
Abstract
Abstract
Purpose:
The purpose of this study was to analyze the outcome of treating epidemic keratoconjunctivitis (EKC) with 2% povidone–iodine (PVP-I) solution.
Methods:
A prospective, interventional, uncontrolled study was performed in participants diagnosed with EKC. PVP-I was applied to the affected eyes 4 times a day for a week. Participants were informed about transient eye stinging and discoloration after application. Drug discontinuation was allowed for early recovery or encountering any adverse effects. Data collection included history, symptoms, and signs at the initial presentation and at 1 week. Main outcomes were the recovery rate within a week of treatment and drug tolerability.
Results:
Of 172 enrolled, 61 participants completed the study. EKC occurred bilaterally in 40 participants (66%). Single eye from each participant was included for analysis. The mean (standard deviation) time elapsed before treatment was 2.1 (1.46) days. The recovery rate within a week of treatment was 77% (95% confidence interval, 65.1–85.8). Twenty-eight participants (45.9%) recovered within a week after the onset. Application of PVP-I was sustained until recovery or completing a 7-day trial in 78.7%. No severe ocular or systemic adverse effects have been reported related to this treatment.
Conclusions:
Ocular application of 2% PVP-I was tolerable. This measure successfully relieved ocular discomfort from EKC in 3 quarters of the study group within a week. A randomized, controlled trial is required to verify the benefit of this measure.
Introduction
This disease is highly contagious and tends to present in epidemics. Patients can spread infection for as long as 10–14 days after the onset. Although EKC is self-limiting, it takes 1–3 weeks to resolve, given no serious corneal complications. Current treatment is mainly supportive. Patients suffering from this disease have to keep themselves away from others, averting them from living their normal lives. Further effective therapy to shorten its clinical course and inhibit disease spreading is required.
Povidone–iodine (PVP-I) is an antiseptic covering a broad spectrum of infective microorganisms. Ocular applications of PVP-I are widely adopted for prophylaxis of postoperative endophthalmitis and ophthalmia neonatorum. 1 It also has virucidal activities against multiple virus species including adenovirus. 2 This potential of PVP-I prompted the authors to perform a pilot trial to treat EKC. The present study reports the outcomes of using 2% PVP-I solution for treatment of EKC.
Methods
The study design was a prospective, interventional case series. Our institutional ethical committee approved the study protocol in April 2004. The authors performed the study between July 2004 and December 2009. During this period there were 2 episodes of epidemics of EKC. The first episode was in 2006 and the second in 2009. The study was conducted following the guidelines of the Helsinki Declaration and was registered in the Clinical Trials.gov with the identifier number NCT01179412.
Patients who were diagnosed with EKC at the outpatient ophthalmic unit were invited to participate in this study. The diagnostic criteria were based on its characteristic clinical presentations including acute onset of external eye inflammation producing eye irritation, photophobia, epiphora, blepharedema, conjunctival hyperemia, conjunctival chemosis, follicular reactions, and subconjunctival hemorrhage without any other explainable causes. All patients were informed on why and how the study was going to be conducted and the consent was signed prior to the study.
Exclusion criteria comprised children younger than 6 years, women being pregnant or during lactation, history of allergy to PVP-I, prior ocular surgery, contact lens usage, and chronic eye diseases with current eye medications.
Baseline data collected were age, gender, date of presentation, number of eyes involved and laterality, duration of the disease in each eye, prior ocular medications, condition of allergic conjunctivitis, flu-like symptoms before the onset, and history of close contact with EKC patients. Participants were asked to evaluate and subjectively grade the degree of their symptoms into no, mild, moderate, and severe. The symptoms evaluated included lid swelling, eye injection, irritation or foreign body sensation, tearing, sensitivity to light, and general feeling of discomfort in their eyes.
