
Abstract
Abstract
Purpose:
To assess the reversibility of clinical benefits of cyclosporine 0.05% (Restasis®; Allergan, Inc., Irvine, CA) therapy and the therapeutic gain after its delayed use by switching treatment modalities in patients with dry eyes who completed a 1-year course of therapy with artificial tears (Refresh Endura®; Allergan, Inc., Irvine, CA) or cyclosporine 0.05%.
Methods:
This was a single-center, prospective, investigator-masked, longitudinal extension trial. Patients who had been treated with cyclosporine 0.05% in the first year of study were randomized in a 2:1 ratio to either cyclosporine 0.05% (C
Results:
At baseline, most patients with C
Conclusions:
Cyclosporine 0.05% withdrawal led to disease progression, thus indicating the necessity for maintenance therapy. Earlier treatment with cyclosporine 0.05% may result in improved outcomes.
Introduction
The primary driving force behind the advances in dry eye pathogenesis was the epidemiological studies that recognized the increasing importance of dry eye as a public health problem.10–12 These studies also promoted the efforts such as those by the International Task Force (ITF) to standardize dry eye diagnosis and treatment. 13 Using the Delphi consensus technique, the ITF categorized dry eye severity into 4 levels (Table 1), with a range of therapeutic options being appropriated to each level. 13 Given the major role of inflammation in dry eye etiology, anti-inflammatory therapy with cyclosporine 0.05% (Restasis®; Allergan, Inc., Irvine, CA) was recommended for all patients, with or without clinically apparent ocular surface inflammation, starting from disease severity level 2. 13
Disease severity is categorized into 4 levels based on the severity of symptoms and signs. At least one sign and one symptom of each category should be present to qualify for the corresponding level assignment.
In spite of this progress, characterization of dry eye prognosis and its response to common dry eye therapies have received little attention. This primarily stemmed from the lack of a universal dry eye definition, mutual diagnostic methodologies, and treatment consensus. The development of ITF guidelines, however, enabled longitudinal studies to evaluate prognosis of dry eye disease based on a set of consensus criteria. Using the ITF guidelines, a published study showed that patients with dry eyes who received artificial tears (Refresh Endura®; Allergan, Inc., Irvine, CA) had a significantly higher rate of disease progression than those who received cyclosporine 0.05% after a 1-year course of therapy. 14 This finding suggests that dry eye disease is progressive in nature and that cyclosporine 0.05% therapy may slow down or prevent its progression. It is not known whether cyclosporine 0.05% withdrawal undermines the disease stabilization attained by patients in that study or whether a 1-year delay in initiating cyclosporine 0.05% therapy hinders achieving similar levels of clinical benefits in patients with artificial tears. Hence, this study implemented a cross-over design to assess the reversibility of clinical benefits of cyclosporine 0.05% therapy and the therapeutic gain after its delayed use by switching treatment modalities in patients with dry eyes who completed the 1-year course of therapy with artificial tears or cyclosporine 0.05%.
Methods
Study design
This was a single-center, prospective, investigator-masked, longitudinal extension clinical trial. The study was approved by the Western Institutional Review Board in Olympia, WA, and was registered with ClinicalTrials.gov. The primary inclusion criteria were completion of the 1-year course of therapy with cyclosporine 0.05% or artificial tears (Refresh Endura) and a disease severity of level 2 or 3 as defined by the ITF guidelines. 13 Patients were excluded if they had active ocular infection or inflammatory disease or uncontrolled systemic disease. All participating patients signed a written consent form before initiation of the study-specific procedures.
Patients who had been treated with cyclosporine 0.05% in the first year of study were randomized in a 2:1 ratio to either cyclosporine 0.05% or artificial tears (Refresh Endura) in the second year of study. Randomization was performed by a statistical program and was overseen by the research coordinator. All patients who had been originally randomized to artificial tears in the first year of study switched to receive cyclosporine 0.05% in the second year of study. Patients received study drugs twice daily for 12 months starting at the last visit of the first year (month 12), which served as the baseline visit (month 0) for the second year. Patients were subsequently evaluated for outcome measures at months 4, 8, and/or 12. The primary outcome measure was disease progression, and the secondary outcome variables were the changes in dry eye signs and symptoms and conjunctival goblet cell density. All patients were allowed to utilize rescue artificial tears as needed if discomfort was experienced. Patients were told to log their use of additional tears and report their use at the study visits. The study was conducted in compliance with regulations of the Health Insurance Portability and Accountability Act and the Declaration of Helsinki.
