
Abstract
Abstract
Purpose:
The aim of this study was to assess the intraoperative application of mitomycin C (MMC) compared to 5-fluorouracil (5-FU) on the outcome of trabeculectomy and to examine the balance of risk and benefit.
Methods:
Pertinent studies were selected through systematic searches of major literature databases, including the Cochrane Library, PubMed, Embase, and Chinese Biomedicine Database. Internet searches of search engines, the professional associations' websites, and the manufacturers' databases were also performed. Clinical controlled trials comparing 5-FU with MMC in trabeculectomy were selected. The primary efficacy measure was the weighted mean difference (WMD) in percentage intraocular pressure reduction (IOPR%) at follow-up end point. The secondary efficacy measure was the relative risk (RR) for “qualified” (with or without medical therapy) success of trabeculectomy at follow-up end point. The third efficacy measure was RR for “complete” (without medical therapy) success of trabeculectomy at follow-up end point. The fourth efficacy measure was RR for adverse events, including wound leak, hypotony, endophalmitis, and shallow anterior chamber (AC). The pooled effects were calculated using the random effects model by RevMan version 5.0 software.
Results:
Eight studies enrolling a total of 536 patients were included in the meta-analysis. MMC was associated with significantly more IOPR% compared with 5-FU, with a WMD of 7.09 [95% confidence interval (CI) 1.47–12.70] at follow-up end point (P=0.01). MMC was comparable with 5-FU in qualified success rate, with a RR of 1.09 (0.99–1.20) at follow-up end point (P=0.09). MMC was comparable with 5-FU in complete success rate, with a RR of 1.17 (0.79– 1.75) at follow-up end point (P=0.43). Rates of adverse events did not differ significantly between 5-FU and MMC, with an RR of 0.71 (0.22–2.28) for bleb leakage, 1.40 (0.72–2.72) for hypotony, 1.63 (0.27–9.75) for endophthalmitis, and 0.95 (0.41–2.21) for shallow AC.
Conclusions:
Intraoperative MMC is more effective in lowering IOP in trabeculectomy compared with intraoperative 5-FU, but is comparable with intraoperative 5-FU in both qualified and complete success rate. Intraoperative use of both agents may contribute equally to adverse events.
Introduction
MMC has been reported in randomized controlled trials4–12 (RCTs) to reduce mean IOP at 12 months. Postoperative 5-FU implications have been assessed with RCTs.13–16 A systematic review has proved that MMC reduces mean IOP at 12 months 17 and RCTs for 5-FU have proved IOP reduction at 1 year compared to placebo. 18 Khaw suggested that a single intraoperative application of 5-FU might be sufficient to control postoperative proliferation of scar tissue at the drainage site. 19 Clinicians now appear to prefer the intraoperative application of agents for the modification of wound healing, and routine postoperative injections of 5-FU are rarely used. Therefore, we focused on intraoperative rather than perioperative use of 5-FU in this review.
The results of two reviews comparing MMC and 5-FU to placebo have suggested a similar effect for the two agents in inhibiting scarring after trabeculectomy.17,18 Some clinicians consider MMC more powerful and some prefer 5-FU. A previous review suggested that MMC results in a greater decrease in IOP than 5-FU. 20 However, a recent meta-analysis found no statistically significant difference between the intraoperative application of these two antifibrosis agents. 21 Clinically, these two agents seem to have different results. Therefore, to evaluate the efficacy and safety of these two antifibrosis agents, we undertook a systematic review and meta-analysis focusing on intraoperative MMC and intraoperative 5-FU use in all relevant controlled clinical trials.
Materials and Methods
This meta-analysis was performed according to a predetermined protocol described in the following paragraph, and standard systematic review techniques, as outlined by the Cochrane Reviewers' Handbook, were followed at all stages of the process. 22
Outcome measures
The primary outcome was the percentage reduction from preoperative to postoperative in IOP (IOPR%). When authors reported mean and standard deviation (SD) of IOP and IOPR, we used them directly. When not available, we computed them according to the methods described in the Cochrane Handbook for Systematic Reviews of Interventions: IOPR=IOPbaseline−IOPend point and SDIOPR=(SD2baseline+SD2end point –SDbaseline×SDend point)1/2. IOPR%=IOPR/IOPbaseline and SDIOPR%=SDIOPR/IOPbaseline.
When the difference in means (MD) and its t-value [t-value also can be obtained from a computer by entering=tinv (P value, Ntreat+Ncontrol−2) into any cell in a Microsoft Excel spreadsheet] were reported, SD=MD−t−1×(N−1treat+N−1control)−1/2.