After visual acuity was recorded, eye examination was performed. The following ocular signs comprising blepharedema, conjunctival congestion, conjunctival chemosis, subconjunctival hemorrhage, follicular reactions, eye discharge, corneal involvement, anterior chamber reaction, and preauricular lymph node enlargement were assessed. Findings that were countable, such as the amount of follicles, corneal lesions, anterior chamber cells, and preauricular lymph nodes, were recorded in number. The severity of uncountable findings was assessed according to the following criteria: “normal” for no abnormality detected, “mild” for subtle abnormality detected with careful observation, “moderate” for obvious abnormality easily detected, and “severe” for overt abnormality producing deformity. The amount of subconjunctival hemorrhage was classified as “mild” for the involvement of less than 25% of total bulbar conjunctival area, “moderate” for between 25% and 50% of the area, and “severe” for more than 50% of the area.
The study drug was 2% solution of PVP-I. It was prepared in the Department of Pharmacology by diluting Betadine® (10% PVP-I; LFD Manufacturing Limited, Patumthani, Thailand, under license from Mundipharma B.V. Netherland) with sterile water for injection under sterile condition to become 2% solution. This solution was sterilized by pressurized filtration through a double-layered cellulose acetate filter of 0.2 μm pore size. Sterility was confirmed by incubation of the resulting solution on blood agar plates and thioglycollate medium. After passing these sterility tests, the solution was transferred and packaged in 5-mL eye drop containers. This process was performed inside the microbiological safety cabinet.
Each participant received 1 bottle of the study drug with the instruction to apply the solution onto his or her affected eyes 4 times a day for a week. They were allowed to discontinue the medication earlier if they found their diseases subsided or encountered any worsening systemic or ocular conditions. The participants were informed that this medication could produce a stinging sensation and brown coloration on the ocular surface. However, these would be spontaneously disappeared within a few minutes. The authors also recommended the hygienic measures on how to prevent the spreading of this contagious disease to others.
Participants were given appointments to return for eye examination a week later. Medication compliance, frequency of application, adverse effects, early discontinuation, and its cause were recorded. Participants were asked to evaluate their eye symptoms and assessment of ocular findings was performed in the same manner as at baseline.
The authors considered the absence of discomfort in the affected eyes as recovery. The main outcome measure was the proportion of participants recovering from EKC within a week. The second outcome of interest was drug tolerability, which was assessed by the proportion of participants sustaining application of the study drug until recovery or completing a 7-day trial.
For the study drug to be of benefit, it should provide a recovery rate of at least 80% within a week. Based on this hypothesis, 62 participants were required as suggested by nQuery Adviser program.
The authors used SPSS version 13.0 for statistical analysis. The collecting data were described in terms of mean, standard deviation (SD), range, median, or proportion as appropriate. Main outcomes were reported with 95% confidence interval (95% CI). We compared data between baseline and follow-up with Wilcoxon signed rank test. The time event of recovery and associated factors were assessed by Kaplan–Meier survival analysis. It was considered statistically significant when P value was lower than 0.05.
Results
During the study period, 172 participants were enrolled. Timing and number of participants are shown in Table 1. Only 61 participants (35.5%) completed the study. This group comprised of 25 males (41%) and 36 females (59%). Mean age (SD) was 41.7 (17.20) years, ranging from 10 to 84 years. Eight of them (13.1%) experienced flu-like symptoms shortly before developing EKC. Twenty-three persons (37.7%) contacted EKC from their close friends or relatives. There were 15 participants (24.6%) receiving other ocular medications, mostly antibiotic and astringent eye drops, prior to the enrollment. Two participants (3.3%) had a history of allergic conjunctivitis.
A total of 101 eyes of 61 participants suffered from EKC. This disease occurred unilaterally in 21 participants (34.4%) and bilaterally in 40 (65.6%). These included 46 (45.5%) right and 55 (54.5%) left eyes.
The authors initially performed a statistical analysis comparing all collected data between the right and left eyes of 40 participants presenting with EKC bilaterally. The analysis showed no significant difference between the 2 sides. We therefore selected data only from the right eye of the bilateral group and combined data with those from the unilateral cases for further analysis.
