
Abstract
Abstract
Purpose:
Report the use of bevacizumab intralesional injection as an adjunctive therapy in a patient with ocular surface squamous neoplasia (OSSN) after an incomplete response to topical and intralesional chemotherapy.
Methods:
This is a case report of a 79-year-old man who was treated with topical and intralesional chemotherapy (interferon-alpha-2b, mitomycin-C, and 5-fluorouracil) over 22 months with incomplete resolution of severe OSSN. Intralesional bevacizumab was tried as an adjuvant treatment to resolve the residual tumor.
Results:
Grossly and histologically there was no significant change in the residual tumor after treatment with intralesional bevacizumab.
Conclusions:
While intralesional bevacizumab has been utilized as a treatment modality in the use of other squamous tumors, further studies on the use of bevacizumab in squamous neoplasia would be needed to recommend this treatment for the ocular surface. In the absence of further studies, the current topical and intralesional chemotherapeutic agents should continue to be the mainstay of medical treatment for squamous neoplasia; surgical management is still the definitive treatment.
Case Report
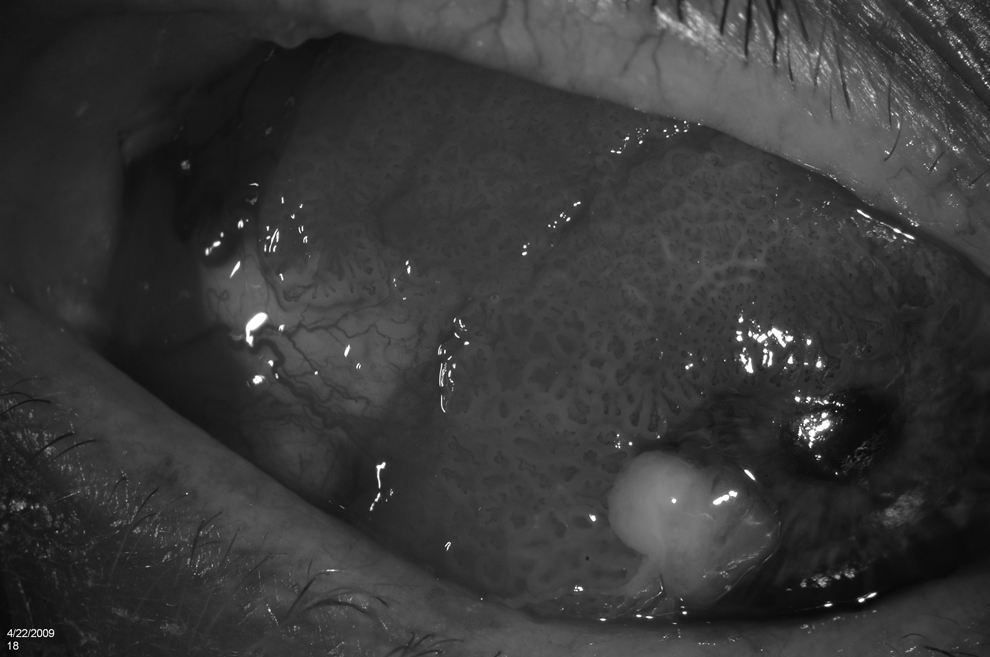
External photo of right eye ocular surface with extensive disease of the bulbar and palpebral conjunctiva. A leukoplakic lesion at the infero-temporal limbus and extensive papilliform extension of the conjunctiva onto the cornea are shown (photo courtesy Donald U. Stone, M.D.).
Initial work-up included a B-scan ultrasound and anterior segment ultrasound biomicroscopy, which did not reveal obvious intraocular extension. The patient had recently undergone multiple recent vascular surgeries and discontinuation of clopidogrel was deemed high risk; an incisional conjunctival biopsy was offered to determine if the lesion was a viral papilloma or squamous neoplasia. The biopsy of the temporal limbal tumor demonstrated moderate to severe dysplastic cells giving a presumptive diagnosis of severe ocular surface squamous neoplasia (OSSN).