For efficacy, the proportion of qualified success and complete success was also used. Qualified success was defined as target end point IOP with or without medications. Compete success was defined as target end point IOP without medications. The fourth outcomes were adverse event rates in either group, including wound leaks, hypotony, late endophthalmitis, and shallow anterior chamber.
Search strategy
Clinical trials comparing intraoperative MMC use with intraoperative 5-FU use were identified through a systematic search of the Cochrane Library, PubMed, and EMbase. A broad search strategy combined terms related to MMC (including MeSH search using mitomycins and keyword search using words mmc, mutamycin, m?tom?cin, mitoc?n and amet?cin?), terms related to 5-FU (including MeSH search using fluorouracil and keyword search using words fluorouracil, fluracilium, fluracil, fluoruracil and flu), and terms related to surgery (including MeSH search using exp Filtering-Surgery and Glaucoma-Surgery, and keyword search using words trabeculectom, sclerostom, filter near surg, filtrat near surg and glaucoma near surg), with a filter to restrict results to clinical trial, meta-analysis and randomized controlled trial. The original search was performed in January, 2011. Regular alerts every 3 months were established on PubMed and Embase databases to capture new studies until June, 2011, and updated searches on the Cochrane databases regularly.
The internet was searched using the Google and Yahoo! search engines and using the terms 5-fluorouracil and mitomycin C. A manual search was performed by checking the reference lists of original reports and review articles, retrieved through the electronic searches, to identify studies not yet included in the computerized databases.
Trials selection
Published and unpublished trials fulfilling the following selection criteria were included in the present meta-analysis: (1) Study design—controlled clinical studies, including cohort studies or randomized trials; (2) population—patients with glaucoma, including primary and secondary, who were undergone trabeculectomy or phacotrabeculectomy; (3) intervention—intraoperative MMC was administered at any concentration and dose, and was compared with intraoperative 5-FU of any concentration and dose; (4) outcome variables—at least one of the following outcome variables, IOPR%, complete success rate, and qualified success rates. Studies involving other types of glaucoma surgery, such as nonpenetrating glaucoma surgery, were excluded. Other exclusion criteria included repeated glaucoma surgery.
After completion of the searches, two review authors (Z.J.L., Y.L.) working independently assessed the titles and abstracts of all obtained reports for a rough judgment of an article's eligibility. The full-text copies of possibly and definitely relevant trials were obtained and assessed by the two authors independently according to the definitions in the criteria, which were checked by J.W.C. Only trials meeting these criteria were assessed for methodological quality. For the publications reporting on the same study population, the article reporting the results of the last end point was included, and data that could not be obtained from this publication were obtained from others.
The observers were blinded to the names of the authors and their institutions, the names of the journals, sources of funding, and acknowledgments, as well as the financer of the study.
Data extraction
Data extraction was performed by two reviewers (Z.J.L., Y.L.) independently. Any disagreement was resolved by discussion. For each study and each type of treatment, the following data were extracted: The authors of the study, the year of publication, information on study design, location of trial, length of study, number of subjects, patient age, sex, and IOP measurements. Numeric discrepancies between the two independent data extractions were resolved after discussion.
Qualitative assessment
The qualities of clinical trials included were assessed by two independent observers (Z.J.L. and Y.L.) using a previously reported quality assessment system that was for both randomized and nonrandomized studies. 23 The system contained 27 items distributed between five subscales about reporting (10 items), external validity (3 items), bias (7 items), confounding (6 items), and power (1 item). Any discrepancy in the qualitative assessment between the two observers was discussed and a consensus was reached. The total score of each trial was expressed as a percentage of the maximum achievable score. Good quality refers to a quality score not lower than 50%.
Statistical analysis
Not all of the trials reported on all the outcomes of interest. For each comparison and outcome, we undertook separate meta-analyses. Outcome measure was assessed on an intent-to-treat (ITT) basis. Considering the different clinical characteristics among study groups and the variation of sample sizes, we assumed that heterogeneity was present, even when no statistical significance was identified, and we decided to combine data by using a random-effects model to achieve more conservative estimates.
For dichotomous outcomes, relative risk (RR) was estimated. Weighted mean difference (WMD) was calculated for continuous outcomes. Analyses were carried out in RevMan version 5.0 software (Cochrane Collaboration, Oxford, United Kingdom). The results were reported with 95% confidence intervals (CIs). A P value<0.05 was considered statistically significant on the test for overall effect. To detect publication biases, asymmetry in funnel plots was visually examined.