The mean duration (SD) of EKC before enrollment in the selected 61 eyes was 2.1 (1.46) days, ranging from 1 to 7 days. Ocular symptoms at initial presentation included lid swelling in 38 eyes (62.3%), red eye in 61 (100%), eye irritation in 60 (98.4%), excessive tearing in 57 (93.4%), sensitivity to light in 47 (77.1%), and general feeling of eye discomfort in 61 (100%). The median visual acuity was 20/20, ranging from 20/20 to 5/200. Eye examination revealed blepharedema in 37 eyes (60.6%), conjunctival chemosis in 33 (54.1%), conjunctival hyperemia in 55 (90.5%), subconjunctival hemorrhage in 22 (36.1%), watery secretion in 45 (73.8%), mucous secretion in 35 (57.3%), and purulent secretion in 2 (3.3%). Follicular reactions appeared in 55 eyes (90.2%), ranging from 4 to 40 follicles. The mean (SD) number of follicles was 13.1 (9.27). Corneal involvement including superficial punctate keratitis and subepithelial infiltration was found in 5 (8.2%) and 1 (1.6%) eye, respectively. Preauricular lymph node was palpable in 3 participants (4.9%), 1 node per participant.
One week after treatment, participants reported the symptoms of lid swelling in 1 eye (1.6%), red eye in 24 (39.3%), eye irritation in 16 (26.2%), tearing in 11 (18%), sensitivity to light in 8 (13.1%), and general feeling of discomfort in 14 (22.9%). The median visual acuity was 20/20, ranging from 20/20 to 20/200. Eye examination showed blepharedema in 2 eyes (3.3%), conjunctival chemosis in 2 (3.3%), conjunctival hyperemia in 21 (34.4%), subconjunctival hemorrhage in 6 (9.8%), watery secretion in 7 (11.5%), and mucous secretion in 2 (3.3%). Purulent secretion was not detected. Follicular reactions remained in 38 eyes (62.3%), varying from 1 to 30 follicles. The mean (SD) number of follicles was 5.4 (6.70). Superficial punctate keratitis and subepithelial infiltration were demonstrated in 7 (11.5%) and 2 (3.3%) eyes, respectively. Preauricular lymph node disappeared.
Comparisons of ocular symptoms and eye findings between baseline and follow-up on day 7 are shown in Table 2. There were significant improvement in most of the symptoms and signs. Follicular reactions were significantly reduced (P=0.000). Visual acuity was stable (P=0.152). Corneal involvement and preauricular lymph node showed no significant changes.
The severity of ocular symptoms was assessed by the participants. Eye findings were graded as “normal” for no abnormality detected, “mild” for subtle abnormality detected with careful observation, “moderate” for obvious abnormality easily detected, and “severe” for overt abnormality producing deformity.
Absence of general ocular discomfort was reported from 47 participants. Therefore, the recovery rate within 7 days of treatment was 77% (95% CI=65.1%–85.8%). Figure 1 shows cumulative proportion of participants successively recovering from EKC after beginning PVP-I application.
