
Abstract
Abstract
Purpose:
Benzalkonium chloride (BAK), a common preservative in eye drops, can induce ocular surface toxicity that may decrease glaucoma therapy compliance. The ocular hypotensive effect, pharmacokinetic (PK) profiles, and local tolerance of a preservative-free latanoprost 0.005% cationic emulsion (Catioprost®), and a BAK-preserved latanoprost 0.005% solution (Xalatan®), were compared.
Methods:
The ocular hypotensive effect was evaluated in monkeys with elevated intraocular pressure (IOP) induced by laser photocoagulation of the trabecular meshwork. Each monkey (n=8) received both latanoprost formulations once daily for 5 consecutive treatment days in a crossover design with at least a 2-week washout period between treatments. IOP was measured at baseline (on day 1, no instillation), on vehicle treatment day (day 0), and on treatment days 1, 3, and 5 before drug instillation and then hourly for 6 h. In rabbits, the ocular and systemic concentrations of latanoprost free acid were determined following a single instillation and the local tolerance of twice daily instillations over 28 days was assessed.
Results:
Both the preservative-free and BAK-preserved latanoprost formulations shared the same efficacy profile with the maximum IOP reduction occurring 2 h after each morning dose (−15%, −20%, and −26%; −15%, −23%, and −23% on days 1, 3, and 5, respectively) and lasting through 24 h. The equivalence in efficacy was confirmed by the PK data demonstrating similar area under the curves (AUCs). While both formulations were well tolerated, the incidence of conjunctival hyperemia was reduced by 42% with the BAK-free latanoprost cationic emulsion.
Conclusions:
In animal models, a preservative-free latanoprost cationic emulsion was as effective as Xalatan® for lowering IOP with an improved ocular tolerance profile.
Introduction
Iatrogenic toxicity of benzalkonium chloride (BAK) in preserved eye drops has been extensively described.5–8 The deleterious effects of BAK on the ocular surface have been demonstrated in vitro, in animal models and in humans. BAK has a detergent effect on the lipid layer of the tear film, 9 is proinflammatory, and induces goblet cell apoptosis. 10 It has been described that up to 60% of patients with glaucoma have signs and symptoms of ocular surface disease. 11 As a consequence, there is a reasonable interest in the development of BAK-free glaucoma therapies to reduce the risk of iatrogenic toxicity to the ocular surface. 12
Preservative-free cationic emulsions were developed to improve the delivery of locally applied therapies for the treatment of ophthalmic diseases. Cationic emulsions consist of small oil droplets (<200 nm in size) stabilized by a lipophilic cationic surfactant––which brings a positive charge (+40 mV) to the emulsion––dispersed in an isotonic water solution containing an emollient. 13 The concomitant actions of the oil and aqueous phases of the emulsion provide lubrication to the ocular surface while restoring the muco-aqueous and lipid tear layers and preventing evaporation of the tear film. 13 Since latanoprost is readily soluble in oil, it was of interest to exploit the benefits of the cationic emulsion on the ocular surface to improve the delivery and overall tolerability of latanoprost.
In the present report we present the findings of nonclinical efficacy and safety studies comparing a preservative-free latanoprost 0.005% cationic emulsion to Xalatan®, a commercialized BAK-preserved latanoprost 0.005% solution.
Methods
Reagents and latanoprost cationic emulsion characteristics
All solvents and excipients were of high performance liquid chromatography (HPLC) grade, while chemicals and reagents were of analytical grade and excipients conformed to United States Pharmacopeial Convention standards. The composition and characteristics of the preservative-free latanoprost 0.005% cationic emulsion are summarized in Tables 1 and 2, respectively.
Droplet size was determined by dynamic light scattering (HPPS; Malvern Instruments), and zeta potential by electrophoretic mobility measurement (Zetasizer 2000; Malvern Instruments).
Animals
All animals were treated according to the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research (ARVO Handbook, 1993). Adult female cynomolgus monkeys used for the efficacy study were from Charles River Laboratory (Wilmington, MA), and were part of a population of monkeys housed at Mount Sinai School of Medicine (New York, NY). The efficacy study protocol was approved by the Institutional Animal Care and Utilization Committee of Mount Sinai School of Medicine. Male and female adult New Zealand white rabbits (2–2.5 kg) were obtained from Grimaud (Roussay, France). Following a thorough ocular examination the rabbits were randomly assigned to groups for subsequent pharmacokinetic (PK) and local tolerance studies. Animals were housed individually in standard cages, with food and water ad libitum, and kept under 12-h light and darkness cycles throughout the study. At predefined time points (PK study) and on completion of the 28-day observation period, the animals were anesthetized and humanely sacrificed.
Efficacy evaluation of a preservative-free latanoprost 0.005% cationic emulsion in glaucomatous monkey eyes
Eight adult female Macaca fascicularis weighing 3–6 kg were used in this study. Elevated IOP was induced by diode (50–120 spots; power 1.2 W; size 75 pm; duration 0.5 s) laser photocoagulation of the midtrabecular meshwork in 1 eye of each monkey, while the contralateral eye remained untreated. 14 Each monkey received both latanoprost formulations once daily (30 μL, at 09:30 am) for 5 consecutive days in a cross-over design with at least a 2-week washout period between treatments. The IOP was measured at baseline (day 0), on vehicle-treated glaucomatous eyes, and on treatment days 1, 3, and 5—immediately before drug instillation, and then hourly for 6 h with a calibrated pneumatonometer (Mentor, Model 30 Classic, Norwell, MA). The technician taking the measurement was not masked, 1 measurement was taken at each time point, and the measurement was acceptable when the standard deviation (SD) was <0.05 mmHg. Five minutes before tonometry, 1 drop of 0.5% proparacaine hydrochloride was applied topically, and ketamine hydrochloride 2–5 mg/kg of body weight was administered intramuscularly for adequate sedation. Slit-lamp examinations for the detection of aqueous humor flare and cells were performed in a dark room before drug treatment and 1, 3, and 5 h after drug instillation on treatment days 1, 3, and 5.
