
Abstract
Abstract
Purpose:
To determine the most appropriate methods for assessing the potential effectiveness of the newer topical fluoroquinolones gatifloxacin, moxifloxacin, and besifloxacin.
Methods:
This article is based on a literature search for published articles about the pharmacokinetic (PK) and pharmacodynamic (PD) characteristics of and measure of bacterial susceptibility to topical ophthalmic fluoroquinolones. Search terms included fluoroquinolones, susceptibility, resistance, minimal/minimum inhibitory concentration (MIC), PDs, PKs, and ocular, ophthalmic, or topical antibiotics.
Results:
Topical fluoroquinolones, particularly besifloxacin, gatifloxacin, and moxifloxacin, have become important treatment options for common ocular bacterial infections due to their broad-spectrum bactericidal activity and low toxicity. An important challenge in ophthalmology is identifying the most accurate in vivo and in vitro methods for evaluating the efficacy of these topical fluoroquinolones. The MIC is the most commonly used measure of in vitro susceptibility. In systemic therapy, this measure is combined with PK data of antibiotics to generate PD indices PK/PD whose breakpoints differentiate clinically susceptible from nonsusceptible bacterial pathogen populations. PD breakpoints are further tested in prospective studies for their ability to predict clinical efficacy. However, it is not known whether systemically derived breakpoints apply to the assessment of clinical susceptibility to ocular agents. Topical ocular antibiotics likely achieve higher concentrations at the target site than do systemically administered antibiotics, but these higher concentrations can be quickly reduced by reflex tearing and blinking induced by instillation. Hence, studies have been conducted in animals and humans to determine the PK concentrations of topically administered antibiotics in ocular compartments. When combined with MIC values for topical pathogens, the results have the potential to predict clinical efficacy after identification of the appropriate PK/PD target. Ocular studies incorporating PK/PD assessments have recently begun to be reported with newer fluoroquinolones, including besifloxacin, gatifloxacin, and moxifloxacin, whose prolonged contact time and potent bactericidal activity have translated into some of the most favorable PK/PD target values. However, the clinical relevance of these studies has yet to be determined.
Conclusion:
There is still a clear need for predictive models to extend our understanding of the clinical susceptibility of ocular pathogens.
Introduction
Although a large amount of data are available from animal and human studies about the systemic dosing of antibiotics in infectious diseases, these data have limited value in the design of topical dosing regimens. Topical antibiotics are confined to surface areas that are not readily comparable to systemic compartments. Therefore, it is difficult to translate our understanding of the efficacy of an antibiotic's dosing regimen when systemically administered against a pathogen into effective treatment of a topical ocular infection caused by the same strain.
This article assesses the unique challenges of evaluating the microbial susceptibility and potential clinical efficacy of topical ocular antibiotics, especially the fluoroquinolones. Topical fluoroquinolones are frequently used in the treatment of ocular bacterial infections due to their broad spectrum of activity, potent bactericidal activity, and low rates of adverse events.1–3 Fluoroquinolones with a topical formulation(s) include ciprofloxacin, gatifloxacin, levofloxacin, moxifloxacin, ofloxacin, and the newly approved besifloxacin. All these agents except besifloxacin (developed solely for topical use) are or have been systemically used (although gatifloxacin and ofloxacin are no longer available for systemic use in the United States) for infectious diseases such as community-acquired pneumonia, acute sinusitis, urinary tract infections, and skin surface infections.4–7
This article is based on a search of MedLine for published articles about the PK and PD characteristics of the newer topical ophthalmic fluoroquinolones, and in vitro and clinical measures of bacterial susceptibility to these antibiotics. Search terms included fluoroquinolones, susceptibility, resistance, minimal or minimum inhibitory concentration (MIC), PDs, PKs, and ocular, ophthalmic, or topical antibiotics. This article is not intended to be a systematic review of the literature on these subjects. Rather, it provides an overview of relevant published literature and a discussion of data highlighting the challenges and progress in predicting bacterial and clinical response to topical ophthalmic antibiotics, with a focus on the newer fluoroquinolones gatifloxacin, moxifloxacin, and besifloxacin.