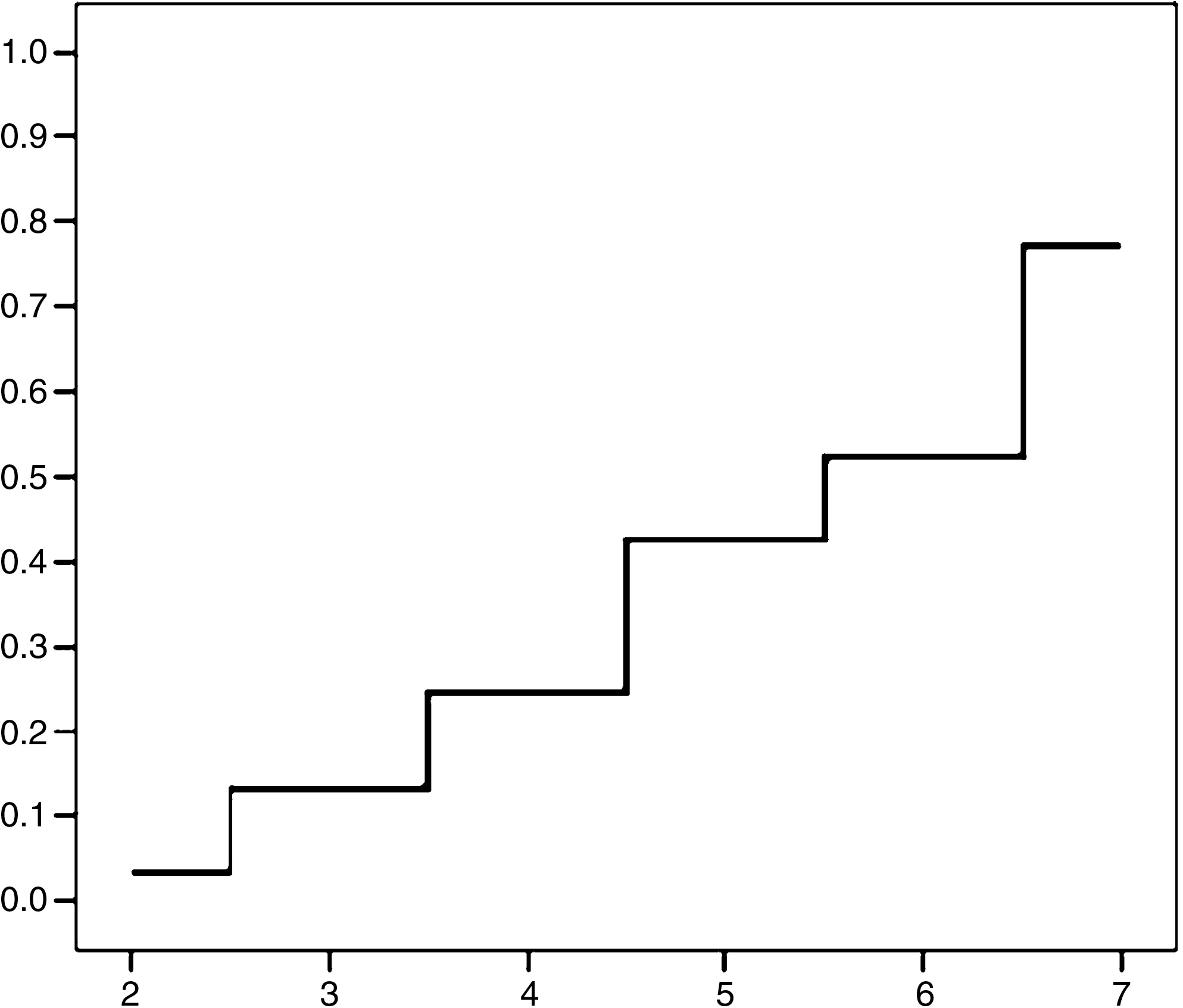
The cumulative proportion of participants recovering from epidemic keratoconjunctivitis after application of 2% povidone–iodine (days).
The duration from the onset until recovery in these 47 participants ranged from 4 to 14 days. There were 28 participants (45.9%) recovering within a week of onset. Figure 2 shows cumulative proportion of recovering participants since the onset.