After discussion of the risks of intraoperative bleeding with concurrent antiplatelet therapy, juxtaposed against the medical risks of discontinuing the clopidogrel, the patient elected to proceed with medical intralesional and topical chemotherapeutics. At this initial visit, the patient was treated with subconjunctival Interferon-alpha-2b and placed on Interferon-alpha-2B ophthalmic topical therapy, 1 million units/mL 4 times a day. The patient's lesion regressed over the following 8 months. At 10 months, the lesion's regression halted and he was placed on mitomycin-c 0.2 mg/mL 4 times a day; the patient developed severe conjunctivitis and dermatitis after two 1-week cycles of this therapy and it was discontinued. At 13 months, cryotherapy was used at the residual bulbar lesion and the patient was given intralesional mitomycin-c 0.2 mg/mL. By 18 months, the bulbar lesion had regressed incompletely. Topical mitomycin-C was restarted at this time, with no clinical effect noticed after four 1-week on/off cycles. At 20 months, an intralesional interferon-alpha-2b injection was given.
The patient returned at 22 months with worsening disease at which time 5-fluoruracil (5-FU) 5 mg/mL topical therapy was started 4 times daily, with no apparent improvement after 1 month. At 23 months intralesional bevacizumab 1.25 mg (0.05 mL) was injected into the residual palpebral lesion (Fig. 2). After 4 weeks, there was no clinically apparent change. At this point the patient confided that he had discontinued the clopidogrel without advising his treating physicians; prior to restarting it, the patient was taken to the operating room for excision of the residual tumor with amniotic membrane graft.

External photo of right eye and palpebral conjunctiva at 23 months after topical and intralesional chemotherapy shows residual palpebral lesion (photo courtesy Donald U. Stone, M.D.).
On review of the histology slides 4 weeks after the bevacizumab intralesional injection, there were signs of dysplasia arising in a papilloma, focal carcinoma in situ, and inflammation in the substantia propria, which are normal findings in OSSN (Fig. 3). No changes were seen that were interpreted as specific to the bevacizumab injection.
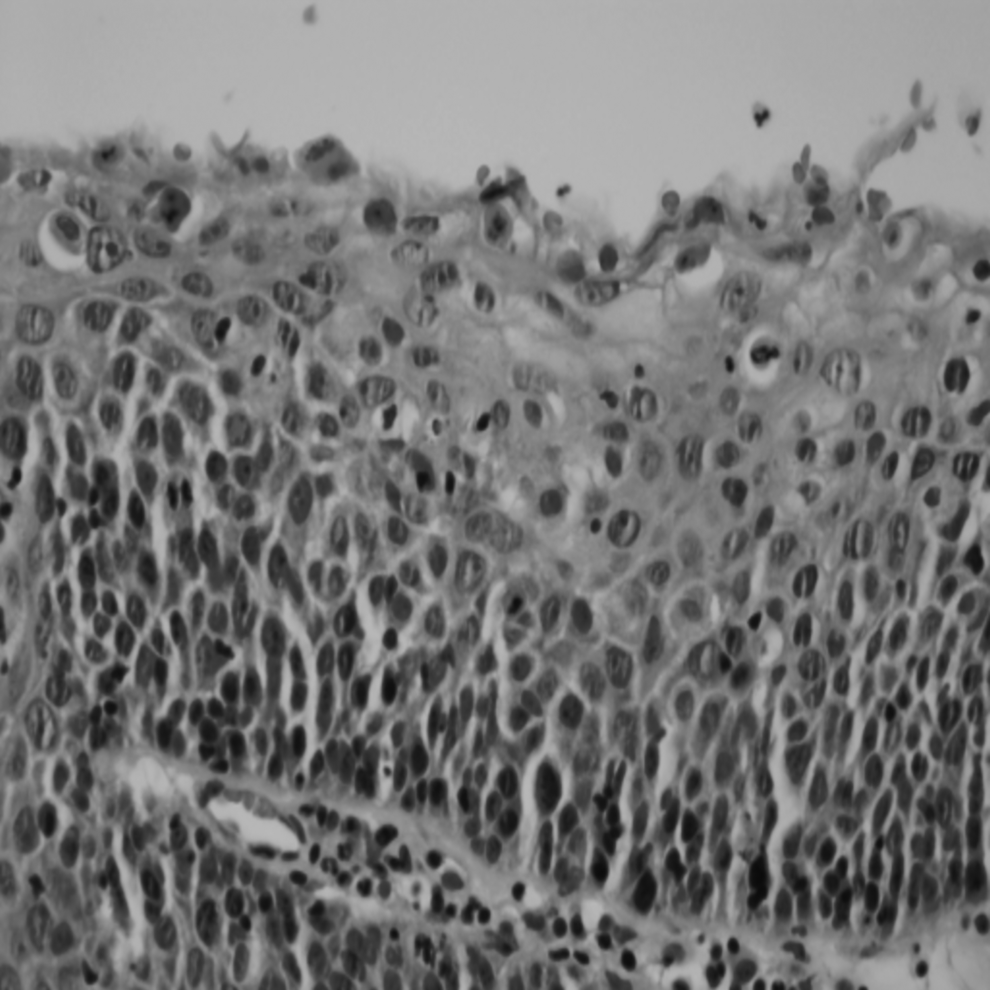
High magnification of the ocular squamous neoplasia with hematoxylin-eosin staining 4 weeks after intralesional bevacizumab (slide courtesy Hans Grossniklaus, M.D., Emory University).
