
Abstract
Abstract
Purpose:
To study the efficacy of a single drug in patients with primary open angle glaucoma and ocular hypertension who were receiving timolol XE 0.5%, latanoprost 0.005% and brinzolamide 1% with its discontinuation.
Methods:
Sixty patients with open-angle glaucoma or ocular hypertension who were administered timolol XE, latanoprost, and brinzolamide were studied. One drug consisting of timolol XE, brinzolamide, and latanoprost was discontinued and 8 weeks later, it was resumed. A change in intraocular pressure (IOP) was studied.
Results:
Mean IOP at baseline and at 8 weeks after discontinuation of each drug was 15.8±1.3 and 17.3±1.4 mmHg in the timolol XE group, 15.8±1.0 and 20.0±1.4 mmHg in the latanoprost group, and 16.0±1.4 and 18.1±1.4 mmHg, respectively. A significant increase in mean IOP was found after drug discontinuation (timolol XE: P=0.0012; latanoprost: P<0.0001; brinzolamide: P<0.0001). The mean change in IOP by discontinuation of the drug was +1.6±0.9 mmHg (+9.6%±5.6%) in the timolol XE group, +4.3±1.7 mmHg (27.4%±12.4%) in the latanoprost group, and +2.2±0.9 mmHg (+13.7%±6.1%) in the brinzolamide group. The change in the latanoprost group was significantly greater compared with those in the timolol XE and brinzolamide groups (timolol XE: mmHg and percent: P<0.0001; brinzolamide: mmHg and percent: P<0.0001). The IOP change in the brinzolamide group was significantly greater than that in the timolol XE group (mmHg: P=0.0417; percent: P=0.0328). No significant difference was observed in mean IOP between before drug discontinuation and at 8 weeks after drug resumption in any group.
Conclusions:
There was a significant increase in IOP from discontinuation of timolol XE, latanoprost, and brinzolamide in the multiple drug treatment. The hypotensive effect of latanoprost in the combined drug therapy is significantly greater than the effects of timolol XE and brinzolamide.
Introduction
Methods
Patients
We studied 60 patients with open-angle glaucoma and ocular hypertension who had received concomitantly timolol XE, latanoprost, and brinzolamide for at least 6 months and whose IOP was low enough not to be considered to deteriorate their disease if 1 of the 3 antiglaucomatous drugs was discontinued. Timolol XE 0.5% (Timoptol XE 0.5%; Santen, Osaka, Japan) and latanoprost 0.005% (Xalatan; Pfizer, New York, NY) were administered once daily, timolol XE in the morning and latanoprost in the evening, and brinzolamide 1% (Eizopt; Alcon, Fort Worth, TX) was administered twice daily. A diagnosis of glaucoma was based on the appearance of the optic nerve head cupping and visual field alteration according to the guidelines of the Japanese Glaucoma Society. 10 Patients with angle closure glaucoma, with any secondary cause of glaucoma, on treatment with oral β-blockers and with any known life-threatening disease were excluded. 11 The study protocol and consent forms were approved by the Human Subjects Committee.
In an open-labeled study, the patients were prospectively randomized to discontinue timolol XE, latanoprost, or brinzolamide with only 1 eye of a patient to be randomized. When both eyes were eligible, the right eye became the study eye. Within 24 h after enrollment, the patients were randomized using an envelope method. In brief, we prepared each 20 envelopes that contained a card which showed either timolol XE group, latanoprost group, or brinzolamide group. Within 24 h after enrollment, an envelope was picked up, and the inside card showed the way to discontinue timolol XE, latanoprost, or brinzolamide. Twenty patients discontinued timolol XE, 20 patients discontinued latanoprost, and the remaining 20 patients discontinued brinzolamide. Treatment began within a week after these random assignments. In consideration of the crossover effect of β-blocker, the administration of the β-blocker, latanoprost, or brinzolamide was discontinued in both eyes if patients were taking 3 drugs in both eyes.
Evaluation of outcomes
Patients read and signed an Institutional Review Board-approved informed consent form before any procedures were performed in this study. Patients had ocular and systemic histories taken and underwent slit-lamp biomicroscopy, visual acuity testing, and dilated funduscopy. Goldmann applanation tonometry was carried out at the same time (±1:00) between 9:00 a.m. and 12:00 p.m. at 3 visits with a 1-month interval, and the mean of the 3 values was calculated to determine the baseline IOP. Three measurements per visit were recorded in each eye, and the mean of these was used in the calculations. The optic nerve was examined with a Goldmann 3-mirror lens, and measurements were taken of the size of the disc, the vertical and horizontal cup/disc ratios, the presence of rim notching or splinter hemorrhage, and the presence of peripapillary atrophy. Visual field testing with a Humphrey visual field analyzer (Humphrey-Zeiss, Dublin, CA) and Program 30-2 SITA STANDARD™ testing were carried out before and 16 weeks after discontinuation of drugs.