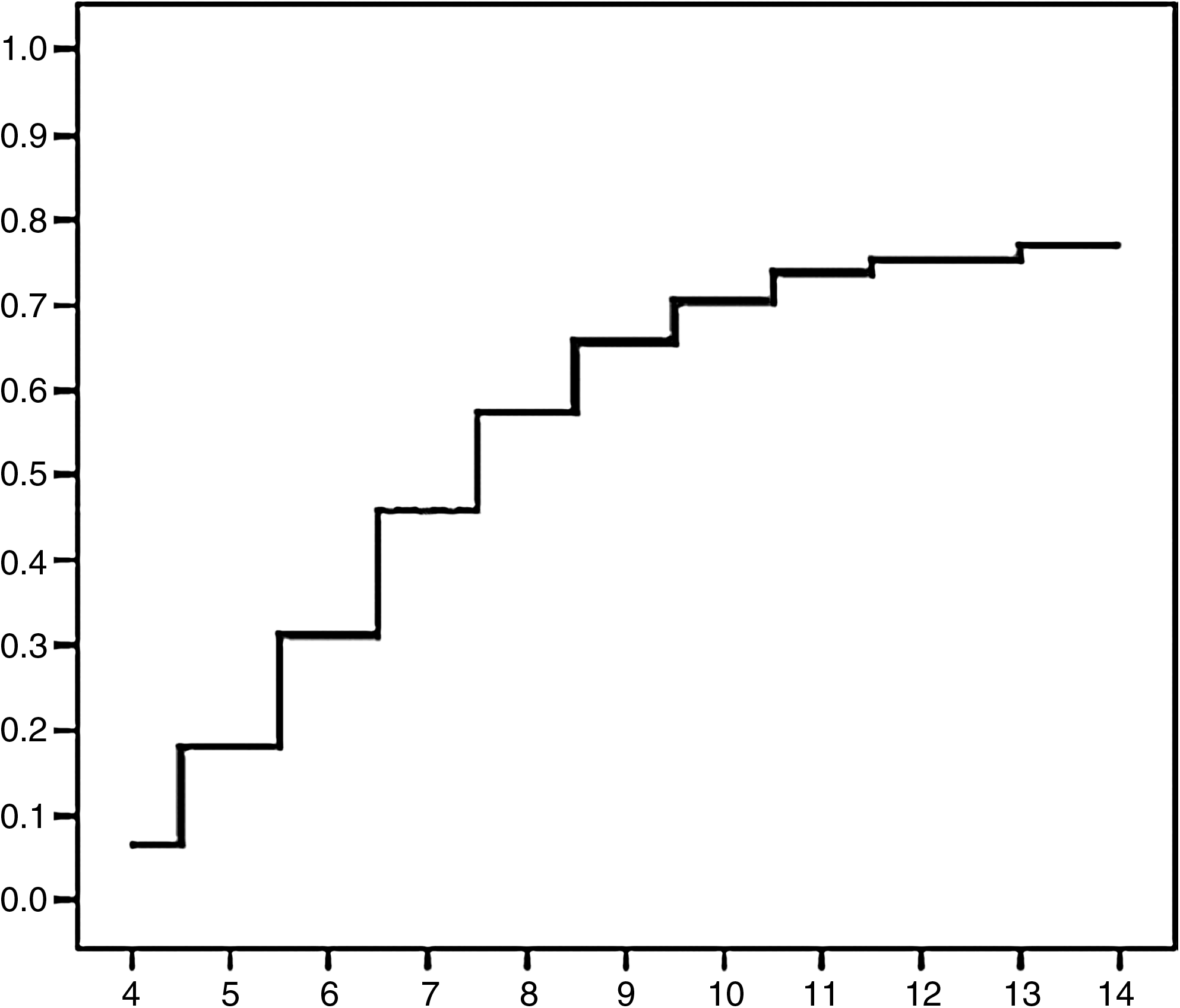
The cumulative proportion of participants, applying 2% povidone–iodine, recovering from epidemic keratoconjunctivitis since the onset (days).
The authors assessed baseline data to find any association with the recovery. Only a symptom of lid swelling was associated with the recovery within 7 days of treatment. Moderate to severe lid swelling brought less chance to recover compared with the milder symptom as shown in Fig. 3 (P=0.015, log-rank test).
