
Abstract
Abstract
Purpose:
Malignant hypertensive retinopathy is a rare, but serious, complication of uncontrolled systemic hypertension for which no treatment has been established yet. We report 2 patients with malignant hypertensive retinopathy who recovered promptly following intravitreal bevacizumab injection.
Methods:
Intravitreal bevacizumab (1.25 mg/0.05 mL) was injected in 4 eyes of 2 patients having malignant hypertensive retinopathy with optic disc edema, macular edema, and retinal exudates. A complete ophthalmic examination, including the best-corrected visual acuity (BCVA), central macular thickness (CMT) on optical coherence tomography (OCT), and fluorescein angiography (FAG), was performed before and after the treatments.
Results:
Two eyes in 1 patient received two intravitreal injections of bevacizumab, whereas 2 eyes in the other patient received a single treatment. All 4 eyes had improvement of macular edema on OCT at 1 month and decreased fluorescein leakage on FAG 3 months after the treatment, which led to improvements in the BCVA in 3 eyes. In 1 eye with foveal atrophy, no change in the BCVA occurred despite the improved macular edema on OCT.
Conclusions:
The results suggest that intravitreal bevacizumab injections might be a useful adjunctive treatment of malignant hypertensive retinopathy in some selected cases. However, further studies are mandatory to determine the safety and the efficacy of such injections in this disease.
Introduction
The treatment of hypertensive retinopathy includes urgent antihypertensive management; however, no randomized controlled studies have evaluated whether treating the hypertension will reverse established hypertensive retinopathy changes.2,8 Bevacizumab (Avastin®), an antibody against vascular endothelial growth factor (anti-VEGF), has been injected intravitreally in several retinal diseases that have increased vascular permeability and edema.10,11 This study reports 2 patients with malignant hypertensive retinopathy who showed severe exudative retinal changes and visual impairment, but recovered promptly following intravitreal bevacizumab injection.
Case Reports
Case 1
In May, 2009, a 28-year-old woman was referred because of blurred vision in both eyes for 2 days. She had been taking medication to treat hypertension for 3 years with poor control of blood pressure and had been on peritoneal dialysis because of end-stage renal disease due to chronic glomerulonephritis for 1 year. Her best corrected visual acuity (BCVA) was 20/63 (Snellen) and 20/400 (Snellen) in her right and left eyes, respectively. Fundoscopic examination revealed bilateral optic disc swelling, peripapillary retinal edema involving the macula, and peripapillary flame-shaped hemorrhages with multiple hard exudates (Fig.1A,B). The anterior segment examination of both eyes was unremarkable. Fluorescein angiography (FAG) showed extensive fluorescein leakage from the optic disc and diffuse capillary leakage along the vascular arcades in both eyes (Fig. 2A,B). Optical coherence tomography (OCT) revealed bilateral macular edema and subfoveal neurosensory detachment (Fig. 3A,B). Her blood pressure was 150/90 mmHg and, due to a diagnosis of malignant hypertensive retinopathy, cardiology, nephrology, and neurology, consultations were obtained. She was lost to follow-up until March, 2011, and referred from the Nephrology Department because of decreased vision in both eyes for 2 weeks. Visual acuity measured 20/100 in the right eye and 20/50 in the left eye. The fundoscopic examination showed star-shaped exudates on the macula and optic disc edema in both eyes (Fig. 1C,D). Bilateral diffuse capillary leakage from dilated vessels and the optic disc were noted on FAG (Fig. 2C,D). Bilateral macular edema and intraretinal exudates were confirmed by OCT (Fig. 3C,D).