Patients who qualified for the study were instructed to discontinue timolol XE, latanoprost, or brinzolamide for 8 weeks and then resume taking the discontinued drug. We asked the patients questions concerning their compliance with treatment and discontinuation more than once per visit to increase the compliance rate.7,9 The patients were reviewed at the interval of 2 weeks for 16 weeks. IOP was measured at the same time (±1:00) as at baseline with Goldmann applanation tonometer, and its change was studied. A single observer took IOP measurements in all eyes.
Patients were also assessed at every visit during the study period for the presence of general and local complications, which included blood pressure change, conjunctival hyperemia, and corneal complications.
Study end
All patients were meant to reach a 16-week follow-up, but the following were considered as endpoints: (1) the need for any further medical or surgical treatment and (2) failure to attend scheduled visits, allowing for a margin of tolerance.
Statistical analysis
Evaluation of continuous variables was achieved using the Student's t-test. To evaluate the difference in IOP between follow-up intervals, the paired t-test was implemented. All t-tests were 2-tailed. Categoric variables were evaluated with chi-square, the Fisher exact test, or the Spearman-rank correlation, when appropriate. A level of P<0.05 was accepted as statistically significant.
Results
Baseline
Baseline data are summarized in Table 1. Sixty patients were enrolled in this study. The mean age was 61.6±11.9 years in the timolol XE group, 62.1±10.6 years in the latanoprost group, and 64.1±9.4 years in the brinzolamide group; there was no significant difference among the 3 groups in age, gender, best-corrected visual acuity, and mean deviation of HFA30-2. All patients had complete follow-up visits and reported to be compliant.
Mean±SD showed mean±standard deviation, and parenthesis indicated range.
IOP, intraocular pressure; POAG, primary open angle glaucoma.
The change in IOP
Mean IOP at baseline and at 8 weeks after discontinuation of each drug was 15.8±1.3 and 17.3±1.4 mmHg in the timolol XE group, 15.8±0.9 and 20.0±1.4 mmHg in the latanoprost group, and 16.0±1.4 and 18.1±1.4 mmHg in the brizolamide group, respectively (Table 2 and Fig. 1). There was no significant difference in mean baseline IOP among the 3 groups. A significant increase in mean IOP was found after drug discontinuation in all groups (timolol XE: P=0.0012; latanoprost: P<0.0001; brinzolamide: P<0.0001) (Table 2 and Fig. 2). Mean change in IOP by discontinuation of the drugs was +1.6±0.9 mmHg (+10.0%±5.7%) in the timolol XE group, +4.3±1.7 mmHg (27.4%±12.4%) in the latanoprost group, and +2.2±0.9 mmHg (+13.7%±6.1%) in the brinzolamide group. The change in the latanoprost group was significantly greater compared with those in the timolol XE and brinzolamide groups (timolol XE: mmHg and percent: P<0.0001; brinzolamide: mmHg and percent: P<0.0001). The IOP change in the brinzolamide group was significantly greater than that in the timolol XE group (mmHg: P=0.0417; percent: P=0.0328). No significant difference was in mean IOP between before drug discontinuation and at 8 weeks after drug resumption in any group. No adverse events were reported during the discontinuation period.