In Vitro Assessment of Microbial Susceptibility
Before addressing the challenges surrounding ocular antibiotic susceptibility assessments, it is helpful to review the basic premises in the development of susceptibility guidelines for systemically administered antibiotics. The most commonly used method for evaluating in vitro antimicrobial activity is through assessment of the MIC.8,9 The MIC measures the intrinsic activity of an antibiotic against an organism, and is determined through broth or agar dilution or gradient diffusion. 9 The MIC50 and MIC90 refer to the lowest concentrations of a drug that prevent visible growth of bacteria in 50% and 90%, respectively, of tested strains in vitro. 10 The assessment of MIC is a rapid (∼24 h after pathogen isolation) method employed as a first step in evaluating the susceptibility of bacterial isolates. Standardized methods established by international standards-setting groups such as the Clinical and Laboratory Standards Institute and European Committee on Antimicrobial Susceptibility Testing help ensure that different laboratories assess MICs in a reproducible manner.11,12
Table 1 presents MIC90 values for besifloxacin, moxifloxacin, and gatifloxacin against common ocular pathogens. The MIC values can help to distinguish susceptible bacterial populations from populations with acquired or selected resistance. 9 From a clinical standpoint, however, MIC assessments are static determinations performed in a controlled in vitro setting and do not account for the in vivo PK and PD characteristics of a drug. As such, MIC values alone are insufficient as sole predictors of clinical efficacy. 8
MRSA-CR, methicillin- and ciprofloxacin-resistant S. aureus; MRSE-CR, methicillin- and ciprofloxacin-resistant S. epidermidis; MIC, minimal inhibitory concentration.
Incorporating PK and PD Characteristics into Clinical Susceptibility Breakpoints
It has become evident in recent decades that PK data, combined with MIC data, play an important role in predicting antibacterial efficacy in various infection models.14–16 PDs is the study of the in vivo pharmacologic effect of a drug, and is inter-related with the PK or concentration patterns over time of a drug within the target tissue. When the 2 principles are linked and correlated, they are referred to as PK/PD, which provides a better picture of drug effect over time (Fig. 1). 9
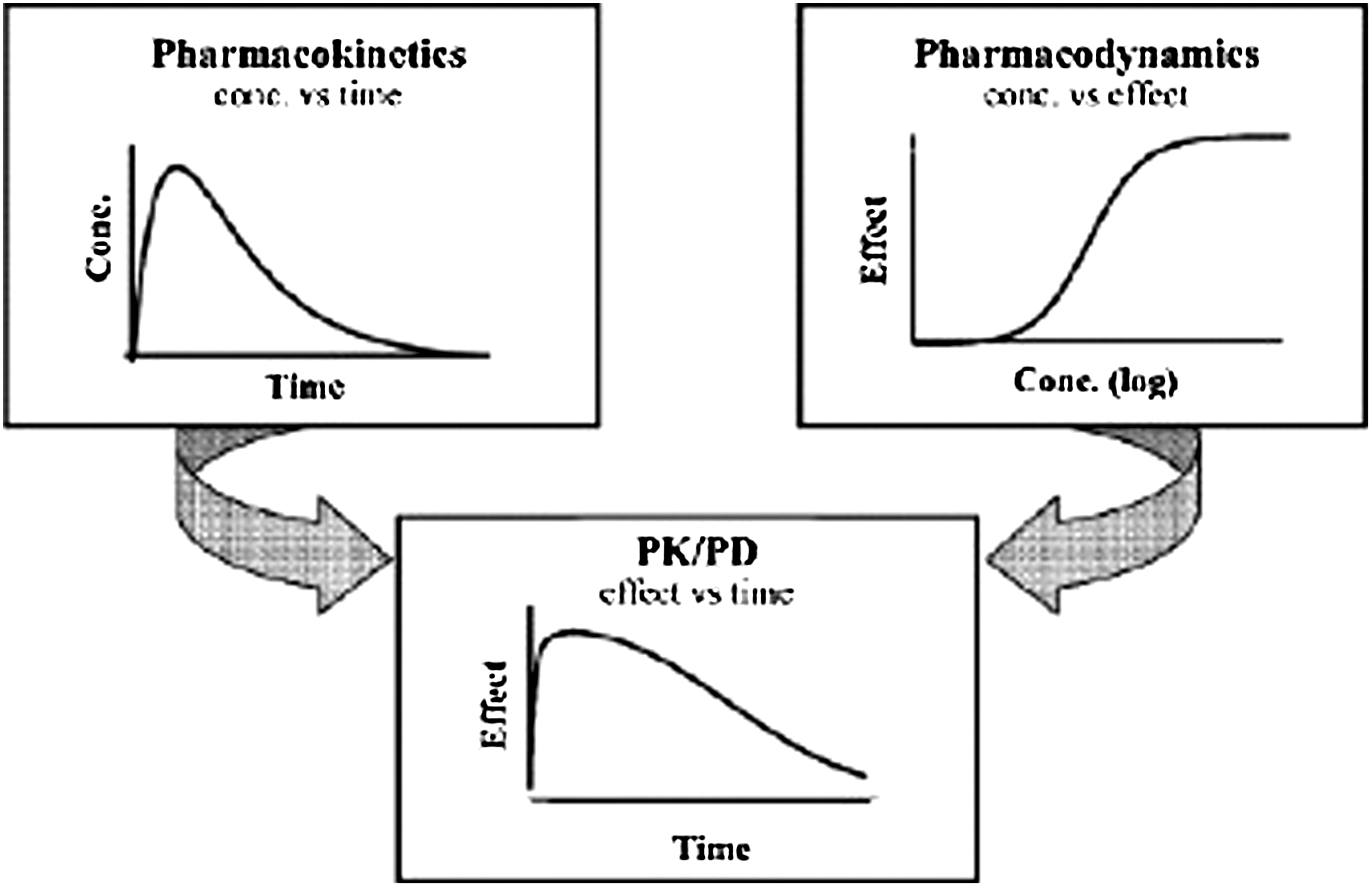
Pharmacokinetic (PK) and pharmacodynamic (PD) modeling as a combination of the classic pharmacological disciplines of PKs and PDs. 13
Various PK/PD indices can be used to determine clinical susceptibility breakpoints. For years, studies in animal models investigated the relationships between PK/PD indices and antimicrobial efficacy, with the conclusion that different classes of antibiotics have PK/PD indices that are predictive of efficacy.17–19 In part, this reflects unique mechanisms of action (eg, whether more time dependent or concentration dependent) as well as the size and duration of postantibiotic effect, or the delay in bacterial growth that occurs when the drug concentration at the site of infection falls below the MIC.9,20,21
