
Abstract
Abstract
Purpose:
Cystoid macular edema (CME) is a rarely reported side effect of nanoparticle albumin bound (nab)–paclitaxel therapy—an antimitotic agent used for breast cancer. We describe a patient with bilateral CME secondary to Abraxane that was minimally responsive to intravitreal bevacizumab. To our knowledge, this is the first reported case of the use of intravitreal bevacizumab for this condition. A previous report has described the ineffectiveness of concurrent intravenous bevacizumab with Abraxane. This lack of efficacy and knowledge of the mechanism of paclitaxel may provide insights into the mechanisms of CME without angiographic leakage.
Methods:
Retrospective, interventional case report of a patient with bilateral CME after starting Abraxane therapy for recurrent breast cancer treated with intravitreal bevacizumab (1.25 mg/0.05 mL) every 4 weeks. Records were reviewed for visual acuity and macular edema as assessed by spectral-domain optical coherence tomography (SD-OCT).
Results:
A 73-year-old patient with recurrent, metastatic breast cancer presented with bilateral visual loss 3 months after nab-paclitaxel was initiated. Baseline visual acuities (VA) were 20/50 in the right eye (OD) and 20/80 in the left eye (OS). Fundus exam showed marked CME in both eyes (OU). Fluorescein angiography was notable for the marked absence of petalloid late-phase leakage characteristic of vascular, ischemic, and inflammatory causes of CME. SD-OCT showed marked cystoid spaces predominantly involving the outer and inner nuclear layers with central subfield thicknesses (CST) of 398 μm OD and 441 μm OS. Serial intravitreal bevacizumab injections (OD, 2 injections; OS, 3 injections) were administered on a 4-week basis with an improvement and stabilization of VA at 20/50 OD and 20/70 OS. However, CME on SD-OCT persisted with CST of 492 μm OD and 478 μm OS.
Conclusions:
The pathogenesis of CME without leakage is poorly understood; however, fluid accumulation in Muller cells due to toxicity has been proposed. The persistence of CME suggests that additional nonvascular endothelial growth factor–mediated mechanisms are involved. Improved understanding of the mechanisms underlying paclitaxel-associated CME is needed, especially in patients with limited systemic options for metastatic carcinoma.
Introduction
Case Report
A 73-year-old patient with recurrent, metastatic breast cancer was presented with bilateral visual loss 3 months after nab-paclitaxel and intravenous bevacizumab were initiated. She had no previous significant past medical history or past ocular history. Baseline visual acuities (VA) were 20/50 right eye and 20/80 in the left. Anterior segment was unremarkable in both eyes. Funduscopic examination showed marked CME in both eyes. FA was notable for the marked absence of petalloid late-phase leakage characteristic of vascular and inflammatory causes of CME (Fig. 1). Spectral domain optical coherence tomography (SD-OCT) showed marked cystoid spaces predominantly involving the outer and inner nuclear layers with central subfield thicknesses (CST) of 398 μm OD and 441 μm OS. After obtaining informed consent, serial intravitreal bevacizumab injections (OD, 2; OS, 3 injections) were administered on an every 4-week basis with stabilization of VA at 20/50 OD and 20/70 OS. However, CME on SD-OCT persisted with CST of 492 μm OD and 478 μm OS (Fig. 2) at 4 months of follow-up. Nab-paclitaxel infusions were continued during this period per oncology recommendations. Due to deterioration in her health, the patient was unable to return for follow-up.