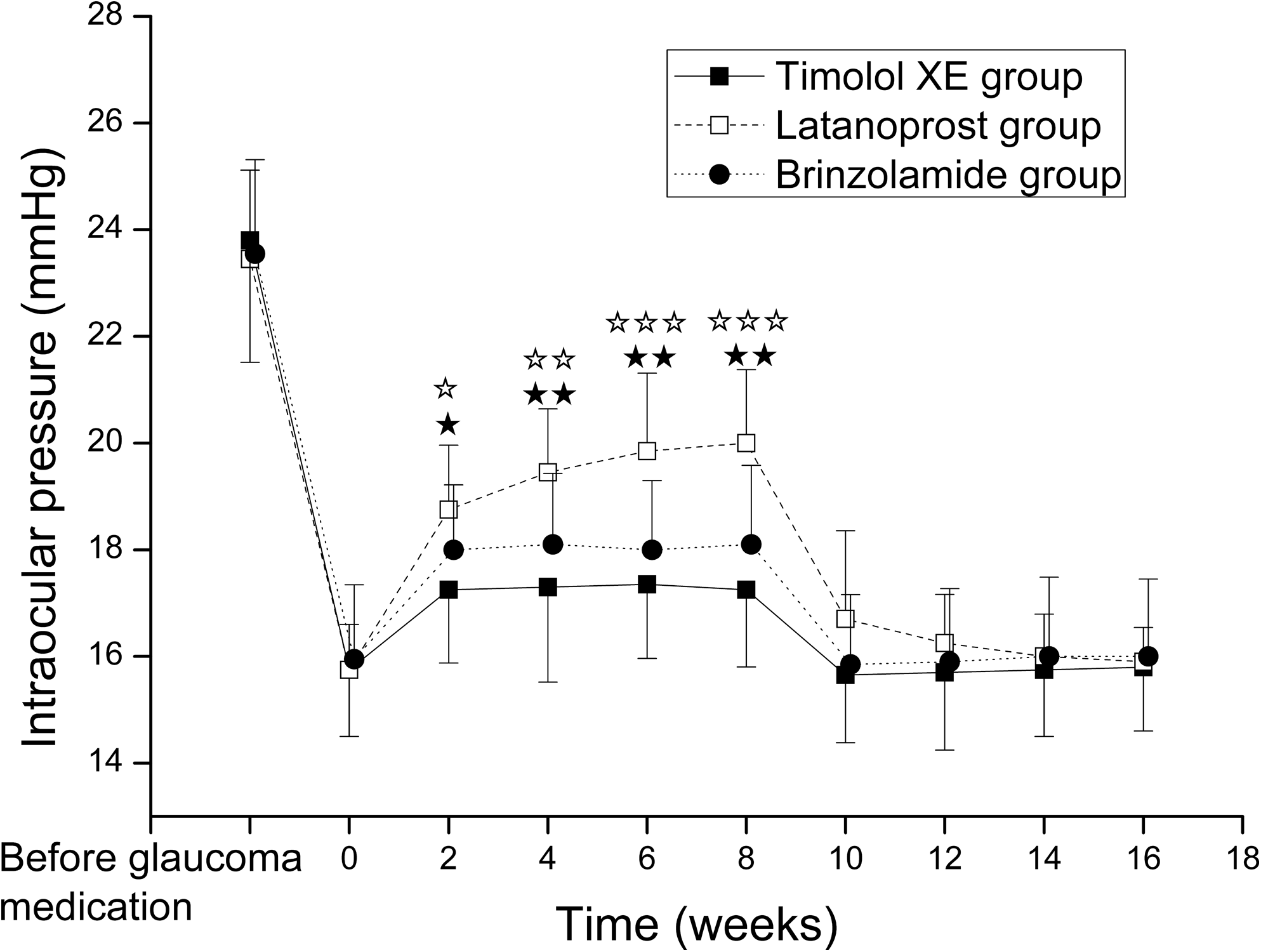
Intraocular pressure (IOP). Solid squares and solid line indicate the timolol XE group, open squares and broken line indicate the latanoprost group, and solid circles and dotted line indicate the brinzolamide group. ★P<0.001; ★★P<0.0001 between the timolol XE and latanoprost groups; *P<0.05; **P<0.001; ***P<0.0005; ****P<0.0001 between the brinzolamide and latanoprost groups.

A change of IOP (mmHg)
Mean±SD showed mean±standard deviation, and parenthesis indicated range.
IOP, intraocular pressure; POAG, primary open angle glaucoma.
Discussion
In the current study, we demonstrated that the discontinuation of timolol XE 0.5%, latanoprost 0.005%, and brinzolamide 1% provided a significant increase in IOP in patients with primary open-angle glaucoma or ocular hypertension who were administered timolol XE, latanoprost, and brinzolamide. The discontinuation of latanoprost produced a significantly greater increase compared with timolol XE and brinzolamide.