The PK/PD indices that have been found to be the best predictors of clinical efficacy include the maximum plasma drug concentration (Cmax) ratio to MIC (Cmax/MIC), the plasma concentration time curve (AUC or exposure) ratio to MIC (AUC/MIC), and the percentage of time during which the antibiotic concentration remains above the MIC (T > MIC or %T > MIC).8,9 The Cmax is the maximum, or peak, drug concentration achieved in the target tissue after each dose, and AUC is the area under the concentration-versus-time curve, often specified for a 24-h period (AUC(0–24)). These calculations should be based on free, unbound antibiotics and are often designated as fAUC and fCmax. Additionally, MIC90 rather than MIC50 values should be used in the calculation of PK/PD indices to include the majority of potentially causative bacterial strains. PK and PD indices calculated with MIC50 values are of little use clinically and are misleading.
Studies looking at relationships between systemic antibiotic PK parameters and bacterial killing have generally used animal models of infection, such as the mouse pneumonia model or the neutropenic mouse thigh model. However, models using immunocompetent animals have also been used.8,9,17–19,22 These studies have suggested that different antibiotic classes have different PK/PD indices predictive of efficacy.17–19 For fluoroquinolones, which have concentration-dependent bactericidal activity, AUC/MIC and Cmax/MIC ratios appear to be the best PK/PD indices predictive of efficacy.8,9,21,23 For example, Fig. 2 depicts the findings of an in vitro infection model study of gatifloxacin against Salmonella isolates in which bacterial killing was plotted against 3 PK/PD indices. 14 Strong correlations were seen between bacterial kill rates and both fAUC(0–24)/MIC (R 2 =0.96) and fCmax/MIC (R 2 =0.93) and were evident for both gatifloxacin-susceptible and -resistant strains Although this study was performed by using systemic administration assumptions, it illustrates the relative significance of various PK/PD indices for fluoroquinolone antibacterial effect regardless of administration route.
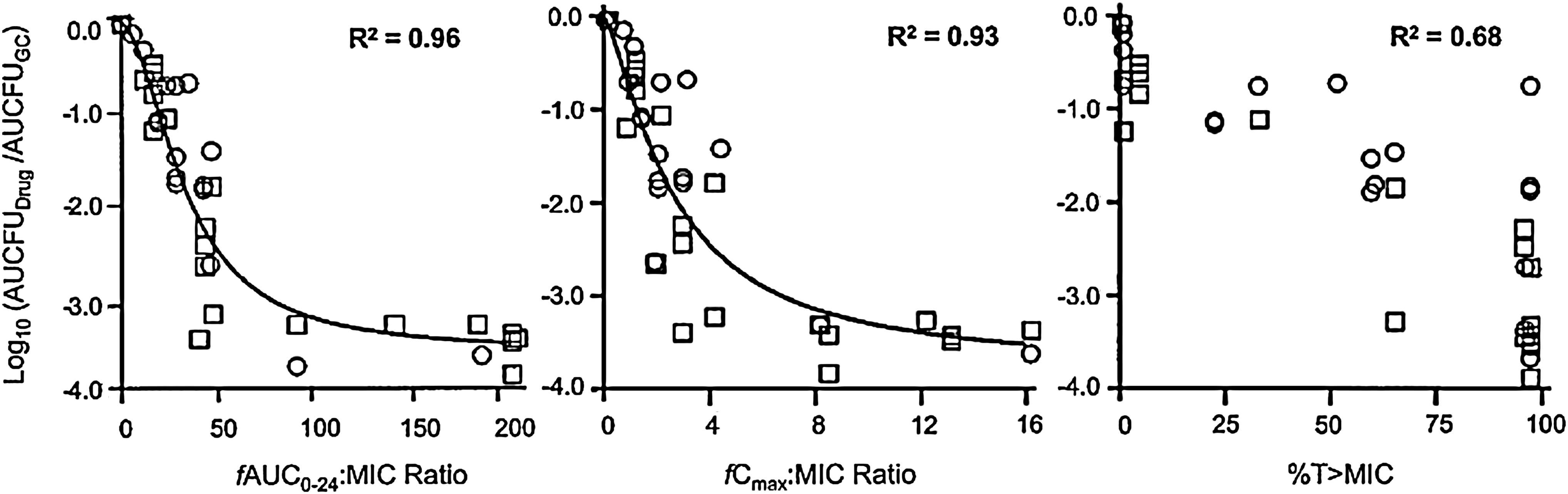
Relationships between various PK/PD indices for gatifloxacin (fAUC0-24/MIC ratio, fCmax/MIC ratio, and %T > MIC) and changes in bacterial density against 2 strains of Salmonella enterica serotype Typhi with differing MICs. Squares represent a susceptible strain (gatifloxacin MIC of 0.5 μg/mL); circles represent a resistant strain (gatifloxacin MIC of 4 μg/mL). The graphs illustrate that for fluoroquinolones the AUC/MIC and Cmax/MIC ratio are statistically most predictive of bacterial kill. 14 MIC, minimal inhibitory concentration.
