
Abstract
Abstract
Purpose:
The purpose of this article was to evaluate the efficacy and safety of intravitreal bevacizumab (Avastin) in eyes with macular edema secondary to central retinal vein occlusion (CRVO).
Methods:
Forty-five consecutive eyes with macular edema secondary to CRVO were included in a prospective clinical trial. Eyes were treated with 3 initial intravitreal bevacizumab injections of 1.25 mg at monthly intervals. Retreatment was based on central retinal thickness (CRT) measured by optical coherence tomography (OCT). OCT was performed monthly; fluorescein angiography was performed every 3 months. Main outcome parameters were visual acuity (VA, using the Early Treatment of Diabetic Retinopathy Study protocol) and CRT in an 18-month follow-up period.
Results:
After 18 months of follow-up, mean VA increased from 40.9 letters at baseline to 61.9 letters (+21 letters; P<0.001) at month 18; CRT decreased from 572.3 μm at baseline to 273.2 μm at month 18 (−299.1 μm; P<0.001). Neither age, duration of CRVO, baseline VA, nor baseline CRT was correlated with the change in VA. No drug-related systemic or ocular side effects were observed following intravitreal bevacizumab treatment.
Conclusions:
Intravitreal bevacizumab is generally well tolerated and may improve VA and decrease CRT in patients with macular edema secondary to CRVO over a period of 18 months.
Introduction
An alternative for patients with macular edema secondary to CRVO is antivascular endothelial growth factor (anti-VEGF) therapy. As intravitreal levels of VEGF in CRVO are the highest of those measured in retinal vascular disease, 11 and VEGF has been implicated as the major factor responsible for increased vascular permeability and macular edema, 12 the inhibition of VEGF could be of therapeutic value for CRVO. Bevacizumab (Avastin; Genentech, San Francisco, CA), a recombinant monoclonal antibody binding all isoforms of VEGF, has been approved for cancer therapy and available for off-label use in ophthalmology.13–16 Since the first report of the efficacy of intravitreal bevacizumab in a patient with macular edema secondary to CRVO in 2005, 14 several case series have analyzed its effect for CRVO, showing promising functional and anatomic results.17–20
Our prospective study evaluated the biological effect, change in VA, and safety of intravitreal bevacizumab in patients with macular edema secondary to CRVO.
Methods
The present study was designed as a prospective, consecutive, noncomparative case series. All patients provided written informed consent before study enrollment. They were carefully informed about the off-label character of the treatment and its potential risk for retinal detachment and endophthalmitis. Institutional review board approval was obtained, and the study was performed in accordance with the Declaration of Helsinki guidelines.
For study inclusion, patients ≥18 years of age with clinical, angiographic, and evidence from optical coherence tomography (OCT) of macular edema [central retinal thickness (CRT): >250 μm] secondary to CRVO were eligible for enrollment in the study. Eligible best-corrected visual acuity (BCVA) in the study eye ranged from 73 to 19 letters at 4 m using the Early Treatment of Diabetic Retinopathy Study (ETDRS) protocol (20/40 to 20/400). Exclusion criteria included BCVA <19 letters (<20/400) in the follow eye; pregnancy; uncontrolled hypertension; greater than moderate nonproliferative diabetic retinopathy or macular edema associated with diabetic retinopathy; evidence of a vitreoretinal interface abnormality; presence of any other ocular condition that could affect VA or macular edema during the course of the study; history of laser photocoagulation within the previous 3 months; history of intraocular surgery within the previous 6 months; use of intraocular, peribulbar, or retrobulbar steroids within the previous 6 months; history of intraocular injection of a VEGF antagonist within the previous 3 months; and uncontrolled glaucoma.
All eyes underwent a complete ophthalmologic evaluation at baseline that included BCVA testing using ETDRS charts at 4 m, slit-lamp biomicroscopy, IOP measurement, indirect ophthalmoscopy, color fundus photography, OCT using the Stratus OCT (Carl Zeiss Meditec, Dublin, CA), and fluorescein angiography (FA).