Disease severity and dry eye signs and symptoms
Disease severity was assessed according to the ITF consensus guidelines at baseline (month 0) and month 12 (Table 1). 13 Patients were evaluated for signs and symptoms of dry eye by Schirmer I test with anesthesia, tear breakup time (TBUT), ocular surface staining, and Ocular Surface Disease Index (OSDI) at baseline (month 0) and months 4, 8, and 12. In each study visit, TBUT was evaluated first, followed by ocular surface staining and Schirmer test, respectively. The TBUT was measured by using fluorescein dye. Ocular surface damage was assessed by the Oxford method using sodium fluorescein to stain the cornea and lissamine green to stain the nasal and temporal bulbar conjunctiva. The scoring scale for ocular staining was 0 to 5 in the cornea, 0 to 5 in the temporal conjunctiva, and 0 to 5 in the bulbar conjunctiva, with 0 representing no staining and 5 representing severe staining. These individual scores were then summed for the total Oxford score, which ranged from 0 to 15. The symptoms of ocular irritation and their impact on visual functioning was assessed by OSDI, a validated 12-item questionnaire, on a scale of 0 to 100 with 0 representing asymptomatic and 100 representing severe, debilitating dry eye disease The change from baseline in dry eye signs and symptoms was calculated by subtracting the baseline score from the month-4, −8, and −12 scores.
Goblet cell density
The density of goblet cells in the bulbar conjunctiva was evaluated at baseline and month 12. Impression cytology was performed in both eyes after evaluation of TBUT, ocular staining, and Schirmer test. Goblet cells were collected on cellulose acetate filters (HAWP 304 FO; Millipore Corp., Billerica, MA). The filters were fixated in glacial acetic acid, formaldehyde, and 70% ethanol and subsequently stained with a modified periodic acid–Schiff Papanicolaou stain. Goblet cells were counted in 5 (400×400 mm) representative microscopic fields on each filter. 