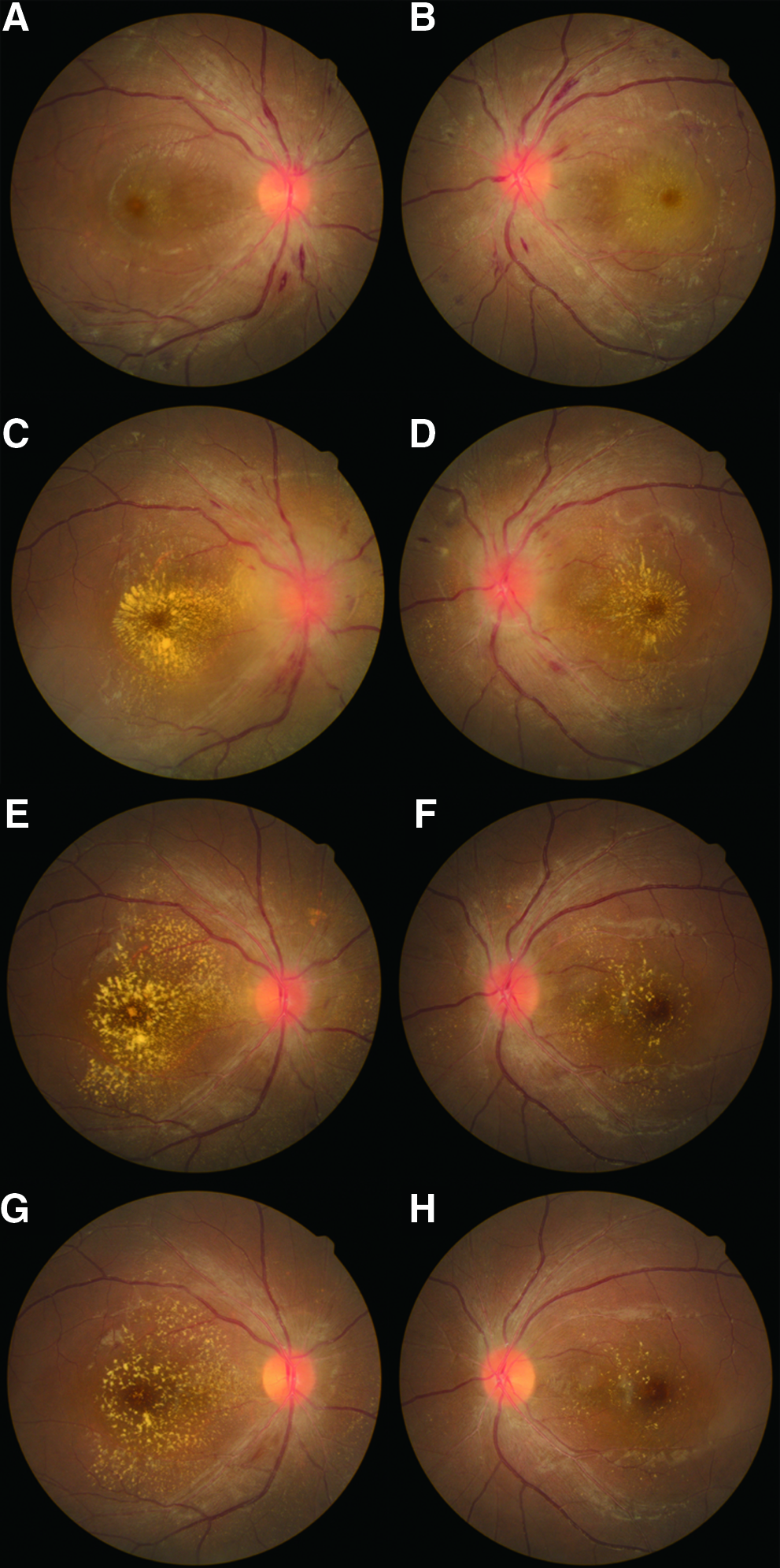
Fundus findings in case 1 before and after intravitreal bevacizumab injection. At presentation, optic disc swelling, macular edema, and peripapillary flame–shaped hemorrhages were present in both eyes (
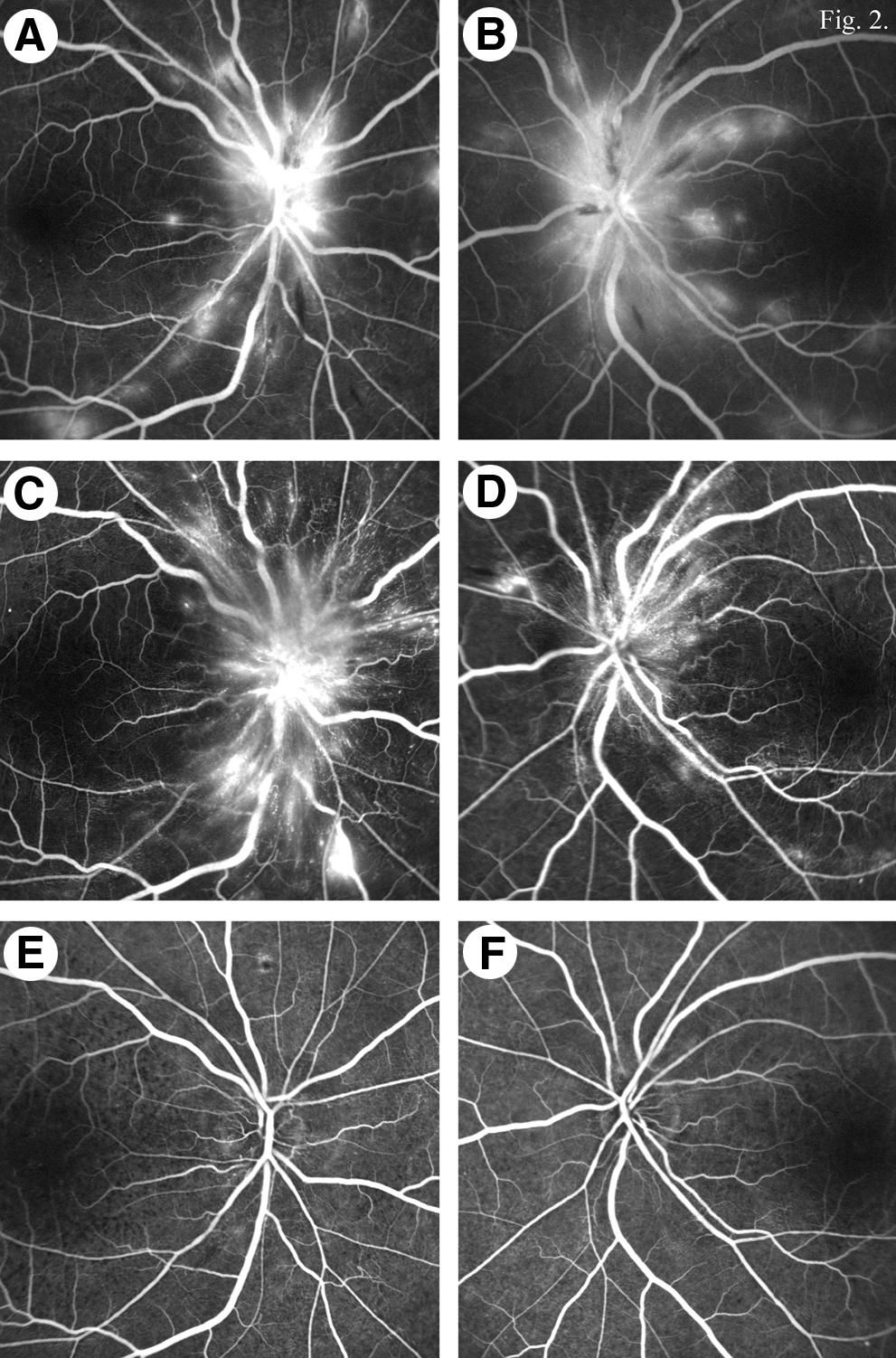
Fluorescein angiography (FAG) findings in case 1 before and after intravitreal bevacizumab injection. At presentation, profuse fluorescein leakage from the optic disc and diffuse leakage from the capillaries along the vascular arcades were present in both eyes (
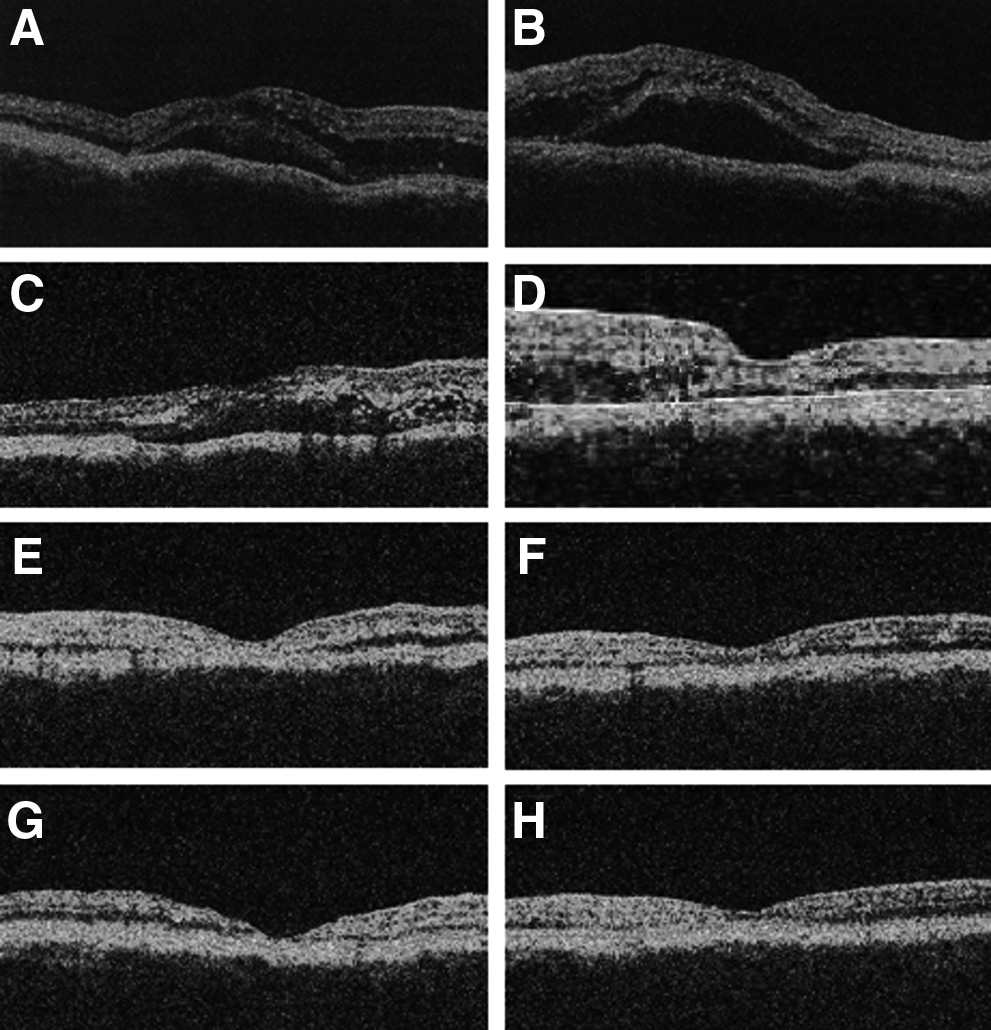
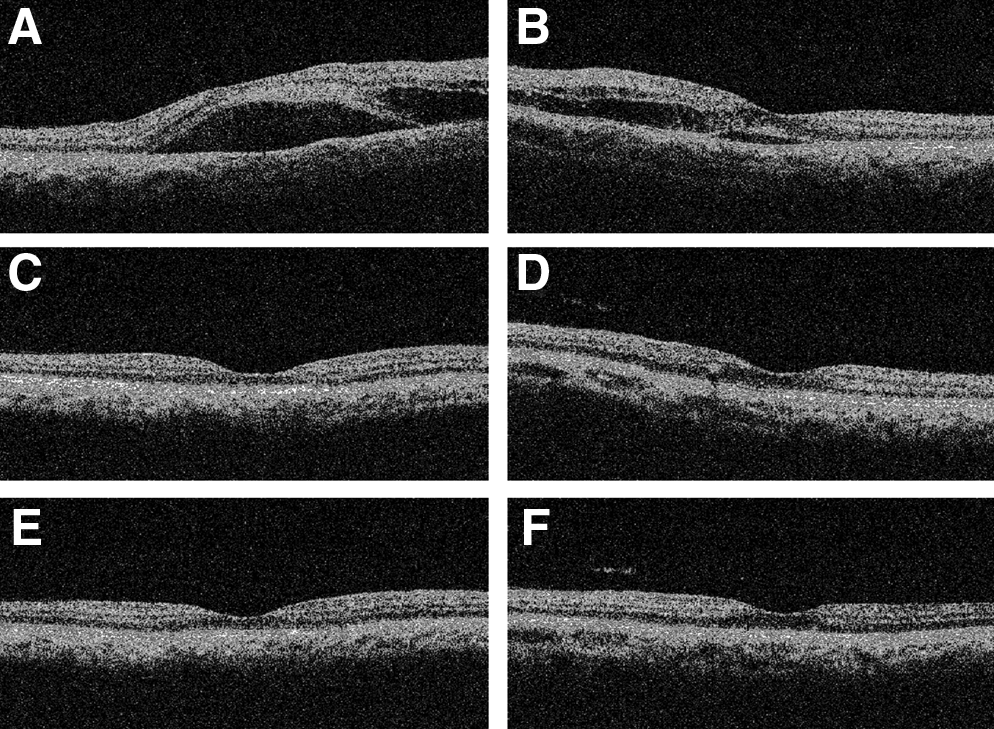