Specific PK/PD-based targets continue to be clarified, based on existing and continuing research. In the case of fluoroquinolones, 90% of their maximum efficacy against Gram-negative bacilli appears to be reached at an AUC/MIC ratio of 100–125. 8 Against Gram-positive organisms, a Cmax/MIC90 ratio ≥10 or an AUC(0–24)/MIC90 ratio of 30–50 are considered predictive for efficacy.24–26 Thus, for any given dosing regimen, using an AUC value calculated for a standard patient, an MIC value that results in an AUC/MIC ratio of 100–125 can be designated as a clinical susceptibility PK/PD target for a Gram-negative strain. Similarly, for Gram-positive organisms, the MIC value for which a Cmax/MIC90 ratio of ≥10 is reached would be designated as a clinical PK/PD susceptibility target. Of note, in many cases for fixed PK parameters, the MIC values that attain the PK/PD target are substantially lower than the MIC breakpoints for classic susceptibility determinations (which do not take into account PK/PD targets). Thus, classic use of MIC values as susceptibility breakpoints without considering the target PK/PD indices of the antimicrobial may lead to clinical failure of therapy.
A few clinical studies have been conducted in humans to confirm choices of PK/PD indices from animal models, because these studies would require clinical and microbiological failures in humans and sufficient variation in dosing regimens.9,21 In the few available clinical studies, the selected PK/PD indices and their magnitudes have correlated reasonably well with those derived from animal studies, which strengthens the case for using PK/PD indices in setting clinical susceptibility breakpoints.9,21
Topical Ocular Antibiotics
The concept of using PK/PD-based susceptibility targets has been most thoroughly studied for systemic antibiotic administration and related target tissues. A few studies have been conducted of PK/PD ratios with topical administration in ocular infections, although the same principles could be expected to apply to topical ocular application. Thus far, it appears that PK/PD targets remain fairly consistent across different infection types and body sites. 21 As in other types of infections, individual PK and PD attributes influence the clinical efficacy of a topical ocular antibiotic, but they are inter-related, with none standing alone as a sole predictor of treatment success or failure. For example, poor ocular tissue concentration might be compensated for by potent in vitro activity. Conversely, excellent penetration could elevate the clinical efficacy of an antibacterial with poor in vitro potency. For example, ceftriaxone, which is intravenously used for the treatment of meningitis, has a relatively poor central nervous system penetration (4%–17% of serum concentrations), but has very low MICs against most causative pathogens of meningitis, thus giving it clinical efficacy for this indication. 27
An important step toward clarifying antibiotic PK/PD targets for ocular infections is evaluating attainable drug concentrations in the relevant ocular tissue compartment(s) (eg, tears/conjunctival concentrations for conjunctivitis or conjunctival/corneal concentrations for keratitis). The concepts for establishing PK/PD breakpoints are the same for ocular versus systemic administration, but topical ocular anti-infectives are expected to achieve concentrations at the target site much greater than with systemic administration, although ocular concentrations may not be sustained for long because of reflex tearing and blinking.28–33 The newer fluoroquinolones (eg, besifloxacin, gatifloxacin, and moxifloxacin) achieve high concentrations in the tears, conjunctiva, and cornea, but poorly penetrate the aqueous humor (Table 2).28,30,33–44 They also display rapid kill rates (under in vitro conditions) for most ocular infections, with almost all of the bactericidal activity occurring within the first few minutes or, in some cases, hours.41,45–47
Studies represent a sample of published pharmacokinetic data, and are not intended to be an exhaustive summary of relevant literature on this topic.