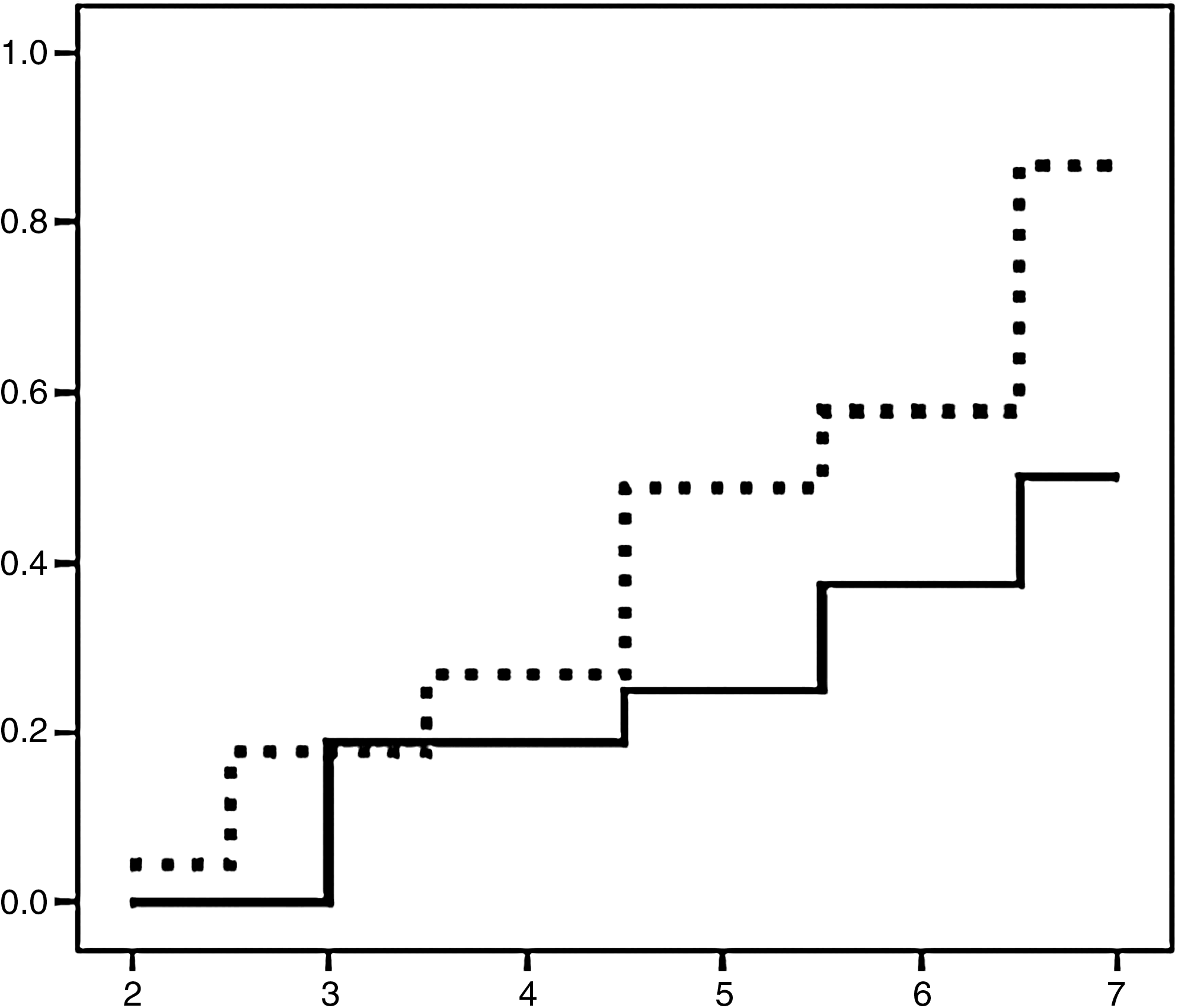
Comparison of cumulative proportions of participants recovering from epidemic keratoconjunctivitis after application of 2% povidone–iodine (days) between an initial symptom of moderate to severe lid swelling (solid line) and the milder group (dashed line) (P=0.015, log-rank test).