Sensitivity analysis
Sensitivity analysis was undertaken to evaluate the effect of methodological characteristics of controlled clinical trials in term of trial design, which was differentiated as retrospective, prospective nonrandomized, and randomized. Another sensitivity analysis was undertaken to evaluate the effect of baseline of controlled clinical trials in term of operation, which was differentiated as phocotrabeculectomy and trabeculectomy.
Results
The selection flow of controlled clinical trials is shown in Fig. 1. We reviewed the full text of 12 articles from 118 studies identified from our initial literature search and hand search. A total of 9 studies met criteria for inclusion, and there was one duplicate publication. Therefore, 8 clinical trials involving 536 patients were included in the final meta-analysis.24–31

The selection flowchart of clinical trials included in the present meta-analysis.
Trials characteristics, populations, and quality
The trials were conducted in various countries, including West Africa, United States, India, and Korea. The characteristics of the eligible studies are summarized in Table 1. A total of 589 eyes of 536 patients were enrolled. The duration of follow-up ranged from 6 months to 84 months. Mean age ranged from 47 to 75 years. Among the 262 patients whose sex were available,24,25,27,29 135 were male and 127 were female. Trabeculectomy with intraoperative MMC or 5-FU was undergone in 7 trials, and phacotrabeculectomy was undergone in 1 trial. Three trials had a prospective, parallel, randomized design; 2 had a prospective, nonrandomized design; and 3 had a retrospective, nonrandomized design. The quality assessment is summarized in Table 2. Funnel plots on qualified success rate was asymmetric while funnel plots on IOPR was symmetric (Fig. 2), suggesting probable publication bias.
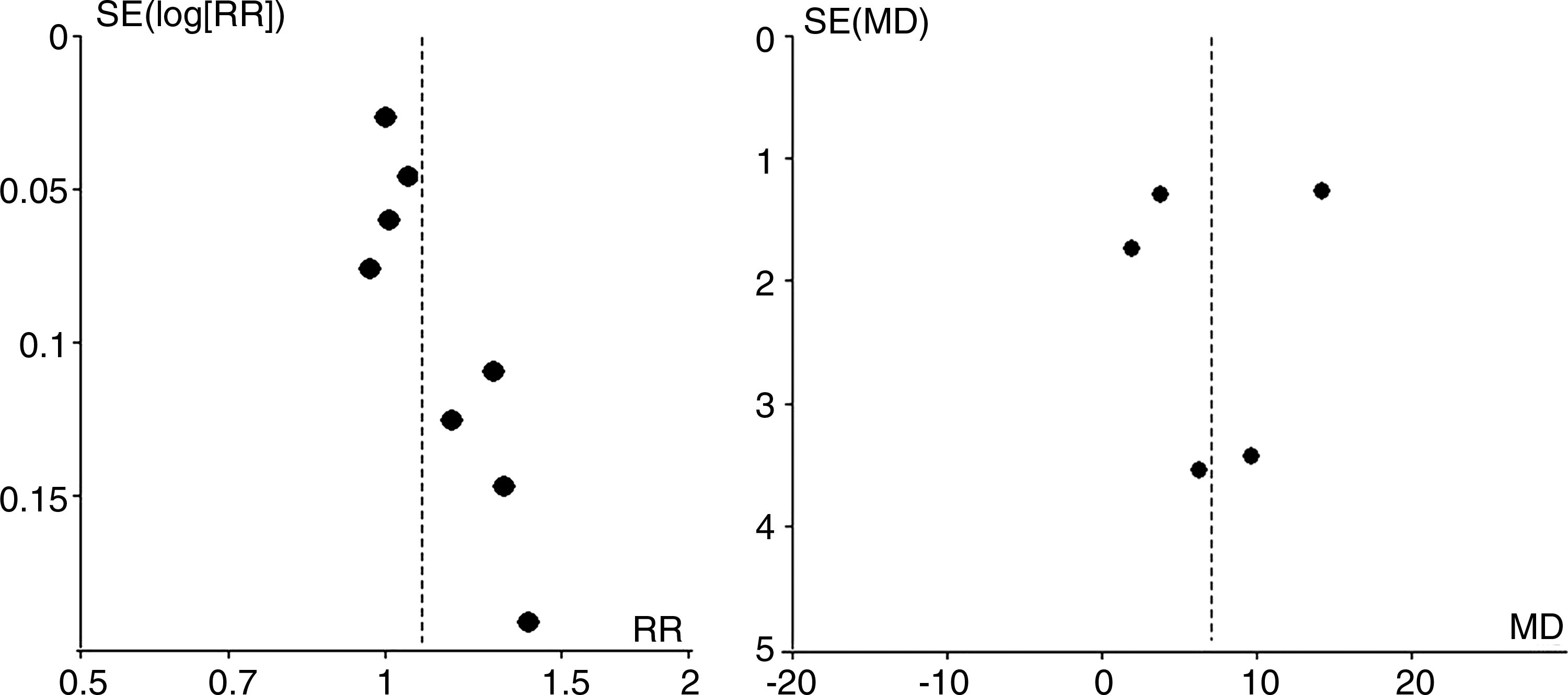
Funnel plot of studies comparing intraoperative mitomycin C (MMC) and intraoperative 5-fluorouracil (5-FU) on qualified success rate (left) and percentage intraocular pressure reduction (IOPR%, right). RR, relative rate; MD, mean difference (both calculated in a random-effects model); SE, standard error.