Single topical administration.
Repeated topical administration.
Four doses, applied at 10-min intervals; mean values obtained 30 min following last dose.
NA, not available.
PK/PD-Based Target Data With Topical Ocular Fluoroquinolones
To date, very few studies have looked at PK/PD-based targets for ocular infection indications, and those studies that have investigated this area were conducted with the newer fluoroquinolones besifloxacin, gatifloxacin, and moxifloxacin. In one human study, concentrations of besifloxacin in human tears relative to MIC90 against 4 common ocular pathogens (Streptococcus pneumoniae, Staphylococcus aureus, Staphylococcus epidermidis, and Haemophilus influenzae) were determined in 64 healthy volunteers. 33 After a single instillation of besifloxacin ophthalmic suspension 0.6% in the conjunctival sac of each eye, a single tear sample was collected at 1 of 8 predetermined sample times over 10 min to 24 h. Mean besifloxacin concentrations in human tears peaked 10 min after dosing with a Cmax of 610 mcg/g, and were 46.4 mcg/g at 8 h, 10.6 mcg/g at 12 h, and 1.60 mcg/g at 24 h postdosing. Total besifloxacin exposure in tears (mean AUC(0–24)) was 1,232 mcg×h/g. Best-fit model parameters from the PK model were used to simulate ocular concentration versus time profiles for besifloxacin as a function of time with 1, 2, and 3 times daily dosing regimens. The AUC(0–24)/MIC90 and Cmax/MIC90 ratios were calculated based on simulated AUC(0–24) values, experimental Cmax values, and MIC90 values previously reported for besifloxacin against relevant ocular pathogens. The results showed that besifloxacin achieved sustained tear concentrations well above the MIC90 values for all 4 pathogens and PK/PD ratios exceeding those associated with bacterial eradication in vivo (Table 3). 33 Subsequent clinical studies demonstrated that besifloxacin administered twice or thrice a day was effective in the treatment of bacterial conjunctivitis.48–51
Target PK/PD Ratios for Gram Positive Organisms: Cmax/MIC90 ≥10 and AUC(0–24)/MIC90 ≥30–50; Target Ratio for Gram Negative Organisms: AUC(0–24)/MIC90 ≥100–125. 33
Calculations based on besifloxacin Cmax (observed) of 610 mcg/g.
Calculations based on besifloxacin AUC(0–24) (predicted) for once-daily, twice-daily, and thrice-daily doses of 1,263, 2,498, and 3,801 mcg×h/g, respectively.
QD, every day; BID, twice a day; TID, 3 times a day; AUC, area under the curve; Cmax, maximum plasma drug concentration; PK, pharmacokinetic; PD, pharmacodynamic.
PK characteristics of besifloxacin ophthalmic suspension 0.6%, moxifloxacin ophthalmic solution 0.5%, and gatifloxacin ophthalmic solution 0.3% were evaluated in ocular tissue of rabbits. 35 Tissue concentrations of each drug in the tears, conjunctiva, cornea, and aqueous humor were measured at predetermined time intervals for 24 h after a single topical administration. These values were compared against the in vitro MIC90 values of methicillin- and ciprofloxacin-resistant S. aureus and S. epidermidis. 35 As shown in Fig. 3, besifloxacin achieved an AUC(0–24)/MIC90 ratio of ∼800 in tears, whereas values were ≤10 for moxifloxacin and gatifloxacin. 