
Abstract
Abstract
Purpose:
The aim of this study was to evaluate the intraocular pressure (IOP) increasing effect and bioavailability of triamcinolone acetonide (TA) microspheres, as a novel drug delivery system, after intravitreal administration.
Methods:
Microspheres loaded by TA were prepared by the solvent evaporation method. After encapsulation, the final microspherical formulation was tested in an animal model. The left eyes of rabbits received microspherical TA and the right eyes were injected with conventional TA suspension. The drug concentration in the vitreous samples at days 7, 14, 28, and 56 after the injection was determined by high-performance liquid chromatography. The IOP was also checked at the same days with the Schiotz tonometer.
Results:
There was no statistically significant (P>0.05) difference between mean concentration of TA in the vitreous of right and left eyes at the different sampling times except day 56. Mean IOP of eyes that received microspherical TA was increased less than that of the eyes injected with TA suspension, and the difference was statistically significant (P<0.05) for each measurement day. TA was detectable in both eyes after 8 weeks. Both TA microsphere and suspension showed the sustained release profile.
Conclusion:
The results of this study showed less IOP increasing effect of triamcinolone microspheres in comparison with suspension form.
Introduction
The most commonly reported complication of intravitreal administration of TA is elevation of intraocular pressure (IOP). Bakri and Beer showed that, after a single IVTA injection, 48.8% of the eyes demonstrated an increase in IOP of 5 mm Hg or more, and 27.9% of patients experienced an increase in IOP of 10 mm Hg or more. 12 In another study, Smithen et al. showed that IOP elevation after IVTA administration was common with rates ranging from 20% to 60%. 13
Despite the high incidence, up to 50%, there is no consensus about the cause of IOP rise. 14 Im et al. found that two-thirds of eyes with clinically significant IOP elevation after IVTA administration developed gonioscopy changes, characterized by particulate matter in the inferior angle, which was not present at the baseline examination. Presence of this particulate matter might be related to poor solubility and precipitation of suspension particles in trabecular meshwork. 15
Microspheres are defined as colloidal systems made of solid polymers and falling in the size range of 1–1,000 μm.16,17 They comprise a polymeric matrix with drug molecules distributed inside the matrix. 18 There are extensive microsphere preparations for delivery of a variety of drugs. 19 The controlled drug delivery systems such as microspheres have numerous advantages compared to conventional dosage forms, including improved homogeneity and solubility, improved efficacy, and reduced toxicity. 20
In the present study, microspheres containing TA were prepared and characterized. The vitreous drug concentration–time profile and IOP were determined in an animal model after intravitreal injection of TA suspension and TA microspheres.
Methods
Materials
PLGA 50:50 (Mw 40000-75000) was supplied by Sigma. TA was obtained from Iran Darou. Dichloromethane, acetone, and polyvinyl alcohol (PVA; Mw 27000) were purchased from Merck. All materials were of analytical grade unless otherwise stated.
Preparation of TA microspheres
Microspheres loaded by TA were prepared by the solvent evaporation method. 21 In brief, TA and PLGA were dissolved in dichloromethane. This solution was emulsified in 25 mL of an aqueous solution containing 0.3% w/w PVA using a homogenizer (Ultraturax, IKA) at 20,000 rpm for 5 min. This emulsion was left to be stirred for 24 h. The microspheres were collected by centrifugation at 14,000 g for 10 min. To remove any residue of PVA, microspheres were washed twice with distilled water. Finally, microspheres were vacuum dried in a freeze dryer (Heto, DW3).
Characterization of microspheres
The shape and surface characteristics of microspheres were examined by scanning electron microscope (SEM) (LEO, 1450 VP). Mean diameters and particle size distribution of microspheres were measured by the particle size analyzer (Malvern nano-ZS) after suitable dilution with double-distilled water.
Determination of encapsulation efficiency
To determine encapsulation efficiency, a weighed amount of TA-loaded microspheres was dissolved in acetone; after filtration through 0.45-μm filter, 20 μL of this solution was injected into high-performance liquid chromatography (HPLC). The HPLC system consisted of a pump and the UV detector. The mobile phase was acetonitrile:water (36:64) with flow rate of 1 mL/min. The UV detector was set at 240 nm. A calibration curve for standard solutions was plotted over the range 0.00032–0.2 mg/mL.