Each patient received 3 monthly intravitreal injections of 1.25 mg bevacizumab (0.05 mL). All injections were performed under sterile conditions in the operating room. Povidone–iodine solution was used to clean the eyelids; a lid speculum was then inserted. Topical anesthesia was applied and the conjunctiva was irrigated with 5% povidone–iodine. A 30-gauge needle was inserted through the pars plana and 0.05 mL of bevacizumab was injected into the vitreous cavity.
Follow-up examinations were performed at 1 day, 1 week, and 1 month after the first injection and in monthly intervals thereafter over a period of 18 months. BCVA testing, slit-lamp examination, IOP measurement, indirect ophthalmoscopy, and OCT were performed at each study visit. FA was performed at 3-month intervals. After 3 initial injections, retreatment was indicated whenever persistent or recurrent macular edema (CRT >250 μm) was documented by OCT.
The primary endpoint of the study was the mean change in BCVA from baseline to 18 months. The secondary endpoints included mean change in BCVA and CRT from baseline to 6, 12, and 18 months, number of treatments, and ocular and systemic safety.
Statistical analysis
Statistical analyses were performed using statistical package for the social sciences (SPSS, Chicago, IL). The t-test was used for statistical analysis of changes in BCVA and CRT. A P value of less than 0.05 was considered to be statistically significant. For correlations, Pearson's product-moment correlation test was used and specified by coefficient r and by P for significance.
Results
Baseline characteristics
In all, 45 eyes of 45 consecutive patients with macular edema secondary to CRVO were enrolled in this study. The mean age at the start of the study was 62.3 years (range: 42–78). Twenty-five of the patients were male. Before study enrollment, the mean duration of CRVO symptoms was 25.1 weeks (range: 5–64). Fluorescence angiographic findings at baseline revealed 33 nonischemic CRVOs (NICRVOs) and 12 ischemic CRVOs (ICRVOs, >30 disk diameters of retinal capillary nonperfusion). 21 Of the 45 patients, 34 (75.6%) had hypertension, 18 (40%) had hyperlipidemia, 6 (13.3%) had diabetes mellitus, 3 (6.7%) had a history of myocardial infarction, and 1 (2.2%) had a history of a transient ischemic attack. Of the 45 patients, 4 (8.9%) had previously undergone intravitreal TA treatment, 3 (6.7%) had undergone panretinal laser photocoagulation, and 1 (2.2%) had intravitreal bevacizumab treatment previously. Baseline mean ETDRS-VA was 40.9 letters, ranging from 23 to 70 letters, and baseline mean 1-mm CRT was 572.3 μm (range: 383–907 μm), as measured by OCT.
Early follow-up
After 1 month of follow-up, mean BCVA had significantly to increased 47.6 letters (+6.7 letters; P=0.02), whereas mean CRT had decreased to 392.8 μm (−179.5 μm; P<0.001). At months 3 and 6, BCVA improved further to 53.5 letters (+12.6 letters; P=0.001) and 57.9 letters (+17.0 letters; P<0.001), respectively. CRT measurements at 3 and 6 months after the first injection demonstrated a highly significant reduction in mean CRT to 342.6 μm (−229.7 μm; P<0.001) and 333.5 μm (−238.8 μm; P<0.001), respectively. After 1 year of follow-up, mean BCVA had increased to 61.4 letters (+20.5 letters; P<0.001) and retinal thickness had decreased to 298.0 μm (−274.3 μm; P<0.001).