Optical coherence tomography (OCT) findings in case 1 before and after intravitreal bevacizumab injection. At presentation, bilateral macular edema and subfoveal neurosensory detachment were noted. The central macular thickness (CMT) was 473 μm in the right eye (
This patient was treated with 2 intravitreal injections of bevacizumab (1.25 mg/0.05 mL) in both eyes 1 month apart. One month after the treatment, visual acuity was 20/100 and 20/32 in her right and left eyes, respectively, and the bilateral optic disc edema and macular edema had resolved (Fig. 1E,F). Three months after the treatment, much of the hard exudates surrounding the fovea bilaterally were absorbed on fundus examination (Fig. 1G,H), and FAG showed minimal leakage from the optic discs bilaterally (Fig. 2E,F). Although she showed resolution of the bilateral macular edema, atrophic thinning of the fovea in both eyes was detected on OCT at 1 and 3 months after the therapy (Fig. 3E–H). Her visual acuity improved to 20/25 in the left eye, but remained 20/100 in the right eye because of the foveal atrophy 3 months after the therapy.
Case 2
A 35-year-old woman complained of decreased vision in her right eye for 3 days in November, 2009. She had a history of gestational hypertension 8 years earlier, but she had no further evaluation after the delivery. Upon presentation, BCVA was 20/100 and 20/25 in her right and left eyes, respectively. The anterior segment findings were normal, and the fundoscopic examination revealed bilateral optic disc swelling, tortuous retinal vessels, macular edema, and cotton wool spots (Fig. 4A,B). FAG showed diffuse fluorescein leakage from the optic disc and retinal capillaries in both eyes (Fig. 5A,B), and OCT revealed bilateral macular edema and subfoveal neurosensory detachment (Fig. 6A,B). Her blood pressure was 250/170 mmHg.

