
Abstract
Abstract
Purpose:
This study aimed to evaluate the safety and long-term effects of infliximab on chronic noninfectious uveitis with measuring best corrected visual acuity (BCVA) and central macular thickness (CMT).
Method:
Ten eyes of 7 patients were included in this prospective case series. All the patients had noninfectious anterior and posterior uveitis that was unresponsive to conventional treatments for 3 months. About 1.5 mg of infliximab in 0.15 cc was injected intravitreally and the patients were followed for 6 months. BCVA was measured by Snellen chart and grading of vitritis was measured according to binocular indirect ophthalmoscope score before injection, 4 weeks, 3 months, and 6 months after the injection. CMT was measured 1 day before injection and compared with the same factors 4 weeks and 6 months after the injection.
Results:
Mean of LogMAR before injection was 1.37±0.43 that changed to 0.67±0.55 and 1.38±0.36 one month and 6 months after the injection, respectively. Mean CMT before injection was 673.2±338.39 that changed to 456.4±317.46 and 659.3±342.48, 4 weeks and 6 months after the injection, respectively. Mean vitreous haziness grade before injection, 4 weeks, 3 months, and 6 months after the injection was 2.7, 0.95, 2.3, and 2.6, respectively.
Conclusions:
Intravitreal Infliximab may be used in treatment of noninfectious uveitis. It probably improves the vision and decreases the macular edema but its effect is temporary and repeated injections may be needed to achieve the best therapeutic goal.
Introduction
Intravitreal injection of infliximab was used in experimental endotoxin-induced uveitis in the animal model. 7 It was also administered for age-related macular degeneration (AMD) without significant side effects. 8 Recently, intravitreal infliximab has been used for treatment of sight-threatening noninfectious chronic refractory uveitis in the human eye with acceptable results and no significant toxicity in short term. 9 Intravitreal infliximab might be immunogenic and retinotoxic and it must be furthur investigated. 10
We had conducted an earlier study, the results of which were published in the journal Retina (October 2010). Over a 4-week period, we had observed a group of patients and reported on the short-term effects of infliximab. 9 In this current study, we followed the same group of patients over a 6-month period to study the long-term effects of intravitreal infliximab on sight-threatening noninfectious chronic uveitis in the human eye.
Methods
This is a prospective study conducted after receiving informed consent and institutional review board approval on 7 patients referred to Poostchi Eye Clinic from March 2008 to April 2009 with the diagnosis of noninfectious anterior and posterior uveitis according to Standardization of Uveitis Nomenclature (SUN) working group definitions. Also, they showed no response to conventional uveitis treatments (including topical and systemic immunosuppressive therapy other than infliximab) in the previous 3 months. Informed consent was received from all patients.
Complete systemic (including rheumatologic consult) and ophthalmic examination was performed for the patients. Best corrected visual acuity (BCVA) with Snellen chart, tonometry, slit lamp examination, and fundoscopy were done for all patients. Macular optical coherence tomography (OCT) (Stratus Carl Zeiss Meditec, Dublin, CA) for central macular thickness (CMT) was done for them before injection. The grading of vitritis was noted according to binocular indirect ophthalmoscope (BIO) score. BIO score graded from 0 to 5. Zero correlating with nil haze, 1 signifying minimal haze with clearly visible posterior pole, 2 correlating with mild haze and the posterior pole with slight haze, 3 signifying moderate haze, 4 signifying marked haze with obscured details of posterior pole, and 5 correlating with severe haze and no details visible.
On the day of injection, in the operating room, each eye was prepped with betadine 5% solution after administration of topical tetracaine. After draping the eyes, 1.5 mg of infliximab in the total volume of 0.15 cc was injected from pars plana into the vitreous cavity. After the injection, topical eye drops of ciprofloxacin was used for three consecutive days in order to decrease the chance of endophthalmitis. Oral acetazolamide was also administered to decrease the intraocular pressure 1 h before injection. All other anti-uveitis drugs were not changed.
All the patients were followed 1 day, 1 week, 4 weeks, 3 months, and 6 months after the injection. In all of the postinjection sessions, slit lamp examination, tonometry, and fundoscopy were done for all patients. BCVA and grade of vitritis were measured in all visits. BCVA with Snellen chart and OCT for measuring CMT were done for each patient at 4 weeks and 6 months after injection.
All the data were gathered and analyzed with SPSS version, 19.0. BCVA was converted to LogMAR before analysis. P value of<0.05 was considered as statistically significant in this study.