Eighteen-month follow-up
At 18 months of follow-up, mean BCVA had improved to 61.9 letters (+21.0 letters; P<0.001), and the mean CRT had decreased to 273.2 μm (−299.1 μm; P<0.001). Figures 1 and 2 show the mean changes in BCVA and CRT up to month 18. There was a statistically significant correlation of improvement in BCVA and decrease in CRT (r=−0.33, P=0.02). Of the 45 eyes, 27 (60%) had improved BCVA (≥15 letters) and 17 (37.8%) had stable BCVA when compared with baseline (Fig. 3). An angiographic example responding favorably to intravitreal bevacizumab therapy is shown in Fig. 4. There was 1 eye (2.2%) with a loss of 15 letters or more at 18 months. That eye had a 19-letter loss; it had undergone panretinal laser photocoagulation at 4 months before study enrollment. A severe recurrence of macular edema occurred in this patient, who initially showed a significant decrease in retinal thickness by OCT and associated improvement in BCVA after the start of bevacizumab injections through month 12 (Fig. 5). However, during follow-up from month 13 to month 18, this patient developed recurrent macular edema with an associated vision loss, despite continued bevacizumab treatment. As part of an extension study, this patient underwent vitrectomy with internal limiting membrane removal at 19 months, resulting in anatomical and BCVA improvement (data not shown). The patients received a mean number of 9.8 injections (median: 11). Twelve eyes (26.7%) required continuous treatment up to month 18. Four eyes (8.9%) received only 3 initial treatments and no further retreatment.
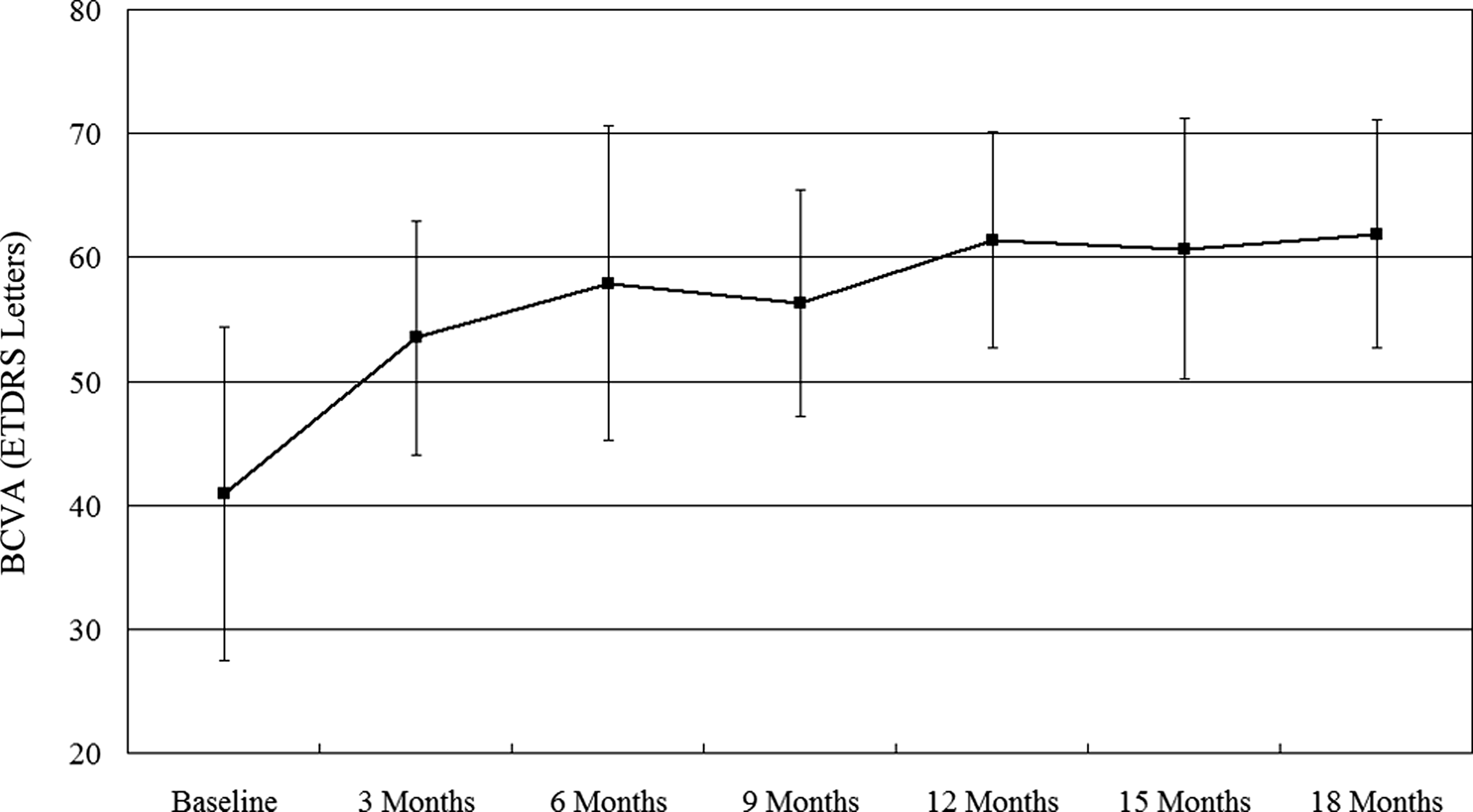
Mean change in best-corrected visual acuity (BCVA) from baseline to month 18. Error bars represent mean and 95% confidence intervals.