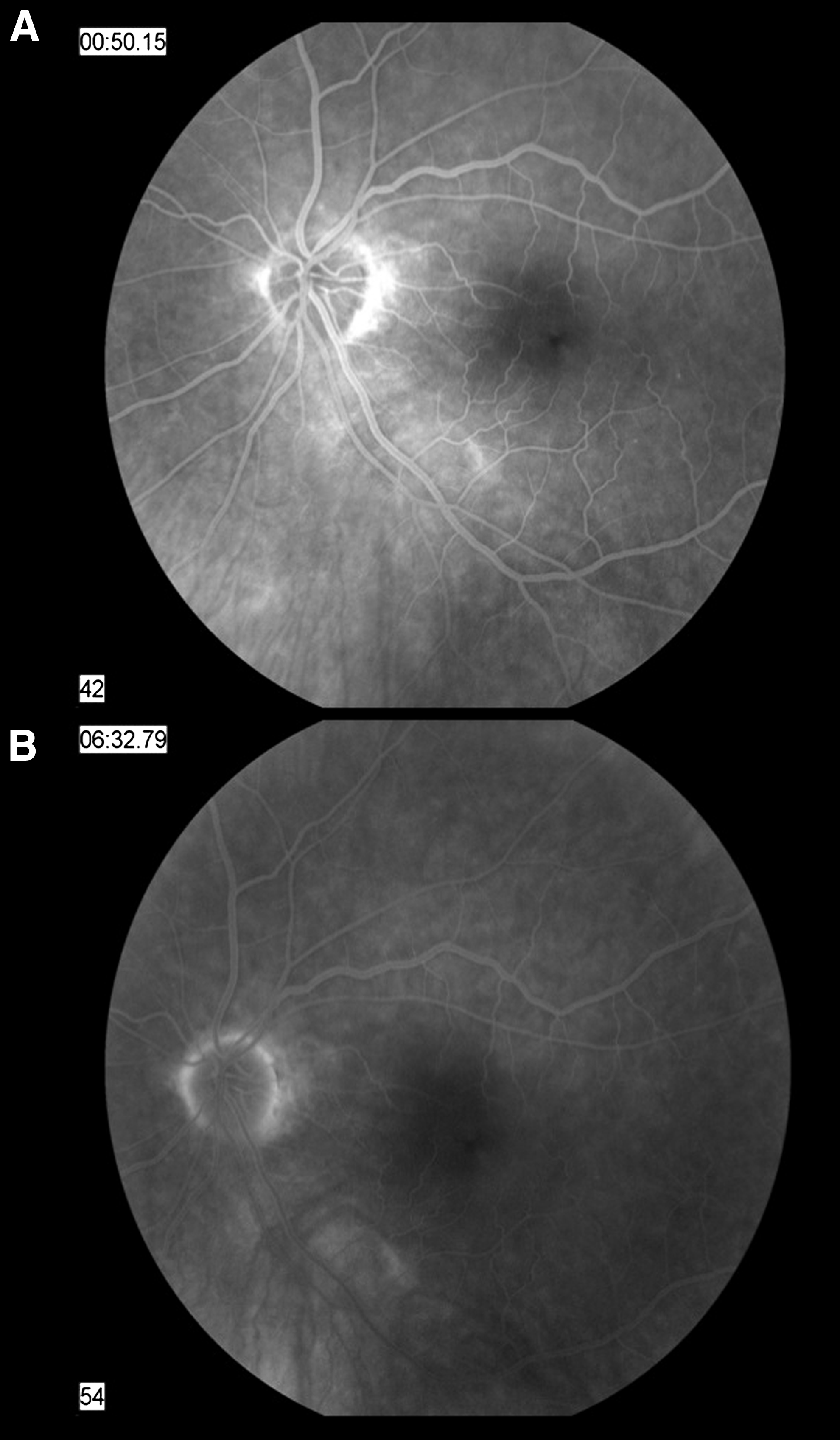
Fluorescein angiography reveals normal vascular filling in the early frames
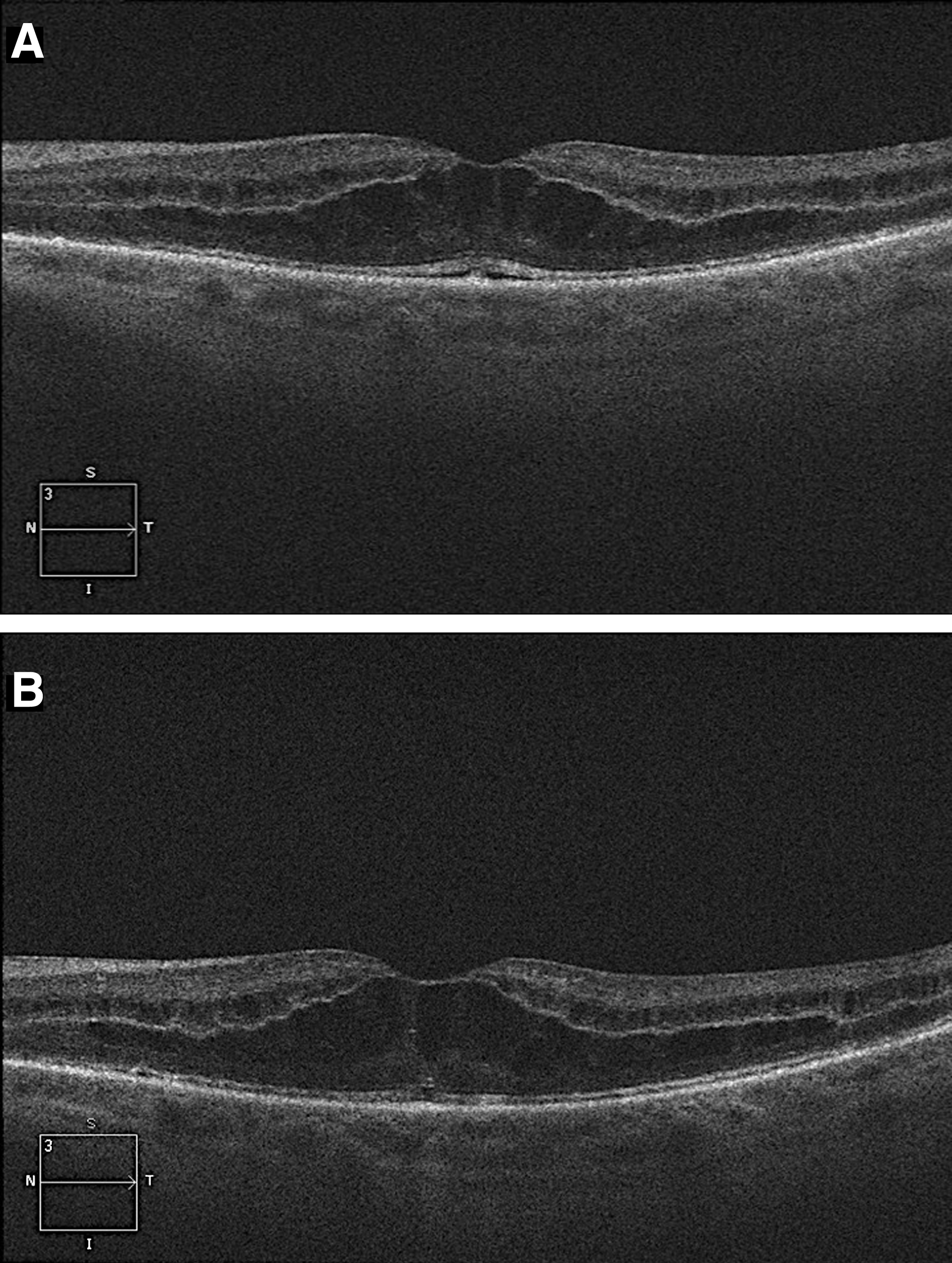
Spectral domain optical coherence tomography imaging shows a small neuroepithelial detachment and significant cystoid macular edema (CME) on presentation for the left eye
Discussion
Visual disturbances have been reported in 13% of patients receiving nab-paclitaxel with 1% classified as severe. 1 The majority of visual changes (i.e., keratitis and blurred vision) were reported in patients receiving doses higher (i.e., 300 or 375 mg/m2) than the currently recommended dose of 260 mg/m2 administered every 3 weeks.
The precise mechanism underlying taxane-associated CME is not known; however, CME typically has resolved in the few reported cases following medication cessation.2–5 In our patient with advanced metastatic breast cancer, nab-paclitaxel was the only medication to which she had a favorable response, thus the desire to continue the medication if possible. The off-label use of intravitreal bevacizumab has become a safe and acceptable treatment for a variety of etiologies of CME.6,7 However, our patient's minimal response by SD-OCT to intravitreal bevacizumab suggests that nonvascular endothelial growth factor–mediated mechanisms of CME are likely involved. This is further supported by Baskin and Garg's recent report describing the inability of systemic bevacizumab to prevent nab-paclitaxel-associated CME. 5
An improved understanding of taxane-associated CME may potentially provide insight into other subtypes of CME without capillary leakage, which is an incompletely understood observation. One proposed mechanism is intracellular fluid accumulation due to direct cellular toxicity of Muller cells, 8 which are critical to stabilization of retinal architecture and the provision of metabolic and structural support to retinal neurons and blood vessels. It is not clear whether taxane derivatives are directly toxic to Muller cells or whether their microtubule-inhibiting action may lead to disruption of Muller cell structure, function, and subsequent accumulation of intracellular edema. Interestingly, microtubule organization and alignment parallel to the long axis of a cellular process does appear to be a feature of cultured human Muller cells. 9 Fortunately, taxane-associated CME appears to be reversible following cessation2–5 ; however, in patients with limited systemic options for the treatment of metastatic cancer, optimizing a local therapy while on this class of chemotherapeutic agents would be beneficial.
Footnotes
Acknowledgment
Funding/Support
Author Disclosure Statement
The authors have no proprietary interest in any contents within this article and no competing financial interests exist.