
Abstract
Purpose:
To report a case of refractory atopic blepharoconjunctivitis (ABC) treated by using topical tacrolimus 0.03% dermatologic ointment.
Methods:
A 73-year-old man with ABC was refractory to topical corticosteroid treatment.
Results:
Topical tacrolimus 0.03% dermatologic ointment (Protopic; Astellas Pharma) was applied into the conjunctival fornix twice each day. Dramatic improvement of patient's symptoms was observed during the first week of therapy. Tacrolimus ointment treatment continued for 12 months. No drug-induced conjunctival hyperemia, ocular surface staining, or other adverse changes were noted secondary to the use of the topical tacrolimus ointment.
Conclusions:
Topical tacrolimus 0.03% dermatologic ointment appears to be an effective treatment for ABC that is refractory to conventional therapy.
Introduction
In this case report, we described our experience in treating refractory ABC with topical tacrolimus 0.03% dermatologic ointment, which includes mineral oil, paraffin, propylene carbonate, white petrolatum, and white wax as inactive ingredients.
Case Report
A 73-year-old man with bilateral severe atopic blepharoconjunctivitis (ABC) presented with diffuse eye lid edema with marked secretion, prominent papillar reaction, superficial punctate keratitis, and mucus discharges. He had a 20-year history of atopic skin disease and had primary open-angle glaucoma for 4 years. Visual acuity was 20/20 in both eyes and intraocular pressures (IOP) were 22 mmHg in the right eye and 20 mmHg in the left eye. Fundoscopy showed optic discs with cup/disc ratios of 0.6 ocularis dexter (OD) and 0.7 ocularis sinister (OS). His detailed history included 4 years of latanoprost 0.005% (Xalatan; Pfizer, Inc.) 1×, a dorzolamide 2%/timolol 0.5% combination (Cosopt; MSD) 2×, and brimonidine tartarate 3×(Alphagan; Allergan). His complaints started after switching from latanoprost to travoprost 0.004% (Travatan; Alcon) 2 weeks before presenting with symptoms.
Over the following 6 months, both antiglaucoma and antiallergic medications were used. Use of oral dorzolamide could not be continued because of intolerable systemic side effects. Brimonidine 3×, brinzolamide 1% 2×medications, and a 180° selective laser trabeculoplasty (SLT) procedure failed to drop IOP efficiently. The patient declined trabeculectomy operation. While latanoprost lowered IOP to 16 mmHg in the right eye and 14 mmHg in the left eye, significant worsening of blepharoconjunctivitis was observed. Despite a 6-month-long treatment consisting of prednisolone 1% (Pred Forte; Allergan) 4×, dexamethasone ointment (Maxidex; Alcon) 4×, and cyclosporine 0.04% 3×(Restasis; Allergan), ABC flared each time we attempted to stop these medications. The patient was diagnosed as corticosteroid dependent and was fully informed about tacrolimus treatment. Topical tacrolimus 0.03% dermatologic ointment was applied into the temporal conjunctival fornix twice a day. After the first week, the patient's symptoms diminished dramatically, improving completely during the first 15 days of the therapy (Fig. 1). In the first 2 months, tacrolimus was used 2×, and then tapered to 1×for 10 months. After the first year, flaring of ABC was seen after tacrolimus application was stopped; the patient was instructed to use tacrolimus continuously 3 times a week and to increase the dose if his complaints increased. No drug-induced conjunctival hyperemia, ocular surface staining, or other adverse changes were noted secondary to the use of topical tacrolimus.