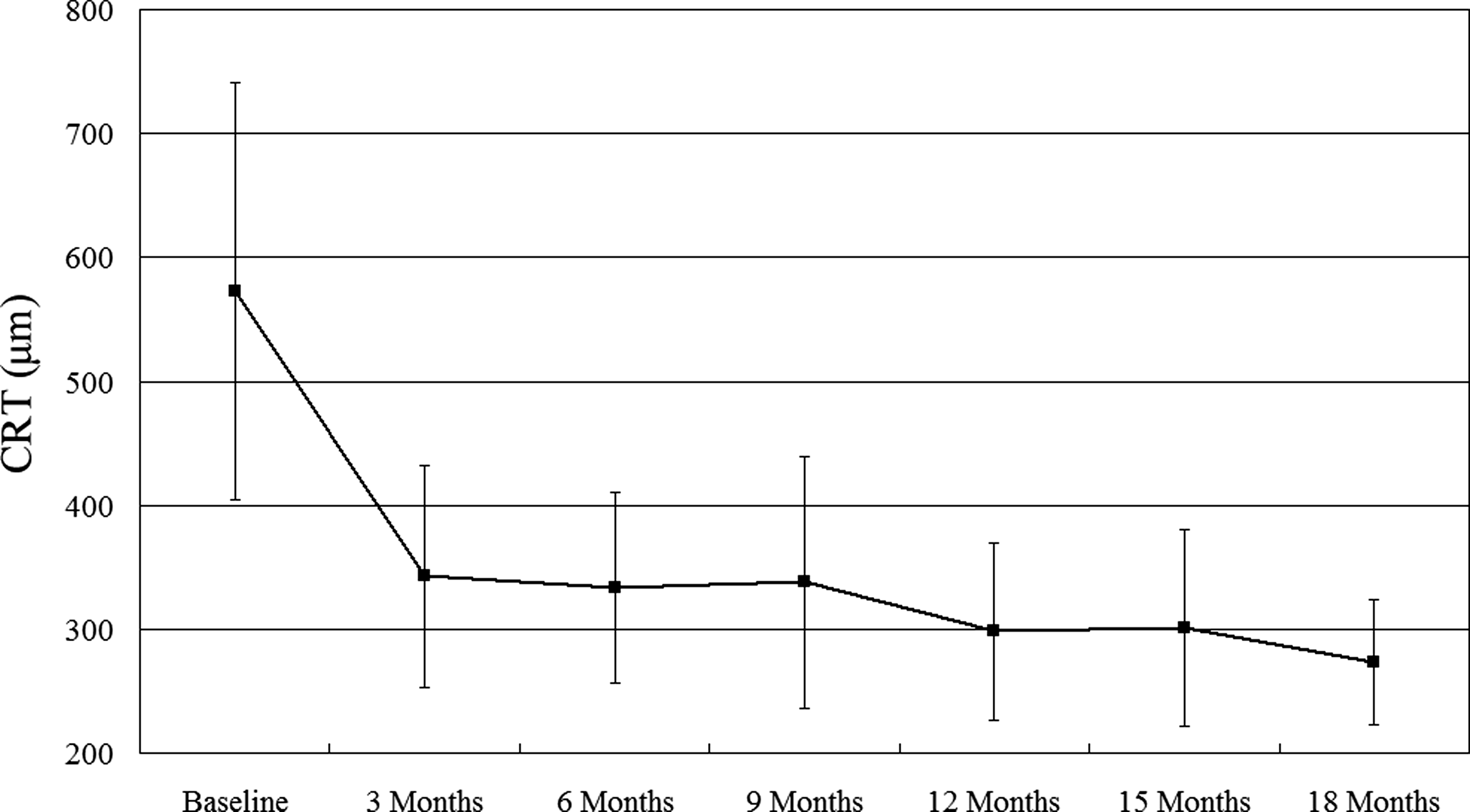
Mean change in central retinal thickness (CRT) from baseline to month 18. Error bars represent mean and 95% confidence intervals.