15 The change from baseline in goblet cell density was calculated by subtracting the baseline score from the month 12 scores.
Statistical analyses
The results were presented as mean±SD or the mean percentage change from baseline±SD. Intergroup comparisons of categorical variables were performed by using the chi-square or Fisher exact test. Continuous variables were analyzed by using nonparametric tests (Mann–Whitney tests for between-group comparisons and Wilcoxon-signed rank tests for within-group comparisons). A P value<0.05 was considered a statistically significant difference. Statview software (SAS Institute, Cary, NC) was used for all analyses.
Results
Patient disposition, demographics, and baseline disease severity
Of the 58 patients who had completed the first year of therapy with cyclosporine 0.05% or artificial tears, 50 patients enrolled in the second year of study from December 2007 to January 2008. Out of the 36 patients who had completed cyclosporine 0.05% therapy in the first year of study, 20 patients continued to use cyclosporine 0.05% (C
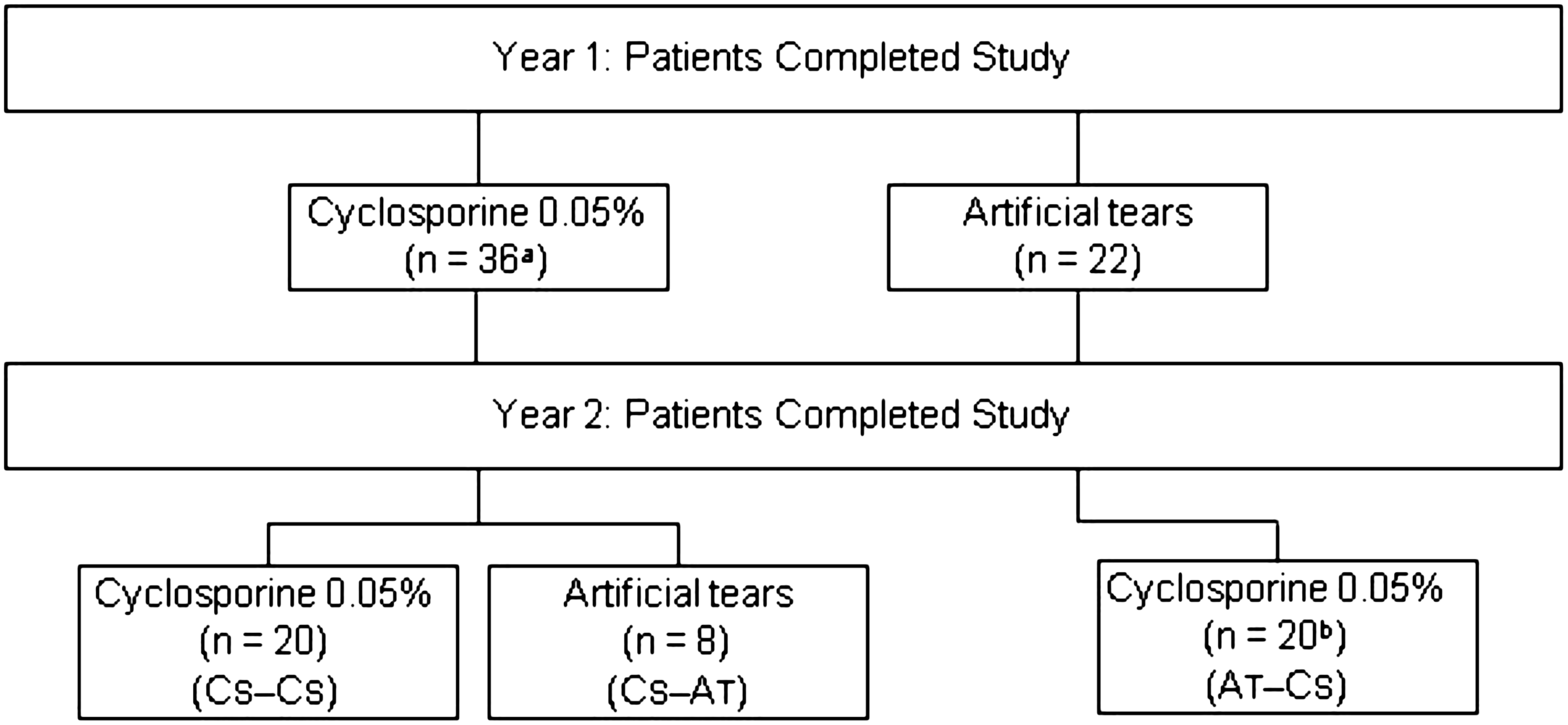
Patient disposition. Patients who had completed cyclosporine 0.05% therapy in the first year of study were randomized to receive cyclosporine 0.05% (C
The mean (SD) age of patients was 47.9±5.1 years in the C
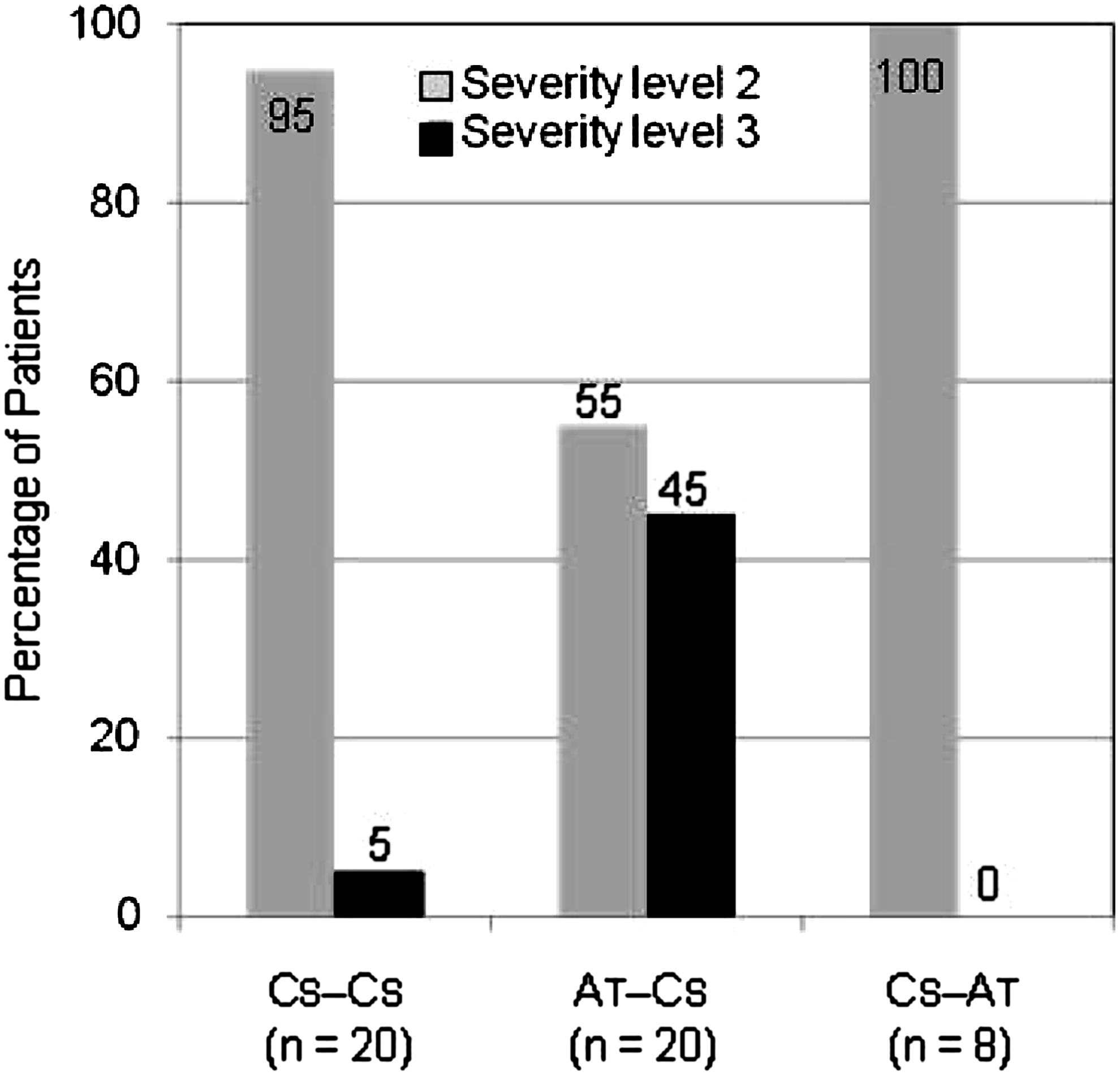
Dry eye severity at baseline. The last visit (month 12) in the first year of study served as the baseline visit (month 0) for the second year of study. At baseline, patients had already completed a 12-month course of treatment with cyclosporine 0.05% or artificial tears. In the second year of study, patients using cyclosporine were randomized to receive either cyclosporine 0.05% (C
Change in dry eye severity
At month 12, a significantly higher percentage of patients with C
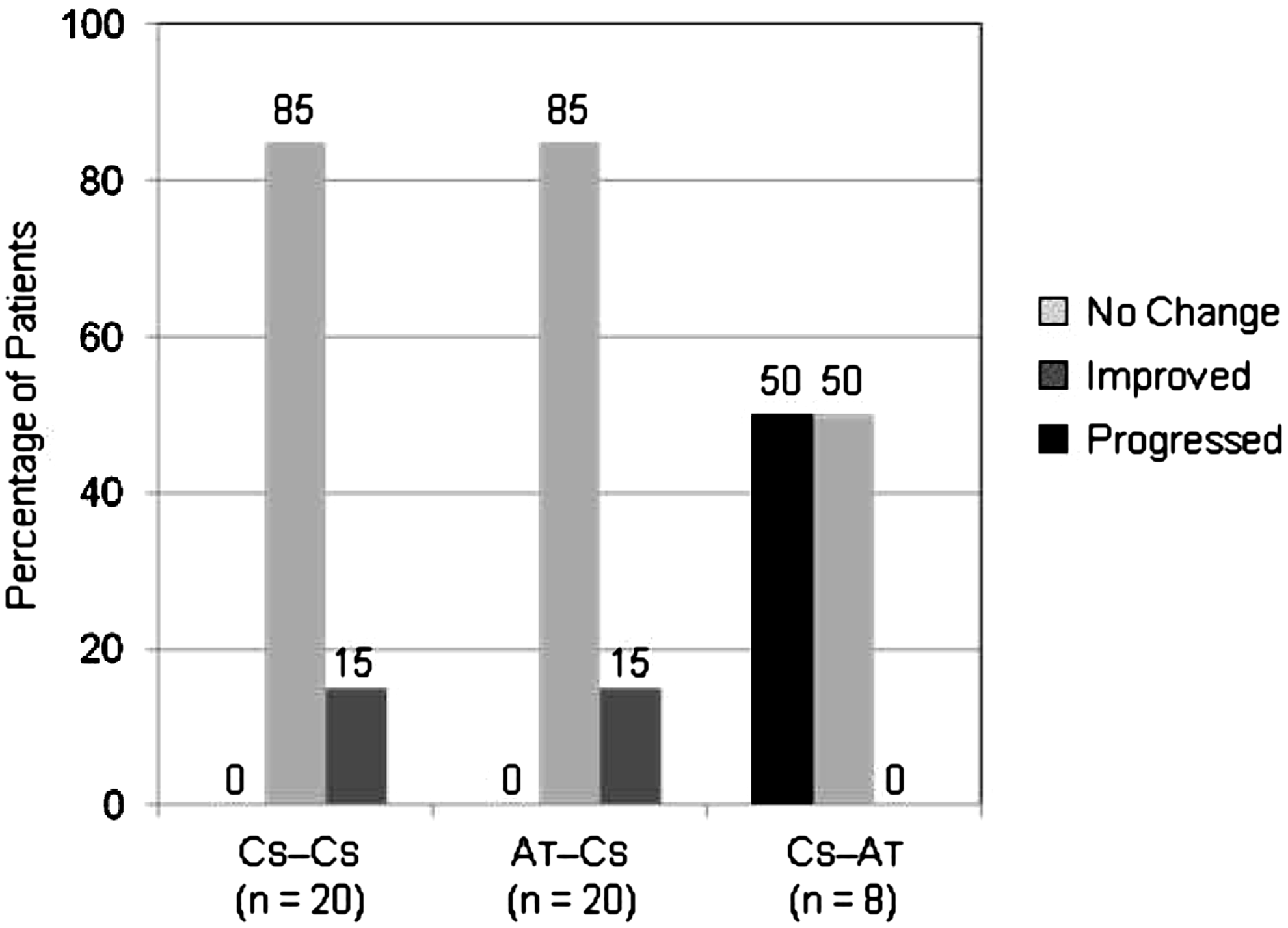