35 The relatively high concentrations of besifloxacin in tears may be attributed in part to the formulation of this suspension with a mucoadhesive polymer (DuraSite®, InSite Vision, Inc., Alameda, CA), which is designed to prolong the drug's residence time on the ocular surface. 52 Although AUC(0–24)/MIC90 ratios were <10 for all compounds in the cornea, conjunctiva, and aqueous humor, besifloxacin ratios exceeded those of moxifloxacin and gatifloxacin with ratios of 9.2 in the conjunctiva (vs. ≤1.7 for gatifloxacin and moxifloxacin), 2.1 in the cornea (vs. ≤0.9 for gatifloxacin and moxifloxacin), and 0.13 in the aqueous humor (vs. ≤0.09 for gatifloxacin and moxifloxacin) due to the potent bactericidal activity of besifloxacin against these strains. 35 These results from animal studies are suggestive of a favorable PK/PD profile for besifloxacin against fluoroquinolone-resistant staphylococci. The increasing incidence of antibiotic resistance among ocular pathogens, which was reflected in the choice of bacteria for this study, demonstrates the continuing need for the development of anti-infective agents with improved activity against or with better ocular penetration of drug-resistant bacteria.53,54
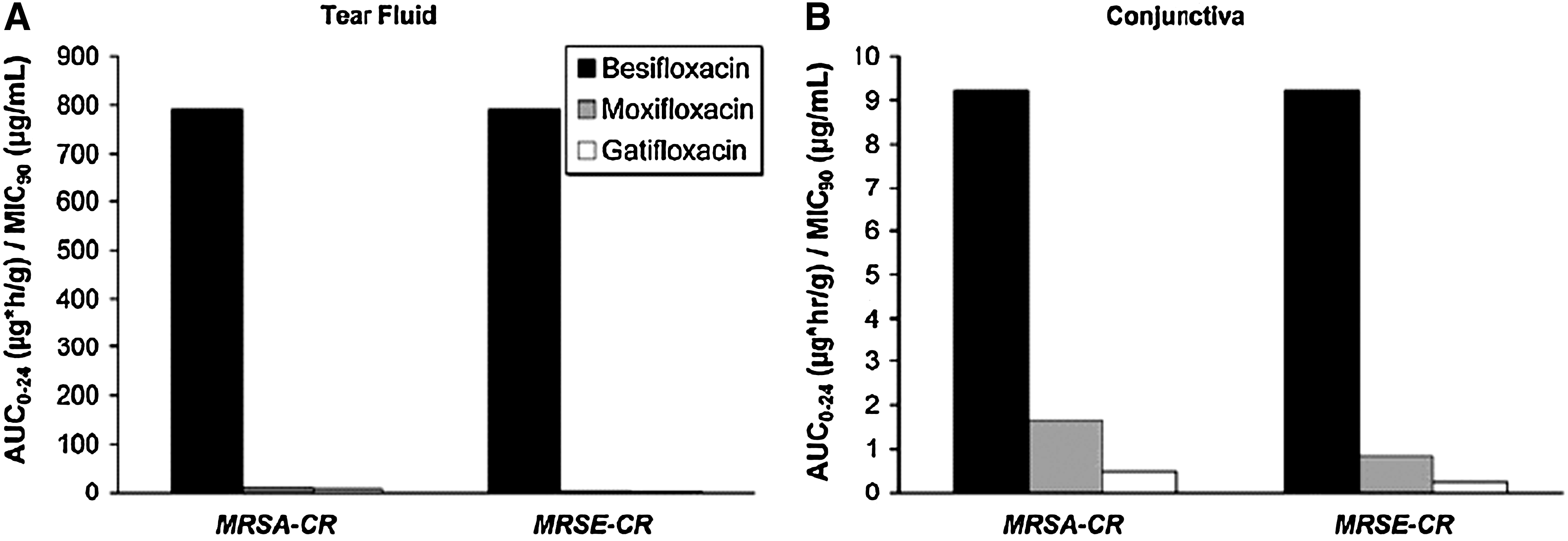
AUC0–24/MIC90 ratios for besifloxacin, gatifloxacin, and moxifloxacin for fluoroquinolone-resistant organisms in tear fluid
In pigmented rabbits, topical administration of a single dose of besifloxacin 0.6% resulted in Cmax values of 2,760, 62.8, and 7.21 mcg/g and AUC(0–24) values of 3,240, 92.8, and 8.56 mcg×h/mL for tears, conjunctiva, and cornea, respectively.33,41 Conjunctival concentrations of besifloxacin were sustained above the MIC90 for most Gram-negative and Gram-positive organisms for at least 12 h. 41 Importantly, the conjunctival Cmax/MIC90 ratio was >10 for several species of nonresistant bacteria, including H. influenzae, S. aureus, coagulase-negative staphylococcus, and S. pneumoniae, and the AUC/MIC90 ratio was >100 for nonresistant species except for Pseudomonas aeruginosa. 41 Thus, besifloxacin demonstrated in vivo PK/PD ratios suggestive of effective bacterial kill and efficacy against Gram-positive and Gram-negative ocular pathogens.
A recent randomized study evaluated the PK properties of besifloxacin 0.6%, gatifloxacin 0.3%, and moxifloxacin 0.5% in the conjunctival tissue of 6 healthy volunteers after topical application of a single drop. 34 Conjunctival samples were taken periodically up to 24 h after dosing. All 3 fluoroquinolones reached a peak mean conjunctival concentration 15 min after dosing. Concentrations of besifloxacin, gatifloxacin, and moxifloxacin were 2.3, 4.0, and 10.7 mcg/g, respectively. Besifloxacin had the longest mean residence time (4.7 h) in conjunctival tissue. All 3 fluoroquinolones reached concentrations in the conjunctiva above the MIC90 of methicillin-susceptible S. aureus and S. epidermidis for at least 2 h, although besifloxacin was the only one to achieve an AUC(0–24)/MIC90 ratio in excess of 100. Besifloxacin also had the greatest AUC(0–24)/MIC90 ratio against methicillin-resistant Staphylococcus organisms, again due in part to its in vitro potency, but did not reach the PK/PD target for these strains.