Animal studies
The animals used in this study were normotensive New Zealand albino rabbits, weighing 1.8 to 2.0 kg. Rabbits were sedated with an intramuscular injection of ketamine hydrochloride (60 mg/kg) and xylazine hydrochloride (6 mg/kg). Eyes were anesthetized with topical administration of 1% tetracaine ophthalmic drop, and then IOP was checked with the Schiotz tonometer. Before the intravitreal injection, povidone iodine 5% was applied on the surface of the eye for 2 min. After washing with a balanced salt solution, the eyes of each rabbit received an intravitreal injection of 4 mg TA, 2.5 mm behind the limbus in the superotemporal quadrant using a 30-gauge needle. Left eyes were injected with TA microspheres, and right eyes received TA suspension. Among different microspherical formulations, microspheres with highest encapsulation efficiency were chosen for injection. Both eyes were injected with the same concentration of TA. Volume of injection was 0.1 mL. Microsphere powder was diluted by isotonic phosphate buffer to provide the same concentration. The same volume of sample was injected to both eyes. Rabbits were killed at days 3, 7, 14, 28, and 56 after the intravitreal injection, 3 animals each day. Both eyes were immediately enucleated, and aqueous humor was aspirated with a 30-gauge needle via an anterior limbal parasynthesis. Then, the corneas were cut off, the crystalline lenses were removed in an open-sky extracapsular cataract extraction fashion, the posterior capsule of the lens and the anterior hyaloids face were severed, and the whole of the vitreous was aspirated. 22 The animal protocol was approved by the local ethics committee.
All samples were then immediately frozen at −80°C. Before quantitative analysis, samples were defrosted overnight at 4°C. TA concentrations were measured by HPLC. For extraction of TA from vitreous samples, the method described by Kim et al. was used. 23
IOP measurements
IOP was measured using the Schiotz tonometer before the intravitreal injection on the first day and then at days 7, 14, 28, and 56. Before each measurement, rabbits were sedated and one drop of tetracaine (0.5%) was applied onto the cornea. The upper and lower eyelids were retracted, and the tonometer was brought into contact with the center of the cornea. At least 2 readings were taken from each eye.
Statistical analysis
Data are expressed as mean±SD. Test was performed using unpaired t-test. The P value less than 0.05 was considered to be statistically significant.
Results
Microspheres were spherical in shape (Fig. 1). Table 1 shows the mean size and encapsulation efficiency data of different formulations. Microsphere mean size ranged from 1.9 to 3.2 μm. Encapsulation efficiency ranged from 50% to 85% in different formulations.
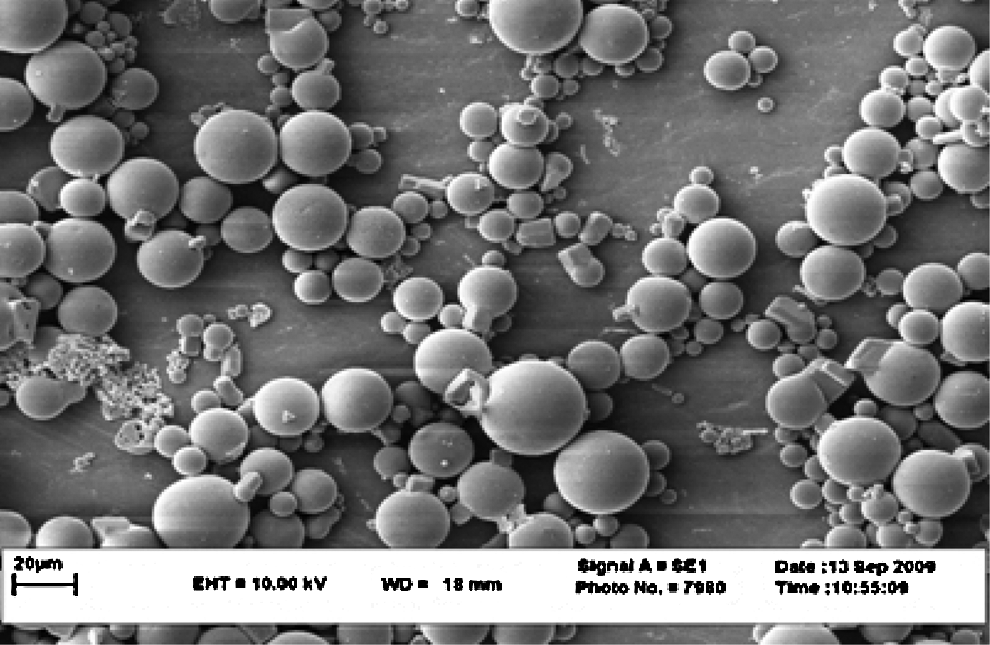
Scanning electron micrographs of microspheres containing triamcinolone acetonide (TA).