The fundus findings in case 2 before and after intravitreal bevacizumab injection. Before the treatment, bilateral disc edema, macular edema, and narrowed retinal vessels were noted (
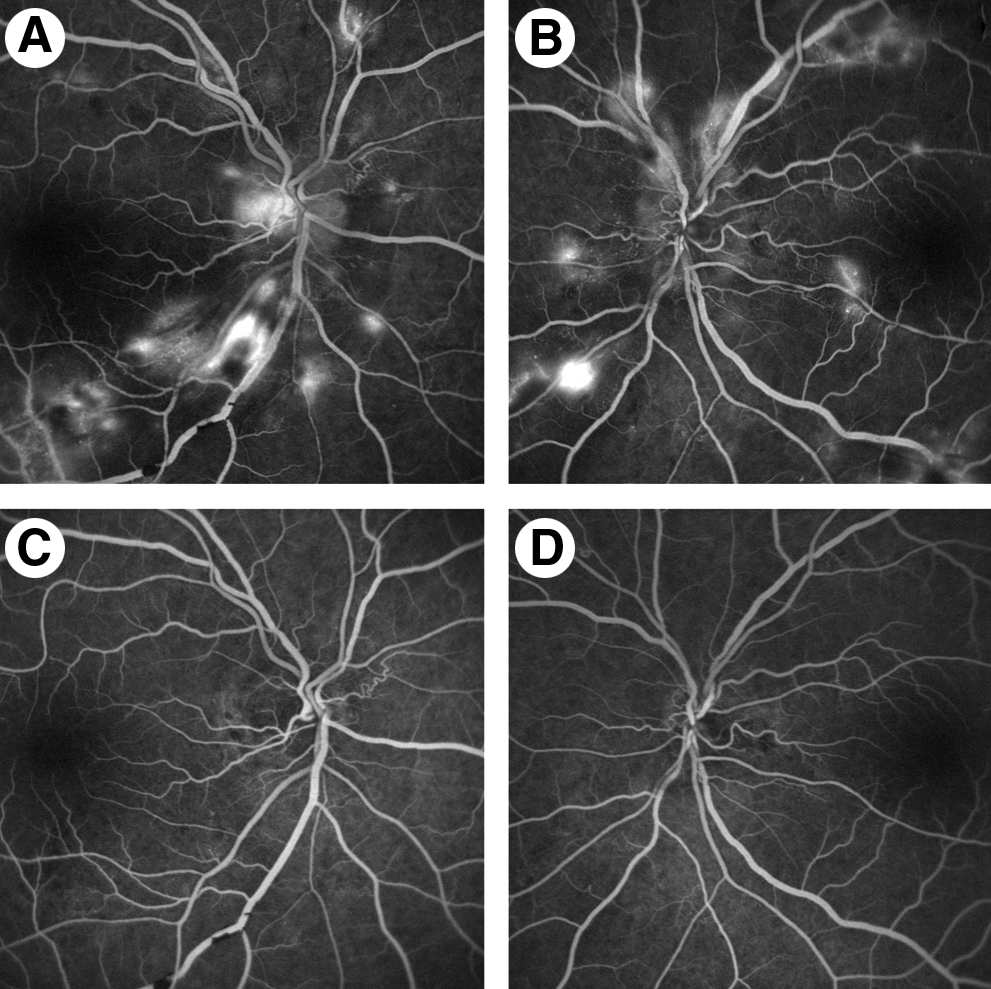
Fluorescein angiography (FAG) findings in case 2 before and after intravitreal bevacizumab injection. Before the treatment, diffuse leakage from the optic disc and retinal capillaries on FAG were observed (
The optical coherence tomography (OCT) findings in case 2 before and after intravitreal bevacizumab injection. Before the treatment, OCT revealed bilateral macular edema and neurosensory detachments with a central macular thickness (CMT) of 539 μm in the right (A) and 331μm in the left (
After the diagnosis of malignant hypertensive retinopathy, cardiology and neurology consultations were obtained and intravitreal bevacizumab (1.25 mg/0.05 mL) was injected in both eyes. One month after the injection, visual acuity improved to 20/25 in the right eye and 20/20 in the left eye, with resolution of the bilateral macular edema on OCT (Fig. 6C,D). The bilateral optic disc edema and macular edema had disappeared with minimal hard exudates in the right eye on fundus examination and OCT 3 months after the treatment (Fig. 4C,D, 6E,F). No fluorescein leakage was detected on FAG in both eyes (Fig. 5C,D), and the visual acuity was 20/20 in both eyes. The retinal findings, visual acuity, FAG findings, and OCT results remained stable for an additional 3 months of follow-up (Fig. 4E,F).