Comment
Intralesional bevacizumab is not a previously reported treatment for OSSN.1,2 The management of this entity has changed from a surgical-first approach to a less-invasive approach since being first described by von Graefe in 1860. 3 Diagnostic testing, such as B-scan ultrasound and anterior segment ultrasound biomicroscopy, aid in confirmation that the lesion has not penetrated the intraocular structures but biopsy remains the modality of choice to assess pathology. Traditionally, excisional biopsy is utilized except for extensive lesions. 4 A wide conjunctival surgical margin of 4–5 mm with adjunctive cryotherapy is recommended to increase the chances of complete removal, with absolute alcohol used to remove the corneal aspect of the tumor. 5
Controversy remains over the necessity of a biopsy before initiating topical or intralesional chemotherapy, and what is the best first-line treatment. 6 Topical chemotherapy has several advantages when compared with traditional surgical excision and cryotherapy. 7 These include treatment of the entire ocular surface and avoidance of surgical risks. Interferon also offers the potential advantage of relative targeting of the tumor cells, reducing the risk of limbal stem cell deficiency associated with mitomycin or extensive surgical excision of the limbus. Disadvantages include limited penetration and potential for failure in eradicating disease when used as the sole agent in invasive squamous cell carcinoma. 8 Topical mitomycin-C and 5-FU have shown efficacy in the treatment of recurrent and primary OSSN.9–18 Recently, interferon treatments have been at the forefront of less-invasive treatments for OSSN. Chodosh and coworkers suggested that both topical interferon-alpha-2b and meticulous surgical excision are effective for OSSN. 19
Comparing medical chemotherapy treatments, Poothulli and Colby showed that rates of tumor regression for intraepithelial neoplasia and squamous cell carcinoma ranged from 80% to 96% after an average follow-up of 27 months. 20 This promising data for noninvasive treatment of OSSN allows an alternative for definitive treatment of this disease in patients who are at risk for bleeding during surgical excision or are at increased risk for complications from anesthesia.
In our case, the patient had a recent history of multiple vascular surgeries, which required the use of clopidogrel. Thus, the decision was made to treat the neoplasia with topical chemotherapeutics. After months of topical and intralesional chemotherapy, a residual palpebral tumor remained. This lesion was treated with intralesional bevacizumab and after 4 weeks did not demonstrate any further resolution. To our knowledge, this is the first such case to be reported. There are promising reports of the chemotherapeutic potential of anti-VEGF (vascular endothelial growth factor) agents in the treatment of squamous neoplasia in other anatomic locations, as VEGF is found to be a key promoter in certain squamous neoplasia, but in our case of refractory OSSN there was no apparent benefit.1,2 Thus, a favorable outcome to treatment may not have been forthcoming and we did not repeat treatment or increase dosing. This adjunct treatment was attempted after refractory findings from other treatment modalities. These findings support that topical and intralesional chemotherapeutic agents should continue to be the mainstay of medical treatment for OSSN, and meticulous surgical excision is still the definitive treatment. We recognize that both the brief follow-up period and the complexity of this single case report can be viewed as insufficient evidence regarding efficacy in refractory management of OSSN. We recommend further studies, including modified approaches of combination therapy, prior to the use of modified intralesional bevacizumab as adjunct therapy in the management of OSSN.
Footnotes
Acknowledgments
Supported in part by an unrestricted grant from Research to Prevent Blindness to the Department of Ophthalmology, University of Oklahoma. No author has a financial interest in any technique or product mentioned in this article.
Author Disclosure Statement
No competing financial interests exist.