Figure 2 shows the change in the TA concentration over time in the vitreous of the injected eyes for both TA microsphere and suspension. Although the mean concentration of TA in eyes injected by microspheres was almost lower than that of suspension at different intervals, the differences were not statistically significant except for day 56. After 1 week, the vitreous concentration of TA was 0.047±0.012 and 0.083±0.067 mg/mL in eyes that received TA microsphere (left eye) and TA suspension (right eye), respectively (P=0.4173). The vitreous concentration of TA declined to 0.009±0.004 and 0.031±0.019 mg/mL after 1 month for left eye and right eye (P=0.1254). The final concentration after 2 months of administration was 0.001±0.0006 and 0.015±0.007 mg/mL in the eyes that received TA microspheres and TA suspension, respectively. This was the only statistically significant difference of TA concentration between right and left eyes (P=0.0370). The area under the drug concentration–time curve (AUC) was 7.874 and 9.019 mg×day/mL for TA microspheres and TA suspension, respectively. Also, calculation of drug clearance showed that the clearance of TA from vitreous after using suspension formulations (0.422 mL/day) was slower than the microspherical form (0.508 mL/day).

Triamcinolone concentration in the vitreous after the intravitreal injection of 4 mg of drug (mean±SD, n=3). Left eyes received triamcinolone microspheres, and right eyes were injected with the triamcinolone suspension.
Figure 3 shows the variation in IOP in different intervals after the intravitreal injection. There were no significant (P>0.05) differences between IOP in both eyes before injections. The IOP gradually increased up to 2 weeks after the injection. Two weeks after injections, mean IOP was 35.40±3.11 and 43.06±0.57 mmHg in eyes that received TA microspheres (left eye) and TA suspension (right eye), respectively (P=0.0138). After that time, the reduction in IOP was observed, but the IOP was statistically significantly (P<0.05) lower in the TA microspheres group compared to the TA suspension group. Fifty-six days after injections, mean IOP was 22.27±4.81 mmHg for left eyes and 34.87±6.74 mmHg for right eyes with the significant P of 0.0227.

Variation in intraocular pressure (IOP) in left and right eyes 7, 14, 28, and 56 days after the intravitreal TA injection.
Discussion
Microspheres have been used as carriers for different drugs, including antimicrobial, chemotherapeutic, and anti-inflammatory agents such as corticosteroids.24,25 As it was mentioned before, the use of biodegradable microspheres as drug delivery systems offers several important advantages, including controlled drug release and improved biodegradability and biocompatibility.26,27
Several factors influence drug release from microspheres, including polymer type and its molecular weight, physicochemical properties of drug, drug loading, and microsphere size. Normally, the drug release rate from small microspheres is faster than larger ones. 25 Although, in the present study, microspheres released TA in a sustained manner, the vitreous concentration of TA declined faster compared to the suspension form. These results can be related to this point that smaller particles may potentially exhibit more migration throughout the vitreous cavity. In addition, as we did not take the vitreous sample in very early postinjection, we could not confirm whether the difference began exactly after the injection or the clearance of TA made the difference.
As previously mentioned, the most important adverse reaction to the administration of IVTA is elevation of IOP. Some authors advocated treatment with topical steroids to determine steroid-responders. Unfortunately, this provocative screening test does not correlate with IOP rise after IVTA administration. In Massin et al. study, despite the negative provocative test, 50% of patients had an increased IOP after their intravitreal injection. 28 This might be related to the selection bias of the exclusion of patient with higher IOP.14,28
In several studies, white particles were found in the anterior chamber and angle after the IVTA injection in correlation with an IOP rise.15,29 It might be related to spillover of TA into the anterior chamber and reduction of an outflow facility of the trabecular meshwork. Results of our study are in concordance to this theory. Despite statistically insignificant differences of TA concentration in 2 eyes up to 1 month after the IVTA injection, we found statistically significant (P<0.05) differences in IOPs in all measuring days. We could relate the reduction in IOP to more homogeneity of the microspherical form of TA.