Change in dry eye severity at month 12 compared with baseline. Patients who received cyclosporine 0.05% in the first year of study were randomized to receive either cyclosporine 0.05% (C
Dry eye signs and symptoms
At baseline, patients with C
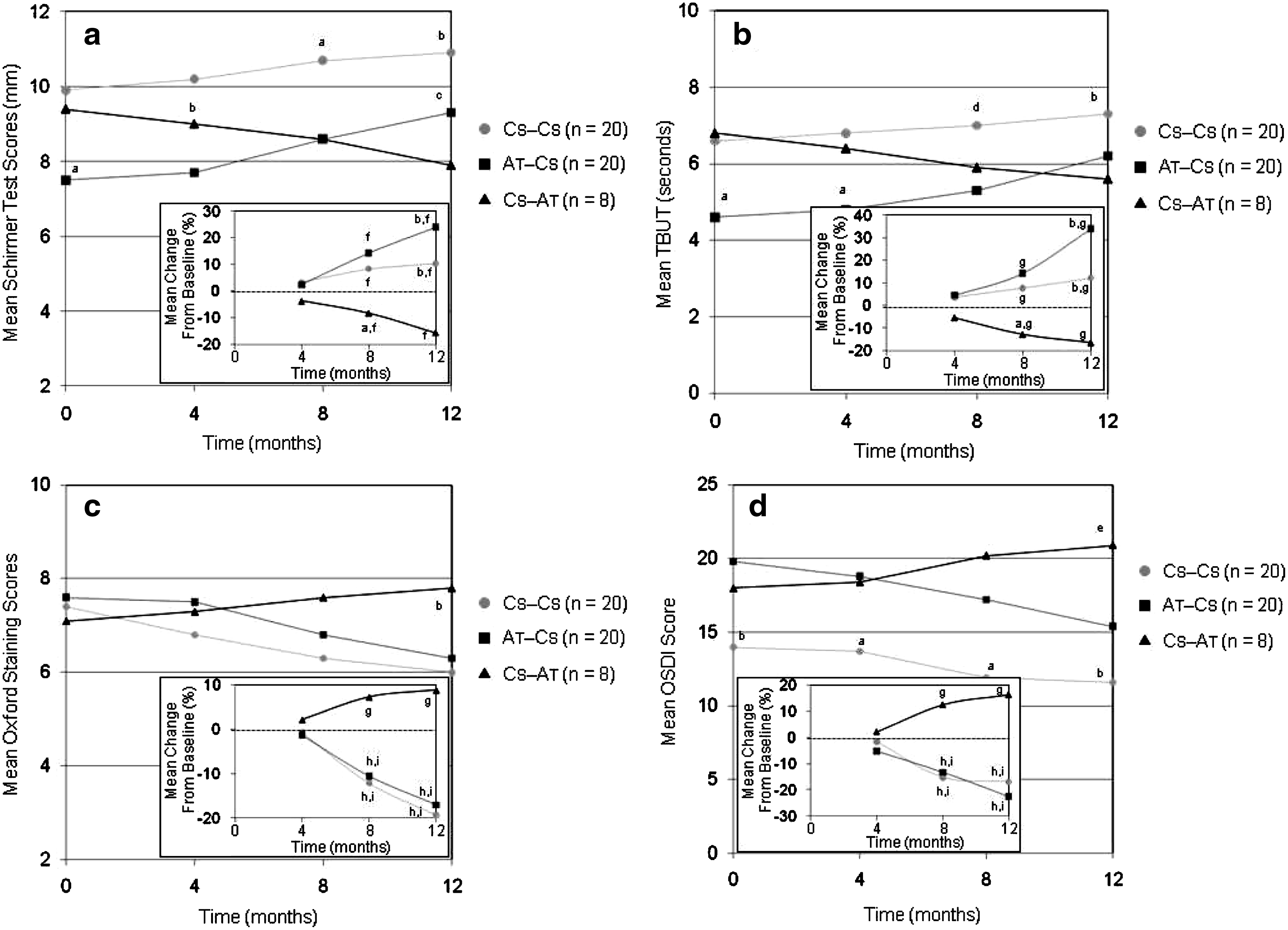
Temporal kinetics of changes in dry eye signs and symptoms. Patients who had received cyclosporine 0.05% in the first year of study were randomized to receive either cyclosporine 0.05% (C
At month 12, patients with C
Goblet cell density
At baseline, patients with C
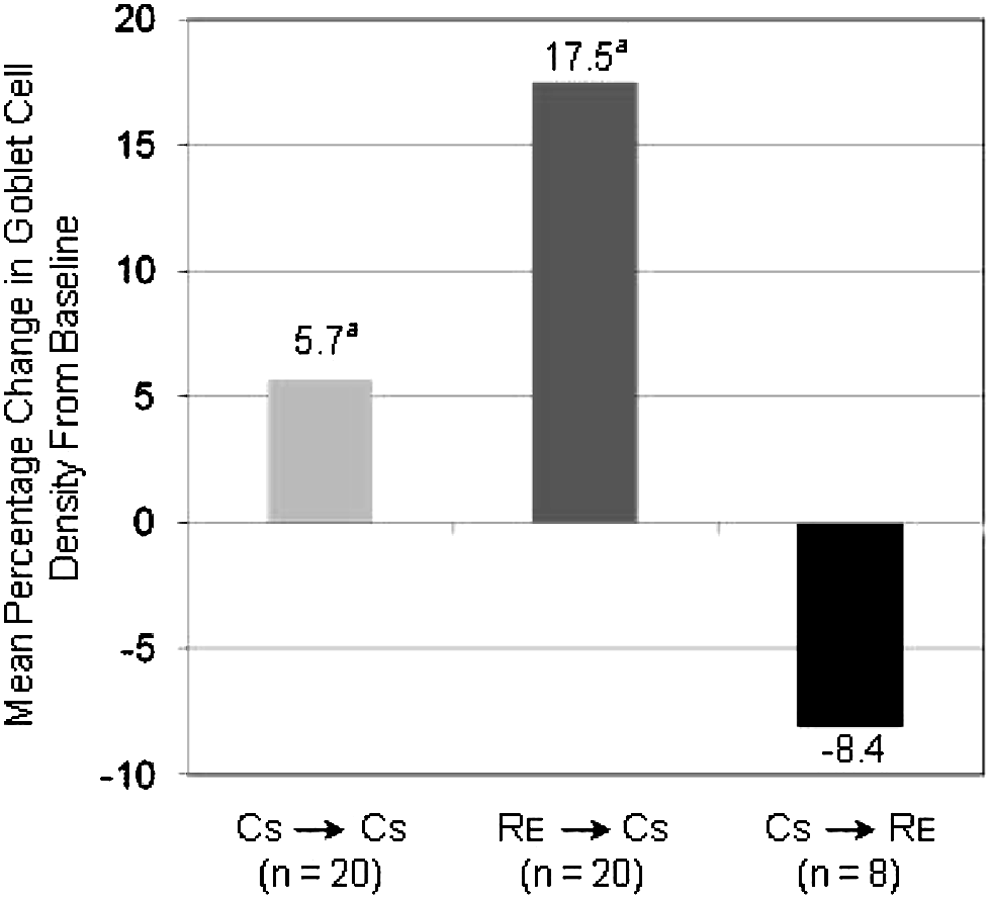
Changes in conjunctival goblet cell density at month 12 compared with baseline. Patients who had received cyclosporine 0.05% in the first year of study were randomized to receive either cyclosporine 0.05% (C
Adverse events
Discomfort on instillation was the only adverse event reported that was attributable to the study medications. There was no statistically significant between-group difference in the use of rescue artificial tears.