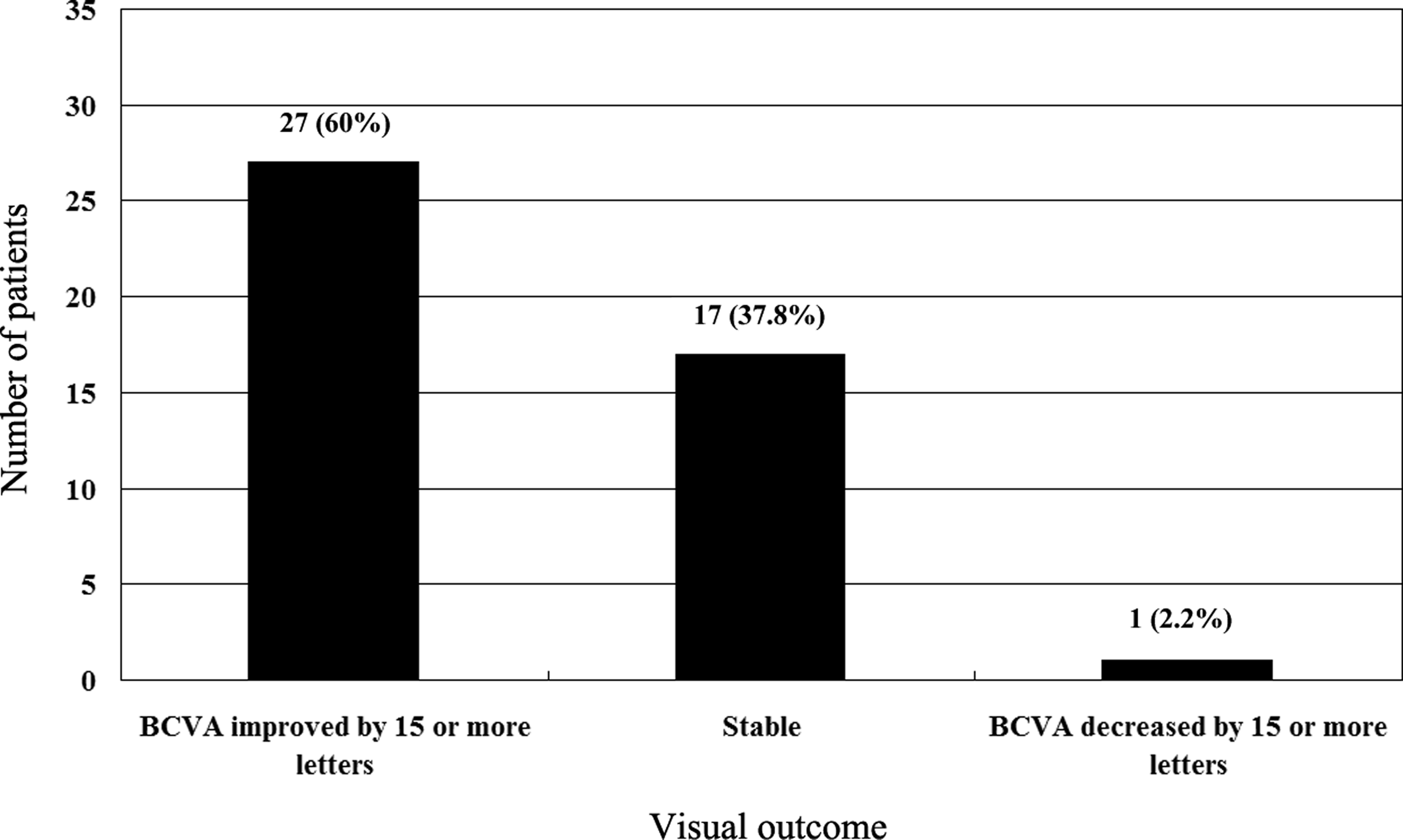
The number of patients (percentage) with improved (≥15 letters), stable, or deteriorated (≥15 letters) vision at the 18-month follow-up.