Results
Ten eyes from 7 patients were enrolled in this study with the mean age of 26.57 and standard deviation of 12.79 in the range of 11 to 50 and median age of 25 years. One of the patients was a man and 6 of them were women. Four of the patients had Behcet's disease, one had juvenile rheumatoid arthritis, one had multifocal choroiditis and panuveitis, and one patient had pars planitis of unknown etiology (Table 1).
OD, right eye; OS, left eye; JRA, juvenile rheumatoid arthritis; PP, pars planitis; MCP, multifocal choroiditis and panuveitis; BCVA1, LogMAR best corrected visual acuity 1 day before injection; BCVA2, LogMAR best corrected visual acuity 4 weeks after injection; BCVA3, LogMAR best corrected visual acuity 3 months after injection; BCVA4, LogMAR best corrected visual acuity 6 months after injection; CMT1, central macular thickness 1 day before injection; CMT2, central macular thickness 4 weeks after injection; CMT3, central macular thickness 6 months after injection (data before injection and 4 weeks after injection were first presented in reference number 9).
Mean logarithm of the minimum angle of resolution (LogMAR) of BCVA was 1.37±0.43 with a range of 1.00 to 2.07 one day before injection, which then changed to 0.67±0.56 with a range of 0.30 to 1.78 at 4 weeks after injection and 1.18±0.42 with a range of 0.70 to 1.77 and 1.38 with a range of 1.00 to 1.77 at 3 and 6 months after injection (Table 1).
The P value of these changes was <0.001, which means that these figures have statistical difference as a whole. There was also statistical difference between values of preinjection and 4 weeks after injection (P=0.001), and between 4 weeks after injection and 3 and 6 months after injection (P=0.002). No difference, was seen between mean LogMAR of preinjection and ′3 and 6 months after injection (P=0.109 and P=0.884).
Mean vitreous haziness grades before injection, 4 weeks, 3 months, and 6 months after injection were 2.7±0.82, 0.95±0.43, 2.3±0.67, and 2.6±0.51, respectively. Median and range of vitreous haziness grade before injection was 3 and 1 to 4, respectively. Median and range of vitreous haziness grade 4 weeks after the injection was 1 and 0.5–2, 3 months after the injection was 2 and 1–3, and 6 months after injection was 3 and 2–3, respectively (Fig. 1). P value of changes of vitreous haze between preinjection, 4 weeks later, and 3 months later is <0.001 as a whole. Mean vitreous haziness grades before and 4 weeks after injection were 2.70±0.82 and 0.950±0.43, respectively (P<0.0005). P values of changes between preinjection and 3 months later, and between 4 weeks after injection and 3 months after that are 0.037 and<0.001, both of which are statistically significant.
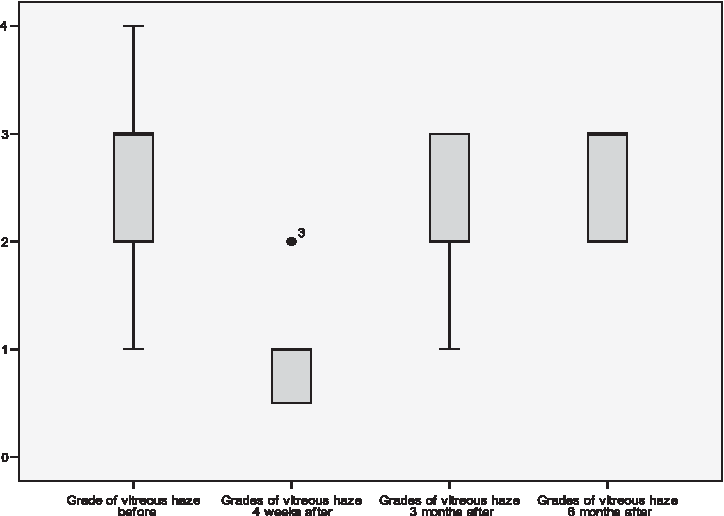
Grades of vitreous haze 1 day before, and 4 weeks, 3 months, and 6 months after injection, according to binocular indirect ophthalmoscope (BIO) score (data befor injection and 4 weeks after injection were first reported in reference number 9).
Mean of CMT before injection was 673.2±338.39 that changed to 456.4±317.46 and 659.3±342.48 four weeks and 6 months after injection, respectively, with the whole P value of 0.01. There was also a statistical difference between CMT values of preinjection and 4 weeks after injection (P=0.01), and between 4 weeks after injection and 6 months after injection (P=0.02). No difference was seen between mean CMT of preinjection and 6 months after injection (P=0.703) (Table 1).