Application of 2% PVP-I solution was sustained in 48 participants, giving tolerability rate of 78.7% (95% CI=66.9%–87.1%). Thirteen participants terminated the application of PVP-I sooner than a week and before recovery because of a stinging sensation. However, no ocular or systemic adverse effects occurred in any participants.
Discussion
Epidemic karatoconjunctivitis is a very infectious eye disease caused by adenovirus. The common serotypes associated with EKC are adenovirus 8, 19, and 37. Asian countries are endemic areas of these viruses. Community outbreaks occur in this region every 2–3 years. It usually presents in rainy season between June and December. However, sporadic cases can be found throughout the year.
Although this disease is self-limiting, the suffering due to ocular distressing symptoms extends to at least 1–3 weeks before it subsides. In case of serious corneal involvement, visual acuity can be disturbed for a long period. Besides, the highly contagious nature of the disease brings social and economic burdens. Several studies of multiple agents have been tried to shorten the disease process and prevent spreading. These agents include antiviral, anti-inflammatory, and antiseptic drugs.
Among the antiviral drugs, ocular application of 3.3% vidarabine ointment was studied in patients with positive adenoviral culture. It was ineffective to prevent development of corneal infiltration. 3 Another study from Philippines also showed no benefit of treatment with trifluridine over the artificial tears. 4 As adenoviruses encode their own replicating enzymes that were different from herpes viruses, they are therefore more resistant to these drugs. 5
Treatment with topical 1% cidofovir yielded a significantly lower prevalence of severe corneal opacities, but a longer duration of punctate epithelial keratitis. This agent produced conjunctivitis and erythematous inflammation of the eyelids. These local toxicities forced a premature termination of the study. 6
Topical human fibroblast interferon was also tested, but the result was inconclusive. High concentration of interferon over 750,000 IU/mL was suggested for treatment of severe cases. 7
N-Chlorotaurine, an endogenous antimicrobial agent, in 1% solution was compared with gentamicin in the treatment of adenoviral conjunctivitis. It is a weak oxidant produced by human granulocytes in response to inflammation. This substance inactivates the pathogens by oxidation of protein. The subjective and objective scores on day 4 and the subjective score on day 8 were lower in the study group. However, the occurrence of subepithelial infiltrates was similar in both groups. 8
Therapy with topical corticosteroids did not prevent subsequent corneal involvement but prolonged disease duration. Study in animal models demonstrated enhancing effect of corticosteroids on viral replication. 9 Corticosteroids should be exclusively reserved for severe cases producing conjunctival membrane or pseudomembrane and debilitating corneal infiltrations. Nonsteroidal anti-inflammatory drugs such as ketorolac and diclofenac had no effect on viral shedding and the formation of corneal infiltrates. 10
Multiple antiseptics were tested in vitro for the ability to inactivate adenoviruses. These included PVP-I, alkyldiaminoethylglycine hydrochloride, chlorhexidine gluconate, benzalkonium chloride, and benzethonium chloride. Among these substances, only PVP-I in concentrations higher than 0.5% can inactivate the viruses within 1 min of exposure. 2 A prospective study in Germany reported a better result in treating EKC with PVP-I alone over the combination of PVP-I with interferon alpha or trifluridine. 11 The use of PVP-I in EKC has been reported in 2 manners: either by swabbing the eyelids with 10% solution in an eye clinic or prescribing a 5% preparation for eye dropping. 12
A solution of 1.25% PVP-I was studied in a controlled trial to treat various kinds of conjunctivitis in children. It was compared with a combination of antibiotics consisting of neomycin, polymyxin-B, and gramicidine. Viral conjunctivitis was diagnosed in participants presenting with follicular reaction, conjunctival membrane, or corneal infiltrates and negative bacterial culture. The results were comparable between PVP-I and the antibiotic combination. Hence, the solution of 1.25% PVP-I was considered ineffective against viral conjunctivitis. However, this trial was not specifically performed in EKC patients. 13
From a previous report on 1.25% PVP-I, the authors decided to use 2% concentration of PVP-I to treat EKC in the present study. Most of the distressing symptoms and signs of EKC were significantly improved from baseline. After a week of treatment, 77% of the participants considered themselves recovering from EKC. The only factor predicting successful recovery within a week was a mild symptom of lid swelling at presentation. This might reflect less-severe cases. The authors tested correlations between the severity of symptoms described by participants and the results of corresponding eye examination and observed well-parallel outcomes. However, the grading of blepharedema did not associate with the recovery.