F-FU, 5-fluorouracil; MMC, mitomycin C; Con, concentration; M/F, male/female; IOP, intraocular pressure; Random, prospective randomized; Retro, retrospective; Pro, prospective nonrandomized; NA, not applicable; PHACO, phacotraceculectomy.
Percentage of IOPR
The percentage of IOPR comparing MMC with 5-FU was reported. Five studies reported data related to IOPR% at various time. We chose the IOPR at follow-up end point (for 1 trial we chose the figure of the 12-month to reduce bias, the others of follow-up end point). MMC was found more effective than 5-FU in lowering IOP. The differences in IOPR% comparing MMC with 5-FU were statistically significant, with WMD 7.09 (95% CI, 1.47–12.70). For the subgroup including RCTs, the differences in IOPR% were also statistically significant (WMD 3.70, 1.23–6.17). For the subgroup including pro-nonrandomized clinical trials, the differences in IOPR% were also statistically significant (WMD 9.61, 2.94–16.28). For the subgroup including retrospective clinical trials, the differences in IOPR% were not statistically significant (WMD 7.53, −1.39–16.46). For the phacotrabeculectomy subgroup, the differences in IOPR% were not statistically significant (WMD 2.00, −1.41–5.41). When excluding the study that phacotrabeculectomy was undergone, the differences in IOPR% were statistically significant (WMD 8.46, 1.99–14.93) (Table 3).
MMC, mitomycin C; 5-FU, 5-fluorouracil; SD, standard deviation; WMD, weighted mean difference (random-effect model); CI, confidence interval. WMDs more than zero denoted an advantage for mitomycin C, and those less than zero denoted an advantage for 5-fluorouracil; 95%CIs of WMDs not including 0 denoted a statistically significant advantage.
Qualified success rate
Eight studies reported the proportions of patients achieving target end point IOP with or without medications at follow-up end point; the difference in qualified success rate between the MMC group and 5-FU group was not statistically significant (pooled RR 1.09, 0.99–1.20). For the subgroup including RCTs, the difference in qualified success rate between the MMC group and 5-FU group was not statistically significant (RR 1.07, 0.94–1.21). For the subgroup including retrospective clinical trials, the difference in qualified success rate between the MMC group and 5-FU group was not statistically significant (RR 1.22, 0.68–2.19). For the subgroup including pro-nonrandomized clinical trials, the difference in qualified success rate between the MMC group and 5-FU group was not statistically significant (RR 1.06, 0.86–1.30). For the phacotrabeculectomy subgroup, the difference in qualified success rate between the MMC group and 5-FU group was not statistically significant (RR 2.00, −1.41–5.41). When excluding the study in which phacotrabeculectomy occurred, the difference in qualified success rate between the MMC group and 5-FU group was not statistically significant, either (pooled RR 1.10, 1.00–1.22) (Table 4).
MMC, mitomycin C; 5-FU, 5-fluorouracil; RR, relative risk (calculated using a random-effect model); CI, confidence interval; Phaco, phacotrabeculectomy.
Complete success rate
Three studies reported the proportions of patients achieving target end point IOP without medications at follow-up end point, the difference in complete success rate between the MMC group and 5-FU group was not statistically significant (pooled RR 1.17, 0.79–1.75). For the subgroup including retrospective clinical trials, the difference in complete success rate between MMC group and 5-FU group was not statistically significant, either (RR 1.46, 0.50–4.25). For the subgroup including pro-nonrandomized clinical trials, the difference in complete success rate between the MMC group and 5-FU group was not statistically significant, either (RR 1.00, 0.89–1.12) (Table 5).