In previous studies, although a wide variation existed in washout times among individuals, the mean washout periods of latanoprost, timolol XE, and brizolamide have been reported to be less than 6 weeks, and the majority of the patients reached baseline by 8 weeks after the discontinuation of each drug.12–16 In this study, we assumed that 8 weeks may be sufficient to eliminate the effect of the drugs. Schuman et al. demonstrated that the use of systemic β-blocker reduced the IOP lowering efficacy of topical β-blockers. 11 In this study, patients with systemic β-blocker treatment were excluded. Since latanoprost has been reported to provide an IOP reduction up to 6 months, we enrolled patients who had administered these anti-glaucomatous medications for at least 6 months. 17
In spite of the long-term efficacy of timolol therapy, investigators have noted that the IOPs initially well controlled in some patients slowly increased after several months.13,14 Brubaker also demonstrated fluorophotometrically that the timolol-induced reduction of aqueous flow is less pronounced at 1 year compared with 1 week after beginning treatment. 18 Long-term drift may be related to partial adaptation of the ciliary body to chronic administration of timolol. 19 Though 98% of patients received β-blocker treatment for longer than 12 months, we enrolled patients who had been administered timolol XE for various times, 9–36 months in this study. Shorter duration of treatment with β-blocker may not produce tachyphylaxis from β-receptor downregulation.
Several investigations have compared hypotensive effects of latanoprost, timolol, and carbonic anhydrase inhibitors as adjunctive therapy.20–27 Latanoprost produced a significantly greater reduction compared with β-blockers and carbonic anhydrase inhibitors in all available data except one, in which Alm et al. showed that adding latanoprost to the eyes treated with timolol provide a reduction of 2.6±1.1 mmHg (13%), whereas adding timolol to the eyes receiving latanoprost resulted in a reduction of 2.6±2.2 mmHg (14%).20,21
There were several studies comparing the efficacy of β-blockers and topical carbonic anhydrase inhibitors in multiple drug treatment.22–26 There was controversy on the superiority of the hypotensive effect between β-blockers and carbonic anhydrase inhibitors. Miura et al. showed that the addition of brinzolamide and timolol to latanoprost significantly decreased IOP by 2.0 and 2.7 mmHg, respectively (both: P<0.01), but there were no significant differences between the 2 drugs. 22 O'Conner et al. compared the IOP-lowering effect of β-blocker, dorzolamide, and brimonidine when added to latanoprost. Dorzolamide lowered an additional 3.9 mmHg (19.7%), β-blockers 2.0 mmHg (12.3%), and brimonidine 2.0 mmHg (9.3%) for 1 year; dorzolamide provided a significant greater reduction compared with β-blocker and brimonidine. 23 Travoprost, another type of prostaglandin, is additive to various anti-glaucomatous drugs, including β-blockers and topical carbonic anhydrase inhibitors.24,25 Reis et al. and Hollo et al. demonstrated no significant difference in hypotensive effect between brinzolamide and timolol when administered as an adjuvant to travoprost in the treatment of patients with open-angle glaucoma and ocular hypertension.24,25 We also showed that timolol XE and brinzolamide had a similar hypotensive effect at the time the drug was first administered in patients already receiving latanoprost. 26 The mean reduction in IOP was 11.5%±7.1% by the addition of timolol XE and 12.2%±3.8% by the addition of brinzolamide. In this study, the discontinuation of timolol XE increased the IOP significantly less compared with brinzolamide.
Several investigators demonstrated in the 24 h IOP pattern that antiglaucoma therapies differ in their ability to lower IOP throughout the 24 h day.27–29 Prostaglandin analogs and carbonic anhydrase inhibitors lower both diurnal and nocturnal IOP, while the β-blocker does not lower IOP during the nocturnal period. Although IOP was measured in the morning in this study, maximal IOP change induced by the discontinuation of each drug may not be studied because of the difference of the individual 24 h IOP pattern and peak period of the drugs. Since IOP was measured at the same time (±1:00) as at baseline, the change with the 24 h IOP pattern could be avoided, and the change of the IOP by the drug discontinuation could be studied.
This study has important limitations. The sample size of this study was small, therefore not powered to detect small differences. Small sample size also precluded assessment of safety. Furthermore, a masked study design could have reduced observer bias.
Although the sample size in each group was small, the current study demonstrated that (1) there was a significant increase in IOP from discontinuation of timolol XE, latanoprost, and brinzolamide in the multiple drug treatment; and (2) the hypotensive effect of latanoprost in the combined drug therapy is significantly greater than the effects of timolol XE and brinzolamide. Future studies of a large population are needed to verify these observations. However, this information may be clinically valuable when treating patients with primary open-angle glaucoma and ocular hypertension.
Footnotes
Acknowledgment
There was no commercial sponsorship or support for this study.
Author Disclosure Statement
No competing financial interests exist.