Additional Ocular Fluoroquinolone Data
Although PK/PD-based susceptibility target data remain scant, a few studies have evaluated only PK characteristics of topically administered antibiotics in ocular tissues of animals35,38 and humans,33,37,55 and compared them against in vitro MIC50 or MIC90 values. Maximum drug concentrations in the aqueous humor (AQCmax) were determined in rabbits after instillation into the conjunctival sac of moxifloxacin 0.5%, gatifloxacin 0.3%, levofloxacin 0.5%, ofloxacin 0.3%, and tosufloxacin 0.3% ophthalmic solutions (3 doses, applied every 15 min). 38 Only moxifloxacin achieved AQCmax concentrations that exceeded the MIC90 values for S. aureus and S. epidermidis isolates (nonresistant isolates), whereas the other fluoroquinolones did not. Based on that criteria alone, the authors concluded that moxifloxacin ophthalmic solution should be sufficiently effective in the treatment of endophthalmitis caused by nonresistant S. aureus or S. epidermidis. 38 However, as previously discussed, a simple comparison of MIC values relative to tissue concentrations alone to predict bacterial kill and clinical efficacy fails to take into account additional PD characteristics such as bactericidal killing patterns of the antibiotic and is not as reliable a predictor of clinical efficacy.
Preoperative dosing with levofloxacin 0.5% (1 to 2 drops, 4 times a day for 2 days) in patients undergoing phacoemulsification resulted in aqueous humor concentrations of 0.28 ng/mL. 56 However, combining this dosing regimen with preoperative pulsed dosing (5 doses every 10 min before surgery) resulted in an aqueous humor concentration of 1.62 ng/mL. 56 Similarly, a different regimen of preoperative dosing combined with postoperative pulsed dosing (5 min apart) with topical levofloxacin 0.5% in patients with cataract resulted in a Cmax of 4.4 (±2.5) mcg/mL in the aqueous humor at 60 min after administration of the last drop. 57 Although this concentration exceeds the MICs of common nonresistant ocular pathogens, 57 it most likely does not reach the PK/PD target, and further studies will be necessary to evaluate the clinical efficacy of such regimens. These findings illustrate the importance of determining a proper dose and dosing interval to achieve desired tissue concentrations and maximize clinical benefit through PK/PD-based targets.
Preoperative dosing (4 times daily starting 2 days before cataract surgery) with moxifloxacin 0.5% or gatifloxacin 0.3% demonstrated greater penetration by moxifloxacin than gatifloxacin into the aqueous humor. Mean concentrations assessed at the beginning of surgery were 2.2 mcg/mL for moxifloxacin and 0.82 mcg/mL for gatifloxacin. By comparison, the concentrations for both drugs reached or exceeded the MIC of common nonresistant ocular pathogens for endophthalmitis. 40 However, as noted with previously cited studies, attainment of PK/PD targets was not evaluated. Another study of topically applied moxifloxacin 0.5% and gatifloxacin 0.3% (2 preoperative doses of 1 drop given 5 min apart) in 50 adult patients undergoing keratoplasty resulted in AQCmax of 0.9 and 0.3 mcg/mL, respectively, and aqueous AUC of 1.2 versus 0.4 mcg·h/mL. 37 More recently, preoperative dosing with moxifloxacin ophthalmic solution 0.5% or besifloxacin ophthalmic suspension 0.6% every 10 min for a total of 4 doses beginning 1 h in patients undergoing routine cataract surgery resulted in mean aqueous humor concentrations of 1.6 and 0.042 mcg/mL for moxifloxacin and besifloxacin, respectively. 42 Although these and other studies58–60 indicate a greater penetration into the aqueous humor by moxifloxacin relative to other fluoroquinolones, aqueous humor concentrations were generally low for all fluoroquinolones and reached the required PK/PD targets only for highly susceptible or nonresistant ocular pathogens. 35 Thus, one would expect that for pathogens with higher MIC values such as MRSA (moxifloxacin MIC90, 8 mg/L) 61 that these drugs would not be effective in killing the bacteria and affecting a clinical cure. Based on the data presented in these studies, it appears that the Cmax/MIC ratios were <10, thus suggesting a low likelihood of clinical success.
A 2-day, open-label study measured levofloxacin concentrations in tears for up to 24 h after a single topical administration of levofloxacin ophthalmic solution 0.5% to 30 healthy adults. 55 Mean concentrations of levofloxacin peaked 15 min after dosing (Cmax=221 mcg/mL) and remained above 6 mcg/mL for up to 6 h. 55 Overall, 67% of subjects at 6 h and 33% at 24 h after administration maintained levofloxacin concentrations exceeding 2 mcg/mL, a concentration greater than the MIC of levofloxacin against most ocular pathogens. 55 Topical administration of levofloxacin resulted in concentrations on the surface of the eye (Cmax of 221 mcg/mL) that were several fold greater than the systemic concentrations attained in usual dosing studies (Cmax of 5.2 mcg/mL). 8 Attainment of PK/PD targets was not reported in this study.