Images obtained from a 63-year-old woman with central retinal vein occlusion (CRVO) in the left eye with VA reduced to 36 letters.
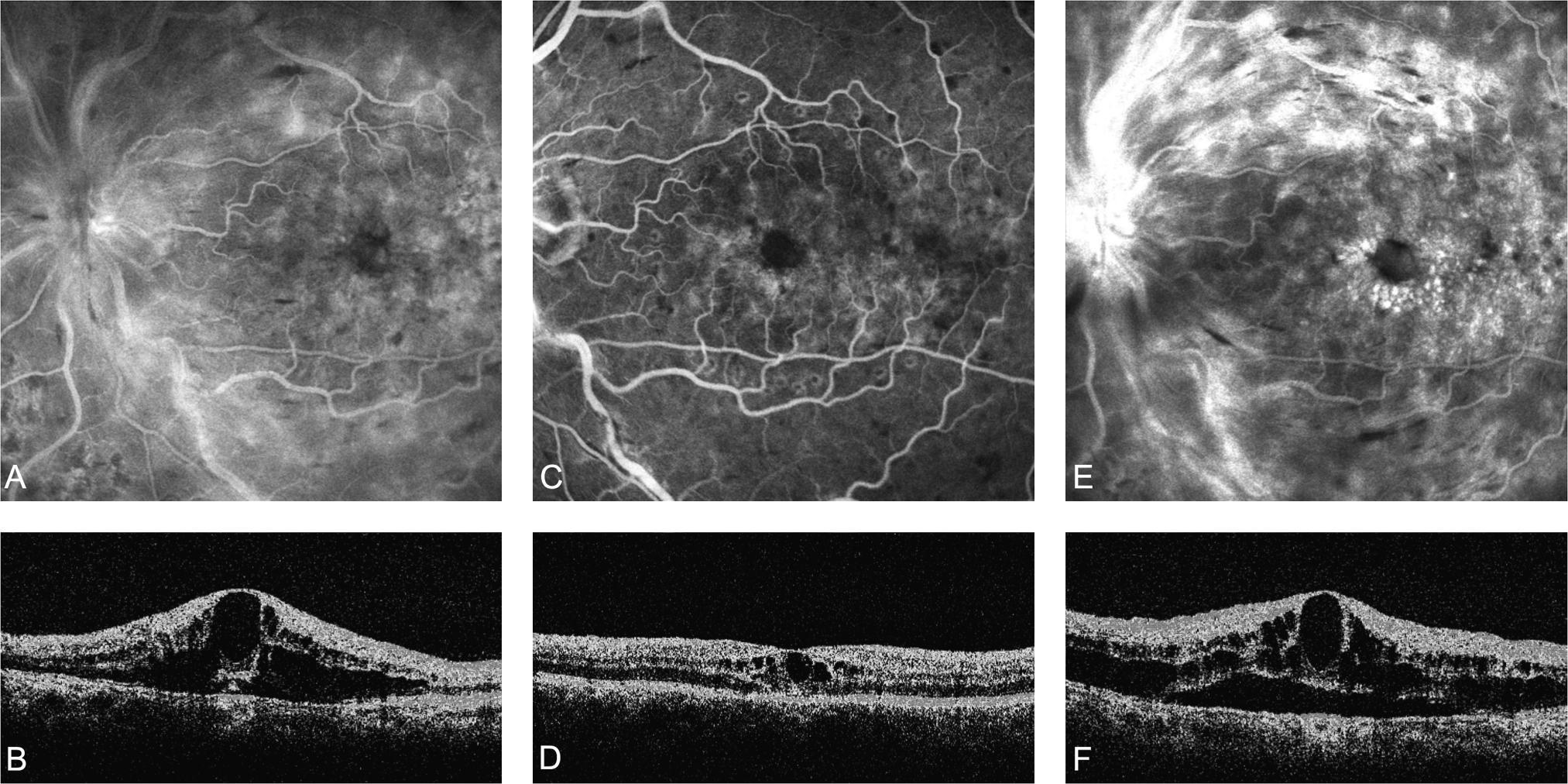
Images obtained from a 48-year-old man with CRVO in the left eye, for which he had undergone panretinal laser photocoagulation at 4 months before study enrollment.
An analysis to reveal predictive factors for outcome found no significant correlation between the duration of CRVO and improvement of BCVA (r=−0.03; P=0.81) or the decrease in CRT (r=0.06; P=0.67). Further, neither the patient's age (r=0.11; P=0.19), baseline BCVA (r=−0.1; P=0.21), nor baseline CRT (r=0.22; P=0.12) appeared to have any predictive effect on BCVA outcome.
Adverse events
After 18 months of follow-up, no patient experienced a severe ocular (endophthalmitis, retinal detachment, and uveitis) or nonocular (thromboembolic event and systemic hypertension) adverse event that was attributable to bevacizumab. No progression of avascular areas according to FA was observed. No patient developed neovascularization of the iris or angle, of the optic disc, or elsewhere in the retina.
Discussion
As anti-VEGF therapy has been approved for the therapy of neovascular age-related macular degeneration (AMD), this approach seems promising for treatment of other ocular diseases associated with VEGF, such as CRVO. The 2 anti-VEGF drugs most commonly used are bevacizumab and ranibizumab (Lucentis; Genentech). Bevacizumab