Discussion
Malignant hypertensive retinopathy is the most severe stage of hypertensive retinopathy in which swelling of the optic disc, macular edema, microaneuryms, hard exudates, and cotton wool spots appear.7,12 These changes in the retina usually indicate severely elevated blood pressure. The clinical course and prognosis of malignant hypertensive retinopathy varies considerably according to the duration of symptoms, visual acuity at presentation, degree of blood pressure elevation, and coexisting retinal vascular complications due to hypertension.13,14 According to Chen et al., 13 11 of 14 patients with malignant hypertensive retinopathy had a favorable visual prognosis when the blood pressure was controlled, whereas 3 patients, who had longer durations of high blood pressure and other retinal co-morbidities, such as central artery occlusion and anterior ischemic optic neuropathy, still had blurred vision. Although some experimental studies 15 and clinical case reports 16 have shown that the signs of hypertensive retinopathy regress with blood pressure control, no randomized controlled studies have evaluated whether blood pressure control will reverse established hypertensive retinopathy changes. Also, whether antihypertensive medications that are thought to have direct beneficial effects on the microvascular structure (e.g., angiotensin-converting enzyme inhibitors) reduce the damage of retinopathy beyond the reduction caused by the lowered blood pressure remained unclear. 2
The use of intravitreal anti-VEGF therapy has expanded tremendously in recent years, and intravitreal anti-VEGF agents are now used to manage complications of various diseases of the posterior segment.10,11 In the exudative stage of hypertensive retinopathy, disruption of the inner blood–retina barrier, necrosis of the smooth muscles and endothelial cells, and exudation of blood and lipids appear.7,17 Therefore, targeting VEGF as a potent permeability factor might be useful in the management of macular edema and optic disc edema in eyes with malignant hypertensive retinopathy. The intravitreal injection of anti-VEGF agents can theoretically accelerate up the resolution of macular edema with exudative retinal detachment and improve the visual outcome.
In our cases, intravitreal bevacizumab injection in patients with malignant hypertensive retinopathy resulted in prompt resolution of the macular edema and optic disc edema. This result suggests that intravitreal bevacizumab injection might be an effective therapeutic modality for treating exudative hypertensive retinopathy, in addition to lowering blood pressure. Nevertheless, our study is limited by the small number of patients and lack of a control group. Furthermore, individuals with malignant hypertensive retinopathy may experience spontaneous resolution of the retinopathy with the control of blood pressure; our cases do not allow one to determine if the resolution of the macular edema and optic disc leaks actually resulted from the injection or was due to the blood pressure control. However, in patient 1, who had persistent bilateral malignant hypertensive retinopathy despite blood pressure control, the macular edema and optic disc leakage promptly resolved following intravitreal bevacizumab injection, suggesting the effectiveness of the treatment. Further investigations are required to evaluate the safety and efficacy of this new therapy and the possible role of VEGF in the pathogenesis of hypertensive retinopathy.
Footnotes
Author Disclosure Statement
The author has no competing financial interests.