
Abstract
Abstract
Purpose:
To describe a case of 68-year-old male industrial chemist who received a chemical injury after a gold/amine compound exploded causing bilateral eye injuries. No apparent long-term problems were anticipated. After cataract extraction 40 years later, he developed a localized ulcerative keratitis adjacent to embedded gold in the cornea.
Methods:
To describe the clinical features, management, and outcomes.
Results:
Successful treatment with topical hydrocortisone was achieved. Subsequently, 3 further episodes of ulcerative keratitis were treated with topical steroid therapy without need for systemic immunosuppression. A systemic vasculitic/autoimmune screen was normal.
Discussion:
Ocular chrysiasis is well recognized after systemic gold administration and is normally considered inert, but in this case exogenous gold deposition might have been a contributing factor to very localized and repeated episodes of stromal erosion in this man, many years after the original injury. To the best of our knowledge this is the first such reported case.
Introduction
Case Report
A 68-year-old male industrial chemist sustained a chemical injury in 1957 after preparing a gold amine solution, which was left to evaporate. The resulting powder subsequently exploded causing bilateral eye injuries, but at that time no apparent long-term problems were anticipated.
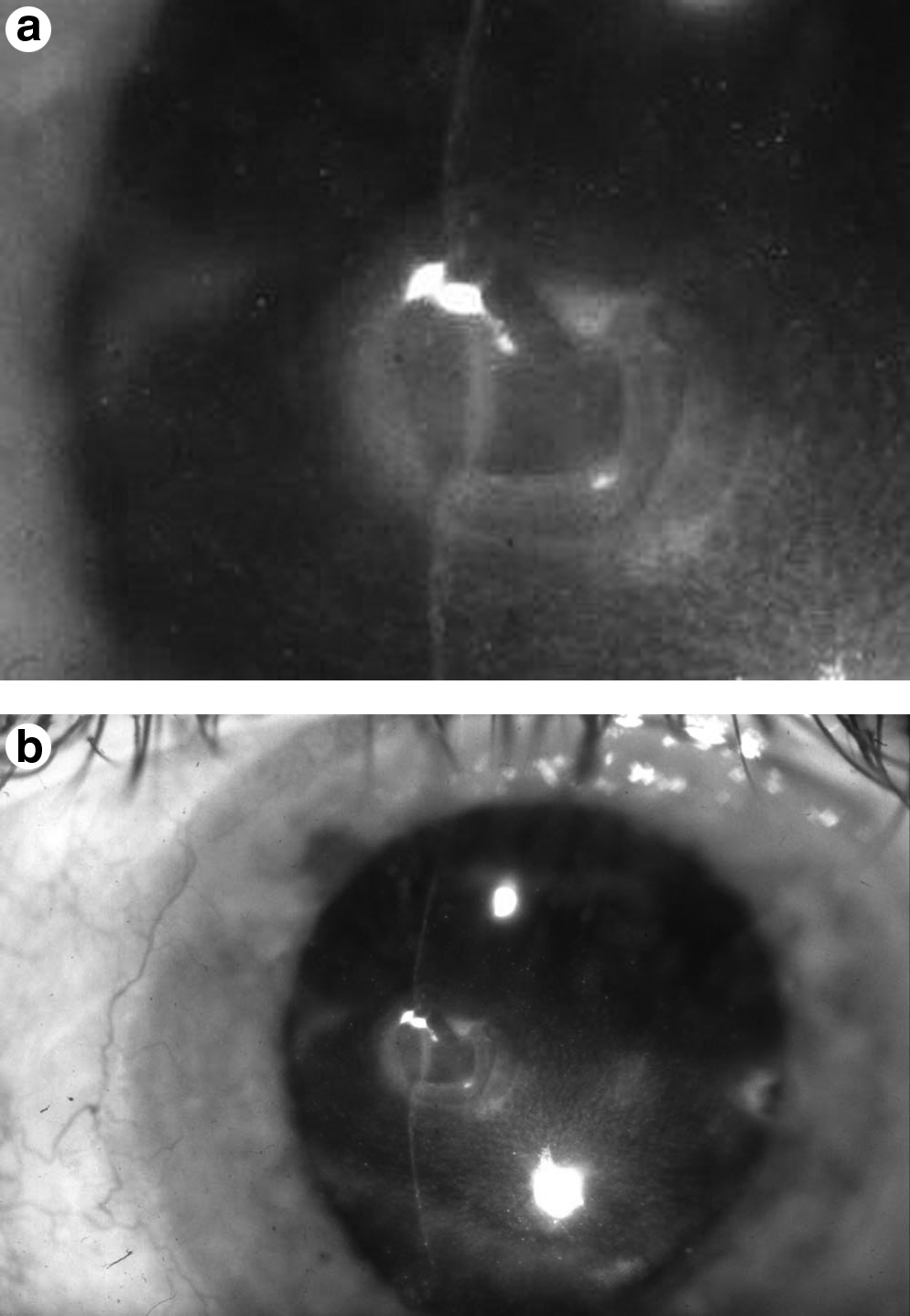
In 1998, the patient attended eye clinic with pain and photophobia in the left eye. He had incidentally undergone routine phacoemulsification cataract extraction in 1997. On examination, his visual acuity was 20/80 in the left eye. He had multiple embedded deposits of gold particles in both conjunctivae and throughout corneal stroma (Fig. 1a). On the left cornea 2 large nebulae deep to Bowman's membrane with central golden glistening particles were found with an area of stromal keratitis and erosion surrounding the nasal deposit (Fig. 1b). Before referral to the corneal service in our department, treatment had been commenced with topical Aciclovir 3% and Ciprofloxacin 0.3% with no improvement. Findings suggested a noninfective keratitis that resolved with minimal scarring on topical hydrocortisone, chloramphenicol 0.5%, and cyclopentolate 1%. Vasculitic screen (Rheumatoid Factor; Anti-Neutrophil Cytoplasmic Antibody; Anti-nuclear, mitochondrial, smooth muscle, and parietal cell antibodies; erythrocyte sedimentation rate and C reactive protein) were normal. Subsequently, 3 further episodes of ulcerative keratitis were treated with topical steroids.
A conjunctival biopsy was taken and demonstrated epithelioid granulomata. Energy dispersive X-ray spectroscopy analysis was requested but unfortunately not completed for reasons beyond our control. He recovered well from the last episode of keratitis and has remained symptom free on g. prednisolone 0.5% od with a visual acuity of 20/30 In the left eye.
Discussion