Discussion
Patients with dry eye disease suffer from ocular irritation often accompanied with vision impairment, which limits important daily activities and negatively impacts quality of life.16–18 The impact of dry eye in limiting daily activities and causing discomfort is known to increase as the disease progresses from mild to moderate in severity. 17 It is thought that initiating cyclosporine 0.05% therapy at the early stages of the disease may provide improved outcomes by interrupting inflammatory cycles. 19 Characterization of dry eye prognosis is, thus, the key to timely initiation and maintenance of appropriate therapies to ensure prevention of disease progression. The current study is the first to evaluate the impact of delayed cyclosporine 0.05% therapy as well as cyclosporine 0.05% withdrawal on the prognosis of patients with dry eye disease who were previously treated with artificial tears or cyclosporine 0.05%.
At baseline, patients with C
Throughout the study, patients with C
Artificial tears are the mainstay of treatment for dry eye. 20 However, artificial tears are not expected to affect the underlying cause of dry eye. It is not known whether the use of artificial tears has in any way affected disease prognosis, as there was not a vehicle arm in this study. Nevertheless, cyclosporine 0.05% withdrawal and initiation of artificial tear use increasingly aggravated dry eye signs and symptoms throughout the study. This finding highlights the necessity of maintenance therapy with cyclosporine 0.05% to preserve therapeutically gained benefits. The disease deterioration after the use of artificial tears also explains the underlying reason that the vast majority of patients seek new therapies after using several artificial tear products over years. 20
Cyclosporine is an immunomodulator agent.
21
In humans, topical cyclosporine 0.05% has been shown to decrease the number of activated T cells and the expression of inflammatory markers in the conjunctiva of patients with dry eyes.22,23 These findings indicate that cyclosporine 0.05% may target the underlying inflammatory processes in dry eye disease. It is noteworthy that the alleviation of dry eye signs in patients with C
The safety profile of a topical anti-inflammatory agent and its suitability for long-term use are the key factors in successful management of such chronic diseases as dry eye. In this study, the safety of BID cyclosporine 0.05% was monitored over the course of 2 years. Discomfort on instillation was the only adverse event reported that was attributable to cyclosporine 0.05%. Larger clinical studies have also reported that cyclosporine 0.05% was well tolerated for up to 3 years with most adverse events being transient in nature and mild to moderate in severity.24–26 These findings suggest that topical cyclosporine 0.05% is safe for long-term use against dry eye disease.
This study had a number of limitations. The sample size was small in the first year of study, as it was a pilot study to assess the feasibility of the study design; it became even smaller in the second year because of the addition of a new treatment arm and patient discontinuations. Further, the between-group differences reported in this study can be applied only to the use of Refresh Endura as the artificial tears. Other artificial tears may have variable efficacies in alleviating dry eye signs and symptoms.
Chronic use of anti-inflammatory therapies that normalize tear film composition early in the disease process are thought to potentially slow, prevent, or reverse dry eye progression. 18 The findings of the current study are the first evidence indicating that earlier treatment with cyclosporine 0.05% results in improved outcomes. Further, maintenance therapy with cyclosporine 0.05% appears to be necessary, as its clinical benefits continue over time, and dry eye worsens on its withdrawal. Large-scale, controlled studies are warranted to confirm these findings.
Footnotes
Acknowledgment
Hadi Moini, Ph.D., of Pacific Communications provided editorial assistance for this article.
Author Disclosure Statements
This study was supported by an unrestricted grant from Allergan, Inc., Irvine, CA. The author has no proprietary interest in any material or method mentioned in this study.