No significant ocular or systemic complication related to injection of infliximab was seen during this study except for mild subconjunctival hemorrhage that was resolved in 10 to 14 days spontaneously.
Discussion
TNF-α antagonists are effective anti-inflammatory drugs in various systemic diseases, such as Behcet's uveitis, Crohn's disease, VKH (Vogt-Koyanagi-Harada), and rheumatoid arthritis.11–14 Their route of administration in rheumatologic diseases is mostly systemic. Systemic use of infliximab has some reported complications; the most important of which are heart failure, exacerbation of multiple sclerosis, immunologic and allergic reactions, and reactivation of tuberculosis. 1 Local administration of this drug may have benefits, such as decreasing the systemic complications as well as increase in the effective dosage for the retina, choroid, and vitreous. Although blood–retinal barrier is disrupted in uveitis, the dosage of infliximab is far less than that would cause any systemic complications. 15 However, it should be kept in mind that retinal toxicity is the major concern when using intravitreal drugs.
Many studies have been done for ocular safety of intravitreal infliximab. The results indicated that infliximab may be a safe intravitreal drug in the animal model at a dose of up to 2 mg. It is also used for neovascular AMD.7,8,16
Short-term report of intravitreal infliximab for sight-threatening noninfectious uveitis also showed acceptable results without significant sight-threatening complications. It can improve the visual acuity and decrease macular edema in uveitic patients. 9 A recent report about the safety of intravitreal infliximab in patients with refractory diabetic macular edema and choroidal neovascularization secondary to AMD indicated retinotoxicity and inflammation. 10 That study was done on diabetic and AMD patients but not for uveitis. Diabetes and AMD may change microperimetry indices over time. Retinal vasculopathy in diabetic patients may increase inflammation in some patients.
Our study was done on chronic noninfectious refractory uveitis. We evaluated visual acuity, grade of vitritis, and CMT as the main outcome measurements. We did not use microperimetry. It can be mentioned that, in short term, infliximab may improve visual acuity and decrease CMT in patients with chronic noninfectious uveitis. In long term, we had relapse of disease without significant deterioration of the main outcome measurements in comparison to measurements before treatment. It seems that its effect is not long lasting and multiple injections may be needed for achieving the best therapeutic goal.
In our previous study, the short-term effect of infliximab was taken into consideration. 9 We found a dramatic improvement of vision and decrease in the CMT and vitritis of all the eyes that were treated with intravitreal infliximab. No significant ophthalmic or systemic complications were detected except for mild subconjunctival hemorrhage.
Some reports are present about successful treatment of sarcoid refractory noninfectious uveitis with Adalimumab, the other TNF-α antagonist, but some reports are present about the proinflammatory effects of etanercept, a TNF-α inhibitory drug. That study showed long-term remission after change from etanercept to infliximab.17,2
Infliximab does not appear effective in diabetic macular edema.18,10 In diabetes the pathogenesis of edema may be different. In uveitis, free TNF-α may be present in the vitreous and infliximab may attach to it immediately after injection, but in diabetes the level of TNF-α may be lower and immediate attachment may not happen and infliximab may act as an immune agent. This hypothesis may explain this difference but must be further investigated.
We had done a study that was published in the journal Retina (October 2010) on the same patients and followed them for 4 weeks and we reported the short-term effects of infliximab. 9 In the recent study, we followed the same patients for 6 months. During the follow-up, at first inflammation decreased during 4 weeks but after 3 months the inflammation increased gradually with deterioration of visual acuity, and after 6 months, with no alteration in other anti-uveitis drugs. The effect of infliximab seemed to vanish and deterioration of vision along with increased CMT and inflammation in all the treated eyes was observed. It seems that repeated injections between 3 and 6 months are needed for control of inflammation and during this period we can review, adjust the dosage of other drugs, and re-evaluate the systemic conditions of the patient.
According to our findings, no deterioration of visual acuity or inflammation was observed as compared with preinjection findings, and no significant ocular or systemic complications were detected.
The adverse effects of TNF-α antagonists must be balanced against the potential benefits in refractory uveitis patients. Clinical practice guidelines, criteria of introduction, duration, and type of treatment with TNF antagonists, including safety issues, must be under constant revision as data from longer periods of patient exposure accumulate.
Footnotes
Acknowledgment
The authors would like to thank Dr. Golsa Madadi, Dr. Nasrin Shokrpour, and Dr. Mohammad Afarid for development of clinical studies and editorial assistance.
Author Disclosure Statement
The author(s) have no proprietary or commercial interest in any materials discussed in this article.