is a full-length anti-VEGF antibody that has been developed and registered for use in oncology. Ranibizumab is an anti-VEGF antibody fragment specifically designed and approved for ophthalmic use. 22 Both ranibizumab and bevacizumab bind VEGF at the same position; however, they differ in size, affinity for VEGF, speed of clearance from the eye, and cost. 23 Recently, a randomized, sham-controlled clinical trial (the CRUISE Study) has demonstrated the safety and efficacy of intravitreal ranibizumab for the management of decreased vision associated with macular edema due to CRVO. 24 In this phase III trail, mean VA improved by 14.9 letters (0.5 mg ranibizumab) and 12.7 letters (0.3 mg ranibizumab) after monthly intravitreal injections of ranibizumab, versus 0.8 letters in the sham group at 6-month follow-up. However, the high expense of ranibizumab limits its use. Ranibizumab costs ∼$2,000 per dose, whereas bevacizumab, the off-label treatment, costs ∼$50. This cost difference, along with the perceived clinical similarities between these 2 drugs, has led to the widespread use of bevacizumab in the absence of level I evidence. 25 More recently, a head-to-head study, the CATT Study, compared ranibizumab with bevacizumab and revealed equal efficacy of both drugs in the management of noevascular AMD at 1 year. 22 The results of the CATT Study support the continued use of intravitreal bevacizumab as an effective, low-cost alternative to ranibizumab.