In addition, use of a more homogenous preparation is also better for intravitreal administration, as in this case more rapid resolution of vitreous opacities can be achieved. We checked the clarity of 2 TA formulations after shaking. TA suspension preparation showed a cloudy appearance, but TA microspheres were clear over the specific time. This caused reduction of red reflex in eyes treated by the TA suspension even 56 days after the IVTA injection in comparison with microspherical TA (Fig. 4). Floaters are the well-known complication after the TA injection. As the TA suspension is not clear, it blocks and scatters incoming light and the patient usually complains about visual floaters.30,31 Clarity and homogeneity of microspherical form of TA might also reduce these common complaints.
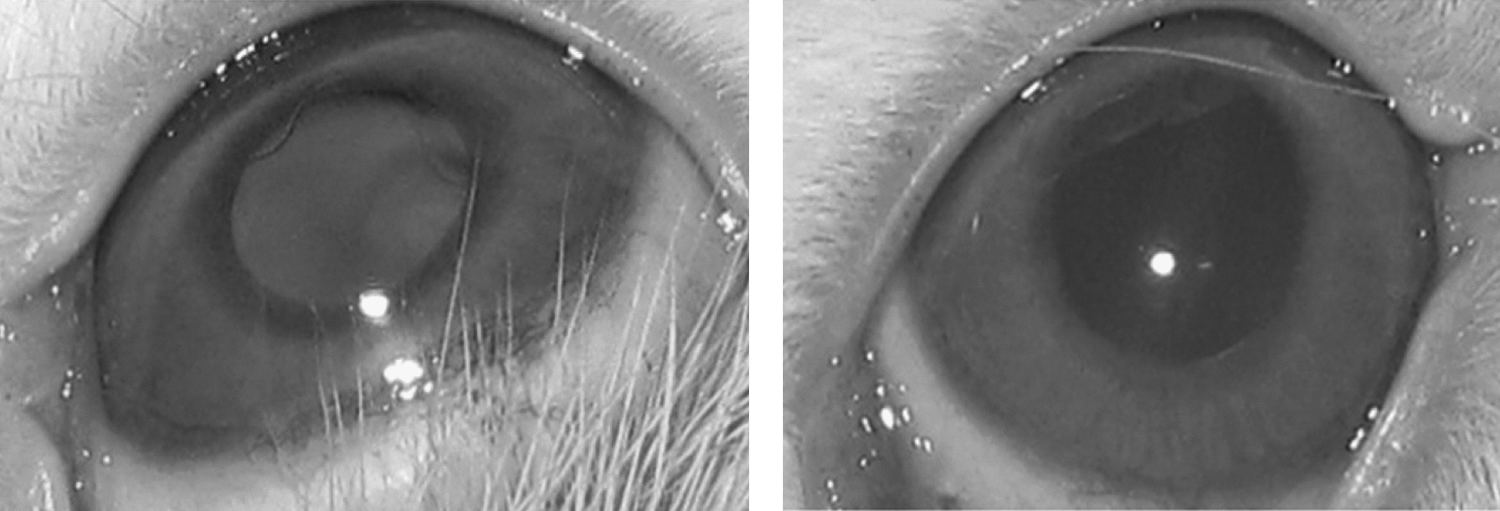
Right: Decrease red reflex 56 days after the intravitreal TA suspension injection. Left: Normal red reflex 56 days after the microspherical TA injection.
Conclusion
TA was released from microspheres in a sustained manner in the vitreous. In the present study, microspheres caused less IOP elevation after the intravitreal injection.
Footnotes
Acknowledgment
This work was supported financially by a research grant from the Vice Chancellor for Research of Mashhad University of Medical Sciences, Mashhad, Iran. The results described in this article were part of a PharmD student thesis.
Author Disclosure Statement
The authors declare that there is no conflict of interests in this study.