A solution of 2% PVP-I could not completely prevent corneal involvement. Superficial punctate keratitis and subepithelial infiltrations were documented in 7 and 2 eyes after 1 week of treatment, comparing to 5 and 1 eye at baseline, respectively. Neither did this agent prevent the fellow eye involvement. Two of 21 participants presenting with unilateral disease developed EKC in the fellow eye. Inoculation of viruses in these fellow eyes might have happened before the application of PVP-I in the affected eyes.
The common ocular adverse effect from 2% PVP-I was eye stinging. This prevents patients from comfortable use of this agent. The authors' previous experience in using 5% PVP-I for prophylaxis of postoperative endophthalmitis found 6.6% of moderate to severe eye irritation without adverse long-term consequences. 14 To reduce the irritating effect, application of PVP-I by eye irrigation and lid swabbing in an eye clinic after topical anesthesia can be an alternative method to treat EKC. Otherwise, a new formulation of PVP-I with less irritating effect is required to solve this problem.
A lower concentration of PVP-I solution was also tested in a limited number of patients. A combination of 0.4% PVP-I and 0.1% dexamethasone ophthalmic solution was preliminarily studied to treat adenoviral conjunctivitis in 9 eyes of 6 patients. Clinical resolution and reduction of viral titer were observed within 5 days of treatment. 15
The present study was designed as a pilot study to observe the possibility of using the study drug in clinical practice and collect data to consider for further clinical trial. No controlled group was prepared.
Although microbiological confirmation is not compulsory for EKC diagnosis, the authors understand that identification of causative pathogens via antigen detection, viral isolation, or polymerase chain reaction would strengthen the diagnosis. The authors are aware of the limitation of diagnosis that it is based solely on clinical presentations. However, most of our participants were enrolled during EKC epidemics in a community and all had characteristic clinical features of the condition. Identification of causative organisms could provide additional information on how individual case may respond to PVP-I treatment. This would be our further study with increasing number of participants.
The authors considered evaluation of general discomfort as a suitable outcome in the present study. All participants reported a general feeling of discomfort at baseline. Although this is a subjective measure, determination of outcome by the participants would help prevent investigator bias.
An episodic presentation of EKC and a high rate of loss to follow-up prolonged the study period. Losses to follow-up commonly occur in managements of low virulent diseases with short running course. The dropout rate was high among patients of studying and working age groups. These were the majority of the participants in the present study.
All of these issues should be considered as limitations in interpreting the study results. Future studies should be prepared to handle these problems.
In conclusion, application of 2% PVP-I onto the eye was tolerable. Recovery rate from EKC after a week of application in the complete study group was 77%. This agent could not completely prevent corneal involvement or totally exclude the fellow eye from infection. A randomized, controlled trial to verify the benefit of this measure is required.
Footnotes
Acknowledgments
The authors thank Mr. Chaipon Manochnon and Ms. Piyapat Pongnarin for their help in the preparation of the study drug. Drs. Siriwon Chinwattanakul, Saowanee Kieatkulchai, and Mathinee Chongchareon were assistants in collecting data. Mr. Suthipol Udompunthurak was the consultant in statistical analysis. Ms. Mathuwan Srikong prepared figures for publication.
Author Disclosure Statement
There is no conflict of interest with any financial organization regarding the material discussed in this article.