Results of our prospective clinical trial at 18 months showed that intravitreal bevacizumab treatment in patients with macular edema secondary to CRVO was associated with a significant improvement in VA (+21.0 letters; P<0.001) and with a marked decrease in retinal thickness (−299.1 μm; P<0.001). Consistent with a decrease in CRT as seen by OCT, FA revealed a reduction in the area of leakage. Avascular areas were stable or had decreased, but did not progress during bevacizumab treatment. During multiple treatments for as long as 18 months, no severe ocular adverse events, such as endophthalmitis, retinal detachment, or uveitis, were detected. No patient showed evidence of severe drug-related systemic adverse events such as arterial thromboembolic events.
The natural history of CRVO is very variable, and the Central Vein Occlusion Study Group has demonstrated that VA at baseline is a strong predictor of final VA after CRVO. 26 Statistical analyses were also done to evaluate potential predictive factors for VA benefit after intravitreal bevacizumab treatment in patients with macular edema secondary to CRVO. In this study, similar to prior studies, 17 statistical analyses failed to identify any association with age, duration of CRVO, baseline VA, or baseline CRT. These data suggest that elderly patients or patients with chronic edema should not be excluded from treatment with intraocular bevacizumab. However, because of the small study sample, further investigation is obviously needed to provide comprehensive information.
Recurrent edema in excess of what was observed at baseline was noted in 1 patient from month 13 to month 18. This patient responded well to the initial monthly injections of bevacizumab; however, during follow-up at month 13, the recurrent macular edema was more pronounced than at initial presentation. Reinjections did not result in an improvement of BCVA and decreased CRT in this patient. These events, described as a rebound phenomenon by Matsumoto et al., may be due to the upregulation of VEGF receptors as a result of the inhibition of the VEGF-A pathway. 27 This patient underwent vitrectomy with internal limiting membrane removal, thereafter resulting in anatomical and BCVA improvement. Vitrectomy decreases levels of VEGF in the vitreous cavity and increases the oxygen concentration at the level of the retina, potentially reducing the stimulus for VEGF production. 28 Removal of the internal limiting membrane might result in decompression of the macular edema and a further improvement in preretinal oxygen tension.29,30 This raises the possibility that combined treatment with bevacizumab and vitrectomy may have a favorable long-term effect.
Even if anti-VEGF treatment provides only symptomatic relief for patients with macular edema secondary to RVO, it showed promising results after 18 months of follow-up. The main drawback of this new treatment modality seems to be the short durability of the therapeutic effect, resulting in the need for frequent retreatment. Three injections were not sufficient in achieving long-term benefit in 91.1% of our patients, and 26.7% of all patients showed no complete resorption of macular edema despite continuous treatment up to month 18. A major unanswered question is the duration of treatment that will be needed. It is important to determine whether and when injections can be terminated without further occurrence of macular edema. Histopathological studies show that the occlusion of the central retinal vein is located at the region of lamina cribrosa, where thrombosis is a major feature. In the majority of cases, the thrombus will be recanalized, allowing some circulation, but this recovery phase may take a long time, and often by this time the potential for visual recovery has been lost because of irreversible changes in the macular region, such as chronic macular edema and varying degrees of ischemia. 31 Frequent anti-VEGF retreatment can reduce macular edema and prevent or reverse the excessive intravascular proliferation of endothelial cells to stabilize avascular areas, 32 avoiding chronic macular edema and ischemia. Accordingly, we hypothesize that anti-VEGF treatment may be more beneficial in the cases where recanalized channels are developing well and will eventually lead to normalization of retinal circulation, and there will be an endpoint of the treatment. On the other hand, in the cases where the circulation remains insufficient, there may be not a clearly defined endpoint. This hypothesis may explain the results in the 26.7% of our patients who needed continuous treatment after month 18. Large, randomized, controlled clinical trials should be conducted to evaluate the long-term efficacy and safety after repeated anti-VEGF therapy in patients with macular edema secondary to CRVO, and these may provide a definitive answer as to the usefulness of intraocular bevacizumab or ranibizumab in these conditions.
Footnotes
Author Disclosure Statement
The authors reported no conflicts of interest and are solely responsible for the content and writing of this article.