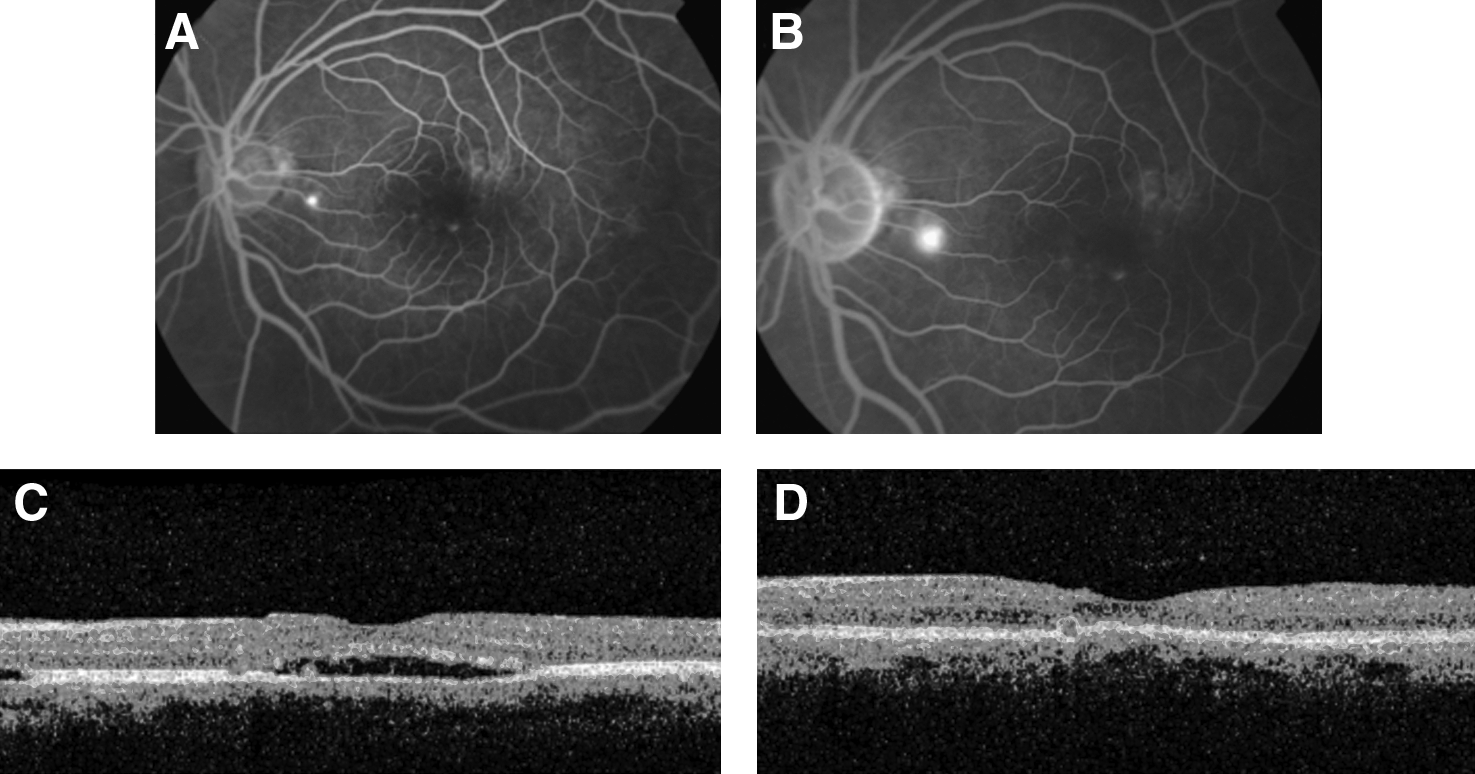
Patient 2. Fluorescein angiogram and OCT before bevacizumab treatment
Patient 3
Patient 3 is a 39-year-old Caucasian man with no significant medical history who complained of blurry vision in his right eye for the past 8 weeks. He had a prior episode of CSC 1 year ago that resolved spontaneously. On presentation, his logMar visual acuity was 0.30. Fluorescein angiography revealed an area of perifoveal pooling in the superior macula with a neurosensory serous detachment, confirmed by OCT with CMT of 320 μm (Fig. 3). Treatment options were discussed with the patient, and he opted for an intravitreal bevacizumab injection of 1.5 mg. Four weeks later, visual acuity improved to logMar 0 and OCT showed resolution of SRF with CMT of 188 μm (Fig. 3). Four weeks later, vision remained stable at logMar 0, and there was no recurrence of SRF by OCT imaging. Four weeks later, however, the patient noted a gray spot in the central vision of his right eye. LogMar visual acuity was 0, but OCT imaging showed a small neurosensory detachment with CMT 281 μm. A second intravitreal bevacizumab injection was given. Four weeks later, his vision had decreased to 0.40 and there was a corresponding increase in SRF with CMT of 418 μm on OCT. He was given a 3rd bevacizumab injection. When the patient returned for follow-up 6 weeks later, vision had improved to 0.18 despite a slight increase in CMT to 495 μm. He was given a 4th bevacizumab injection and 4 weeks later vision improved to logMar 0 with a slight improvement in CMT to 458 μm. A 5th injection of bevacizumab was given and 4 weeks later; vision remained stable at logMar 0, with improvement in CMT to 417 μm. The patient opted for observation and additional bevacizumab was not given. Four weeks later, vision was 0.10 and CMT was 405 μm.