MIC/Clinical Outcome Correlations
Finally, a few studies have attempted to correlate in vitro microbial susceptibility results with clinical outcomes. These studies have generally concluded that treatment with a topical anti-infective agent active against bacteria in vitro correlates with clinical cure in patients infected with the same bacteria, most likely because these high topical concentrations reach effective PK/PD targets. For example, a prospective study of 391 patients with culture-confirmed bacterial keratitis sought to determine whether an association existed between clinical improvement and cure rates with ciprofloxacin treatment and in vitro susceptibility to ciprofloxacin of each patient's principal corneal isolate (ie, the bacteria with the highest MIC for ciprofloxacin). 62 Among infections having an MIC above 1 mcg/mL, rates of clinical improvement and cure were reduced by 43% and 29%, respectively, compared with those with more sensitive isolates. 62
Similar results were seen in a prospective randomized trial that compared the in vitro bacteriologic and clinical efficacy of gatifloxacin 0.3% and ciprofloxacin 0.3% in 104 patients (104 eyes) with bacterial keratitis. During in vitro susceptibility testing, gatifloxacin was active against a significantly higher percentage of S. epidermidis and S. pneumoniae isolates than ciprofloxacin. The number of keratitis ulcers healed by treatment with gatifloxacin (39 eyes, 95.1%) was significantly higher than the number with ciprofloxacin (38 eyes, 80.9%) for ulcers caused by S. epidermidis (P=0.042) and S. pneumoniae (P=0.007). 63 Finally, a review of the clinical outcome and MIC data from 421 patients with bacterial keratitis that sought to correlate the MIC of bacteria against 10 antimicrobials with clinical outcome found significant linear associations between clinical outcomes and MIC for Pseudomonas species (P=0.047), S. aureus (P=0.04), and Enterobacteriaceae (P=0.045) but not for streptococci and coagulase-negative staphylococci. 64
It is worth noting that almost all fluoroquinolones marketed for topical ophthalmic administration are also formulated for systemic use (oral and/or intravenous). As a result, systemic breakpoint data for a broad range of pathogenic bacteria are generally available in addition to ocular pathogens. Consequently, the prescribing information for topical ophthalmic fluoroquinolones contains 2 listings of ocular pathogens predicted to be susceptible to that fluoroquinolone—one listing based on the ocular pathogens successfully eradicated in clinical studies for the indication and a second listing based on microorganisms predicted to be eradicated based on systemic breakpoints. Since besifloxacin is exclusively marketed for ocular administration, the prescribing information for Besivance (besifloxacin ophthalmic suspension 0.6%) contains only one listing.
Conclusions
Systemic susceptibility breakpoints may not be appropriate measures for assessing microbial susceptibility to topical ocular antibiotics, because ocular drug concentrations achieved after topical administration are likely to differ from drug concentrations expected to be systemically attained after systemic administration. Therefore, predictions of therapeutic success against ocular infection are often estimated by comparing nonsystemic, PK characteristics in ocular tissues of relevance with in vitro MIC data. Resulting PK/PD indices provide useful estimates of the ability of an ophthalmic agent to eliminate pathogens from the eye and successfully treat infections, especially when these measurements exceed systemically established PK/PD targets previously shown to be clinically effective. These concepts were not given much attention for ophthalmic application until recently; thus, most relevant data have been generated with newer agents such as besifloxacin, gatifloxacin, and moxifloxacin. Findings reported to date indicate particularly favorable PK/PD ratios for besifloxacin that are probably due to prolonged ocular surface contact time and potent bactericidal activity. However, prospectively designed clinical studies will still be required to validate these assumptions.
Nevertheless, unmet needs include the development of animal models to establish susceptibility breakpoints for topical ocular agents used for various ocular diseases and clinical studies that would validate those ocular breakpoints in the relevant tissues. In the absence of those models and studies, efforts to estimate the topical susceptibility of ocular pathogens will most likely continue to rely on systemic susceptibility breakpoints and ocular PK measures in combination with in vitro MIC testing results.
Footnotes
Acknowledgments
The authors thank Sandra Westra, PharmD, of Churchill Communications for writing and editorial assistance. Bausch & Lomb provided funding to Churchill Communications.
Author Disclosure Statement
The authors declare the following conflicts of interest in relation to this article.
Dr. Bertino reports that he is a consultant with Bausch & Lomb.
Dr. Jones was a paid consultant to Bausch & Lomb in 2010.
Dr. Segreti was a paid consultant to Bausch & Lomb in 2009.
None of the authors received payment for their work in this article.