MMC, mitomycin C; 5-FU, 5-fluorouracil; RR, relative risk (calculated using a random-effect model); Retro, retrospective; Pro, prospective.
Side effects
No significant differences comparing between MMC and 5-FU were found in the incidence of bleb leakage, hypotony, endophthalmitis, and shallow anterior chamber, with the pooled RRs being 0.71 (0.22–2.28), 1.40 (0.72–2.72), 1.63 (0.27–9.75), and 0.95 (0.41–2.21), respectively (Table 6).
MMC, mitomycin C; 5-FU, 5-fluorouracil; RR, relative risk (calculated using a random-effect model); CI, confidence interval; AC, anterior chamber.
Sensitivity analysis
Trials designed as retrospective, prospective nonrandomized, and randomized were stratified, and the differences of qualified success rate and IOPR% were compared, respectively. For the subgroup including retrospective clinical trials, the differences in IOPR% were not statistically significant (WMD 7.53, −1.39–16.46). Results of the rest were statistically significant. Trials that included trabeculectomy and phocotrabeculectomy were stratified and the differences of qualified success rate and IOPR% were compared, respectively. For the phacotrabeculectomy subgroup, the differences in IOPR% were not statistically significant (WMD 2.00, −1.41–5.41). Results of the rest were statistically significant.
Discussion
The present systematic review suggested that intraoperative MMC is more statistically effective in IOP lowering in trabeculectomy compared with intraoperative 5-FU, but comparable with intraoperative 5-FU in both qualified and complete success rate. Both agents contribute equally to adverse events.
Abdu et al. analyzed data from 9 clinical trials and reported that intraoperative MMC is comparable with perioperative 5-FU in mean IOP and success rate. 21 In contrast to that analysis, we focused on intraoperative MMC and intraoperative 5-FU instead of perioperative 5-FU and reviewed 8 controlled clinical studies in trabeculectomy, comparing intraoperative MMC with intraoperative 5-FU, and found that intraoperative MMC application was associated with greater IOP-lowering efficacy, with statistically significant differences in IOP reduction compared with intraoperative 5-FU at follow-up end point. However, both groups achieved comparable qualified success rate at follow-up end point.
The first strength of the present analysis is that we focused on direct comparison between intraoperative MMC and intraoperative 5-FU rather than indirect comparison between perioperative MMC and perioperative 5-FU. Furthermore, in the quality assessment of trials, we used a system for both randomized and nonrandomized trials that was definitely better than the Jadad scoring system only for randomized trials. Five (62.5%) of all including studies were nonrandomized design, which may fail to detect actual results. 32 The third strength is that we undertook subgroup meta-analyses by only including randomized clinical trials and subgroup meta-analyses by excluding trials in which phacotrabeculectomy occurred. Two independent co-authors judged the eligibility of articles and extracted data from the eligible articles, with discrepancies resolved after discussion by all of the authors. Only the series of the same patient group at the last end point were included in the present analysis. Asymmetry was showed by funnel plots, indicating less possibility of publication biases.
One major limitation of this analysis was that patients were not stratified into high, medium, and low risk of trabeculectomy failure subgroups, which may possibly produce more interesting results. 33 A second limitation is that our analyses of IOPR, success rate, and adverse events were based on data pooled from trials of different durations. It was due to lack of data reported in all phases of follow-up. It was a compromise proposal to choose the data of follow-up end point. Another limitation is that only published studies were included. To avoid publication bias, we conducted not only an electronic search but also a manual search to identify all potentially relevant articles, including published and nonpublished ones. Unfortunately, it is possible that we may have failed to include some papers, especially those published in other languages. The other limitations are the factors such as small sample size, inadequate allocation concealment, or inadequate or no double blinding, which may greatly affect the interpretation of the results. The inclusion in meta-analysis of studies with very small sample sizes may have a paradoxical effect of decreasing the power of random-effects tests. 34 Therefore, in future, rigorous randomized controlled trials with long enough follow-up and big enough sample size are strongly recommended to further evaluate the real IOP-lowering effect of intraoperative MMC, compared with intraoperative 5-FU in trabeculectomy.
In conclusion, the results of this meta-analysis of 8 randomized controlled trials suggested that intraoperative MMC is more effective in IOP lowering in trabeculectomy compared with intraoperative 5-FU but comparable with intraoperative 5-FU in both qualified and complete success rate. Intraoperative use of both agents may contribute equally to adverse events.
Footnotes
Acknowledgment
This paper was supported by Shanghai Municipal Natural Science Foundation, and National Natural Science Foundation of China.
Author Disclosure Statement
The authors have no competing financial interests.