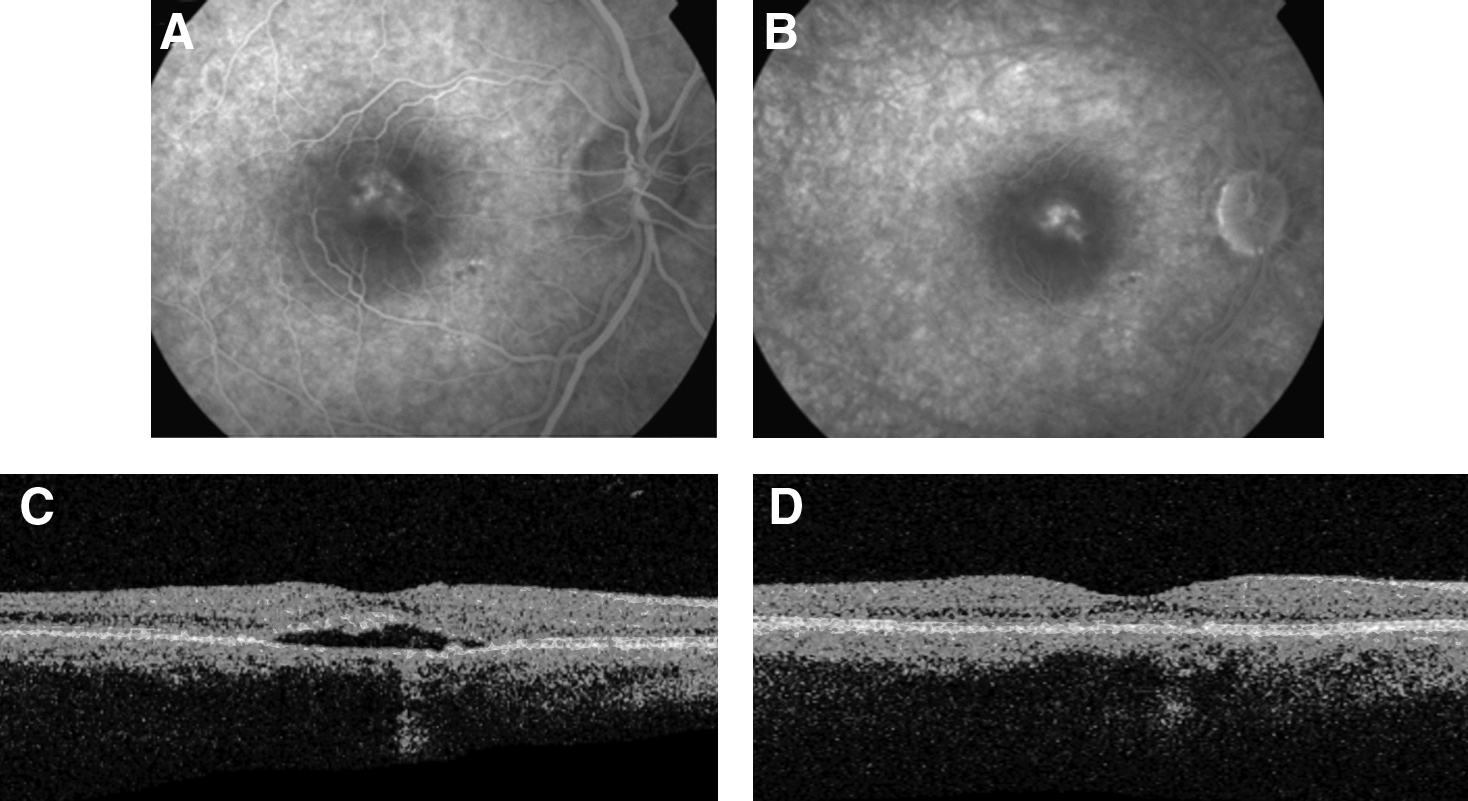
Patient 3. Fluorescein angiogram and OCT before bevacizumab treatment
Discussion
Bevacizumab is a monoclonal antibody to vascular endothelial growth factor (VEGF) that has been widely used in recent years primarily in the treatment of choroidal neovascularization but also in proliferative diabetic retinopathy, diabetic macular edema, pseudophakic cystoid macular edema, macular edema due to vein occlusions, and in iris neovascularization.11–15 In addition to its role in angiogenesis, VEGF has been shown to modulate vascular permeability and breakdown of the blood–retinal barrier in diabetes 16 ; thus, bevacizumab is effective in the treatment of diabetic macular edema. It is also reasonable to believe that bevacizumab may be an effective means of modulating the increased choroidal vascular permeability that may be responsible for CSC. Torres-Soriano et al. recently reported successful treatment of 5 eyes with CSC with intravitreal bevacizumab 2.5 mg, 17 as did Lim et al. using 1.25 mg of bevacizumab. 18
Although all 3 patients in our series experienced a prior episode of CSC with spontaneous resolution, none could recall the time required for resolution, but did recall a fast recovery. By the time of presentation for the current episode, the patients complained of a longer duration of symptoms. The presence of sub-retinal granular deposits and paucifocal or multifocal areas of RPE changes, and also patient desire for treatment established precedence for earlier intervention, as eyes with recurrent disease are predisposed to visual morbidity, including decreased final visual acuity, stereopsis, and color vision. 10 Given the favorable results in our patients with recurrent CSC treated with intravitreal injection of bevacizumab, early intervention with bevacizumab in recurrent cases is a reasonable and safe treatment option. Additional studies are warranted to help elucidate long-term efficacy and safety.
Footnotes
Acknowledgments
This research was supported in part by the Leir Foundation (New York City, NY), Newman's Own Foundation (Westport, CT), and Research to Prevent Blindness (New York, NY). The sponsors or funding organizations had no role in the design or conduct of this research.
Author Disclosure Statement
The authors have no conflicts of interest, and no financial or proprietary interest in this research. The authors have full control of all primary data and agree to allow the Journal of Ocular Pharmacology and Therapeutics to review their data upon request.