The term “chrysiasis” is derived from the Greek word chrysos and refers to the deposition of gold in tissues, and in particular the skin. It was first described in 1928 in a 20-year-old woman who showed a slate-gray pigmentation affecting the light-exposed areas and had received 12.3 g parenteral sodium aurothiosulphate.1–3 Widespread deposit of gold occurs in patients who have received a cumulative dose >1 g in conditions such as rheumatoid arthritis. 4 McCormick et al. 4 examined 34 patients who had received over 1 g of gold compounds for rheumatoid arthritis for ocular chrysiasis. Ninety-seven percent of the patients receiving continuous chrysotherapy at the time of their ocular examination exhibited corneal chrysiasis. With few exceptions, corneal gold deposits were limited to the posterior one-half of the corneal thickness. Deposits tended to concentrate inferiorly and to spare the superior and peripheral cornea. Duration of chrysotherapy correlated positively with the clinically graded density of deposits. In their series, 55% (16/29) of these patients receiving gold therapy for 3 years or more had lenticular chrysiasis, although this has previously been considered rare. It was also suggested that gold is deposited in the cornea and lens from the anterior chamber aqueous fluid. 4
Deposition of gold in ocular structures, particularly in the cornea, is termed ocular chrysiasis.5,6 Corneal deposits can be limited to the epithelium or the stroma. 6 Two variants of gold-induced keratopathy (corneal chrysiasis) have been described. 7 The more common variant manifests as asymptomatic deposition of fine brown or purple granules in the central posterior corneal stroma, sparing the periphery. Other patterns include peripheral deposition with extension toward the central cornea, superficial, and deep axial deposition. 4 Corneal gold deposition by itself is not considered an indication to discontinue gold therapy. 4 The second variant of keratopathy presenting with inflammatory symptoms and signs is, however, rare. They might have marginal interstitial keratitis that may ulcerate, with white, subepithelial limbal infiltration and deep, brush-like stromal vascularization.7,8 Crescent-shaped marginal ulcers 2–3 mm in length may also be present. This variant is presumed to be an idiosyncratic reaction.7,8 It may be unilateral or bilateral, and is considered an indication to stop gold therapy. 7 The underlying pathogenic mechanism, as well as the possible associations with other systemic gold toxicity, is unknown. This seems a likely mechanism in our case with the likelihood of disturbed gold particulates in the cornea following the cataract surgery; however, it must be noted that the keratitis was away from the corneal section and the side port entry wounds. It is notable that the keratitis in our case was responsive to topical corticosteroids and recurred after steroid withdrawal. A similar response has been reported in systemic manifestations of gold toxicity.9–11 Zamir et al. 11 reported a case of recurrent gold-induced interstitial keratitis in a 60-year-old woman with rheumatoid arthritis who had intramuscular injections of gold sodium thiomaleate (50 mg once weekly) and a cumulative dose of 7.4 g of gold over 3 years. Her recurrent keratitis was treated by topical steroids and by stopping the gold therapy. This patient, like ours, required long-term maintenance steroid drops to keep the keratitis in remission.