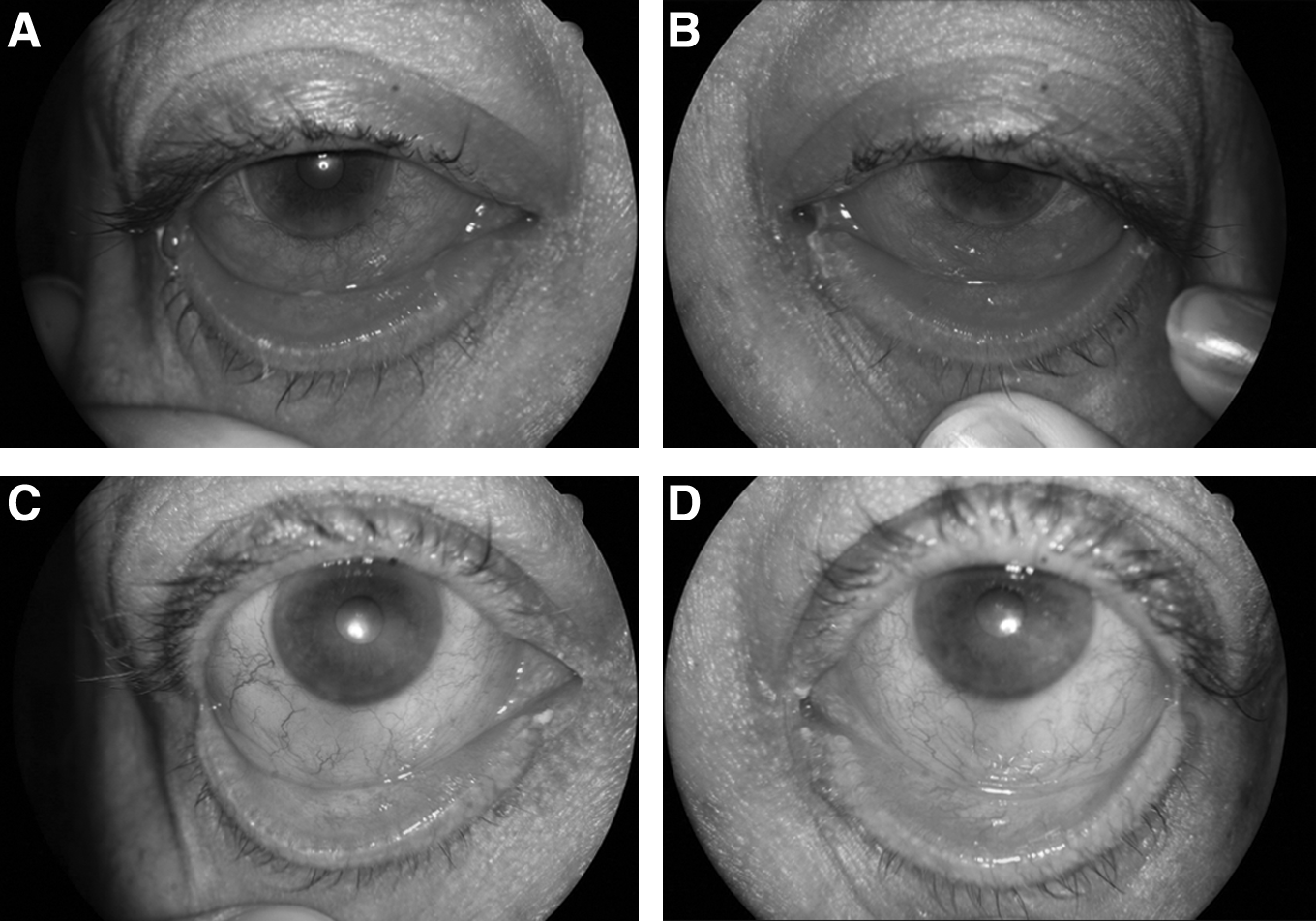
Severe blepharoconjunctivitis despite topical corticosteroid use
Discussion
Off-label topical use of tacrolimus 0.03% dermatologic ointment was found to be effective, safe, and well tolerated in patients with atopic eyelid disease, refractory ocular surface inflammatory disease, giant papillary conjunctivitis, ABC, allergic conjunctivitis, and ocular cicatricial pemphigoid that are refractory to conventional treatment.3–6 Tacrolimus ointment did not cause progression of corneal epithelial defects in corneal shield ulcers, ulcerative keratitis, Mooren's ulcer, 4 or worsening of descemetocele. 5 Additionally, tacrolimus 0.06% eye drop was well tolerated after keratoplasty and gave comparable results to prednisolone acetate 1% when used postoperatively 3 times a day for 6 months.4,5 Joseph et al. reported a case in which topical tacrolimus spared the patient from keratoplasty surgery. 5 Similarly, Miyazaki et al. reported a case in which topical tacrolimus halted the corneal perforation. 4 Interestingly, application of tacrolimus ointment only to the eyelid also caused improvement of corneal and conjunctival inflammation.4,5 In a retrospective study, a decrease was observed in eosinophils, neutrophils, and lymphocytes in the conjunctival cytology samples after tacrolimus ointment treatment. 7 Herpes simplex keratitis was a single reported complication of topical tacrolimus. 5 Skin atrophy, which is a well-known complication of long-term corticosteroid use, was not reported secondary to long-term use of tacrolimus ointment. 1 Similarly, we did not observe any side effects in this case and the patient tolerated tacrolimus ointment well.
A case report of allergic reactions to prostaglandin analogs was reported before. 8 In our case, we accused travoprost, a topical prostaglandin F2 α analog, of triggering ABC. Since the patient declined trabeculectomy operation, we had to use latanoprost, which belongs to same group, to prevent glaucomatous optic nerve damage but ABC nevertheless flared again. It was not easy for the patient to instill the tacrolimus ointment into the inferior conjunctival fornix himself. We discovered that when the tip of the ointment was placed and pressed into the temporal edge of the eyelid, the ointment was easily broken into pieces.
In conclusion, topical tacrolimus 0.03% dermatologic ointment seems to be an effective alternative treatment for ABC that is refractory to conventional therapy. Further prospective studies with longer follow-up periods and larger series are needed to evaluate the long-term efficacy of this therapeutic approach.
Footnotes
Acknowledgment
The authors state that no grants or funds were received.
Author Disclosure Statement
Neither author has a financial or proprietary interest in any material or method mentioned. The authors state that no financial support was received.