On histopathologic evaluation, gold deposits are present both intracellularly and extracellularly without any inflammatory reaction. 6 Gold compounds can produce 2 types of ocular lesions—chrysiasis and inflammation or ulceration of the cornea.12–14 The latter may be a manifestation of an allergic reaction and hypersensitivity to gold. In yet one study 15 corneal changes (punctuate keratitis and corneal thinning) were seen in 62% of cases after the use of gold foil electrodes in electroretinography. However, all changes were transient, and there were no serious sequelae in any of the subjects. There was, however, significant association between the severity of the corneal changes and 2 factors; the age of the subject and the use of topical anesthetic drop. 15
Ever since its first use in 1927 colloidal gold therapy has been effective in slowing the progression of rheumatoid arthritis, and therefore patients who respond favorably are usually kept on maintenance therapy for many years, 16 and occurrence of asymptomatic ocular chrysiasis generally does not require discontinuation of gold therapy. The diagnosis of gold keratopathy should be considered in patients with rheumatoid arthritis who present with marginal keratitis. Assessment of possible systemic toxicity is warranted and cessation of therapy should be considered in such cases. Patients should be continuously followed, since stromal inflammation may recur even after cessation of gold therapy.
Ulcerative keratitis may be associated with systemic collagen vascular disease. The mechanism involves a breakdown of a complex cytokine-mediated regulatory system, which may lead to a corneal ulcer. There was no evidence for an infective or autoimmune etiology in this patient, he was not immunosuppressed, and he had never received systemic gold treatment. It may be argued that the apparent thermal injury from the initial trauma might have played a part in this clinical scenario; however, the arguments against that are the facts that the thermal injury was a single event, but not only were the gold particles persistent to date, but also the areas of ulceration were limited to areas of the particular deposits and crucially there were areas of stromal scarring/haze consistent with inflammatory processes that were clearly focused around shiny golden particles. This led us to the apparent conclusion that the gold was a contributory factor in this case.
Elemental gold is normally considered inert, yet seems to have contributed to very localized and repeated episodes of stromal erosion and scarring in this man, many years after the original injury. To the best of our knowledge, this is the first such reported case of exogenous gold deposition in such a manner. Furthermore, we propose that its deposition in the cornea after the first accident and subsequent disturbance after cataract surgery was the cause of a possible idiosyncratic reaction and the related keratitis and melt.
Footnotes
Author Disclosure Statement
No competing financial interests exist.