Ocular PK profile of latanoprost and latanoprost free acid in the rabbit
Seventy-two New Zealand white rabbits were allocated into 2 groups of 36 rabbits; each group was divided into 6 subgroups (1 for each time point) of 3 males and 3 females. The rabbits received 30 μL of either the unpreserved latanoprost cationic emulsion or Xalatan® in both eyes. Both formulations were applied in the lower conjunctival cul-de-sac of both eyes of each animal. Following the instillation, the eyelids were gently held together to prevent loss of the instilled elements. Ocular tissues (conjunctiva, cornea, ciliary body, and aqueous humor) were harvested 0.25, 0.5, 1, 4, 6, and 24 h postinstillation for latanoprost and latanoprost free acid determination. In addition, at the first 3 time points, blood was collected to assess the systemic passage of both latanoprost and latanoprost free acid.
Local tolerance evaluation of repeated instillations of a preservative-free latanoprost 0.005% cationic emulsion in the rabbit
Twenty-four New Zealand white rabbits were randomly assigned to 3 groups of 4 males and 4 females. Latanoprost cationic emulsion, Xalatan®, or normal saline (0.9% NaCl) was instilled twice daily (30 μL), 6 h apart, for 28 consecutive days into the right eye. The contralateral eye of each animal served as an absolute control. Complete ophthalmoscopic examinations were performed in all animals at baseline, on day 12, and at the end of the treatment period. The conjunctiva, cornea, and iris of both eyes of all animals were examined daily before the first instillation and 1 h after the second application by direct examination in white light. Findings were graded using the Draize scale as well as other ocular irritation tests, as defined in part 10 “Tests for irritation and delayed-type hypersensitivity” of the standard EN ISO 10993-10–February 2003. Corneal lesions were further evaluated with fluorescein.
At the end of the 28-day treatment period, and 15 min after the last instillation, blood was collected to quantify both latanoprost and its free acid form in plasma. Local and general toxicities were performed during the course of the experiment, while at sacrifice a gross necropsy and complete histology of the eyes and nasal mucosa were performed. Following sacrifice, both eyes of each animal and the nasal mucosa of the treated group animals were subjected to a full histopathological examination.
Ultra performance liquid chromatography and high performance liquid chromatography-tandem mass spectrometry methods for latanoprost and latanoprost free acid determination in ocular tissues and plasma
The validation for each matrix conformed with the Food and Drug Administration (U.S. Department of Health, 2001) and the Société Française des Sciences et Techniques Pharmaceutiques15–17 guidelines, and evaluated the following: the specificity, the analysis of the response function, the selection of the most appropriate regression model, the assessment of trueness, the precision (repeatability and intermediate precision), the accuracy over the concentration range, the determination of the lower limit of quantification (LLOQ) and limit of detection, the study of linearity, and the estimation of analyte recovery. For both latanoprost and latanoprost free acid, the LLOQs were 5 pg/μL in aqueous humor; 5 pg/ng in the cornea, conjunctiva, and ciliary body; and 30 pg/mL in plasma.
Data analysis and statistical methods
The ocular tissue concentration data from the PK and toxicokinetic studies are presented as mean±SD and expressed in pg/mg or pg/μL, and pg/mL, respectively. Microsoft Excel® software was used to calculate AUCs and two-tailed Student's t-test for statistically significant differences between groups for latanoprost free acid concentrations (mean±SD), and IOP mean is presented as mean±standard error of mean (SEM).
Results
Ocular hypotensive effect of a preservative-free latanoprost 0.005% cationic emulsion (Catioprost®)
Once daily administration of a preservative-free latanoprost 0.005% cationic emulsion (30 μL/day) reduced IOP from 1 to 6 h after the first dose (Fig. 1). On treatment days 3 and 5 a reduction in IOP was observed at 0 h prior to the morning dosing through 6 h. The IOP reduction at 0 h indicates that the duration of IOP reduction was at least 24 h after the second and fourth dose. The maximum reduction in IOP occurred 2 h after each morning dose of the latanoprost cationic emulsion and was 4.4±0.5 mmHg (−15%), 5.9±0.5 mmHg (−20%), and 7.8±0.8 mmHg (−26%) on treatment days 1, 3, and 5, respectively. The same reduction in IOP was observed with once daily administration of Xalatan® (30 μL/day) for 5 consecutive days (Fig. 2). On treatment days 3 and 5 a reduction in IOP with Xalatan® was observed prior to the morning dosing and through 6 h and lasted at least 24 h after the second and fourth doses. Similar to the latanoprost cationic emulsion, the maximum reduction in IOP with Xalatan® occurred 2 h after each dose, and it was 4.3±0.6 mmHg (−15%) on treatment day 1, 6.5±0.5 mmHg (−23%) on treatment day 3, and 6.8±0.6 mmHg (−23%) on treatment day 5. The IOP reduction was enhanced by repeated dosing as compared with day 1; days 3 and 5 produced greater IOP reductions of longer duration for both latanoprost formulations. There was no significant difference in IOP reduction between either latanoprost formulation except at a single measurement point; at 6 h on treatment day 1 (P<0.05; Fig. 3A).
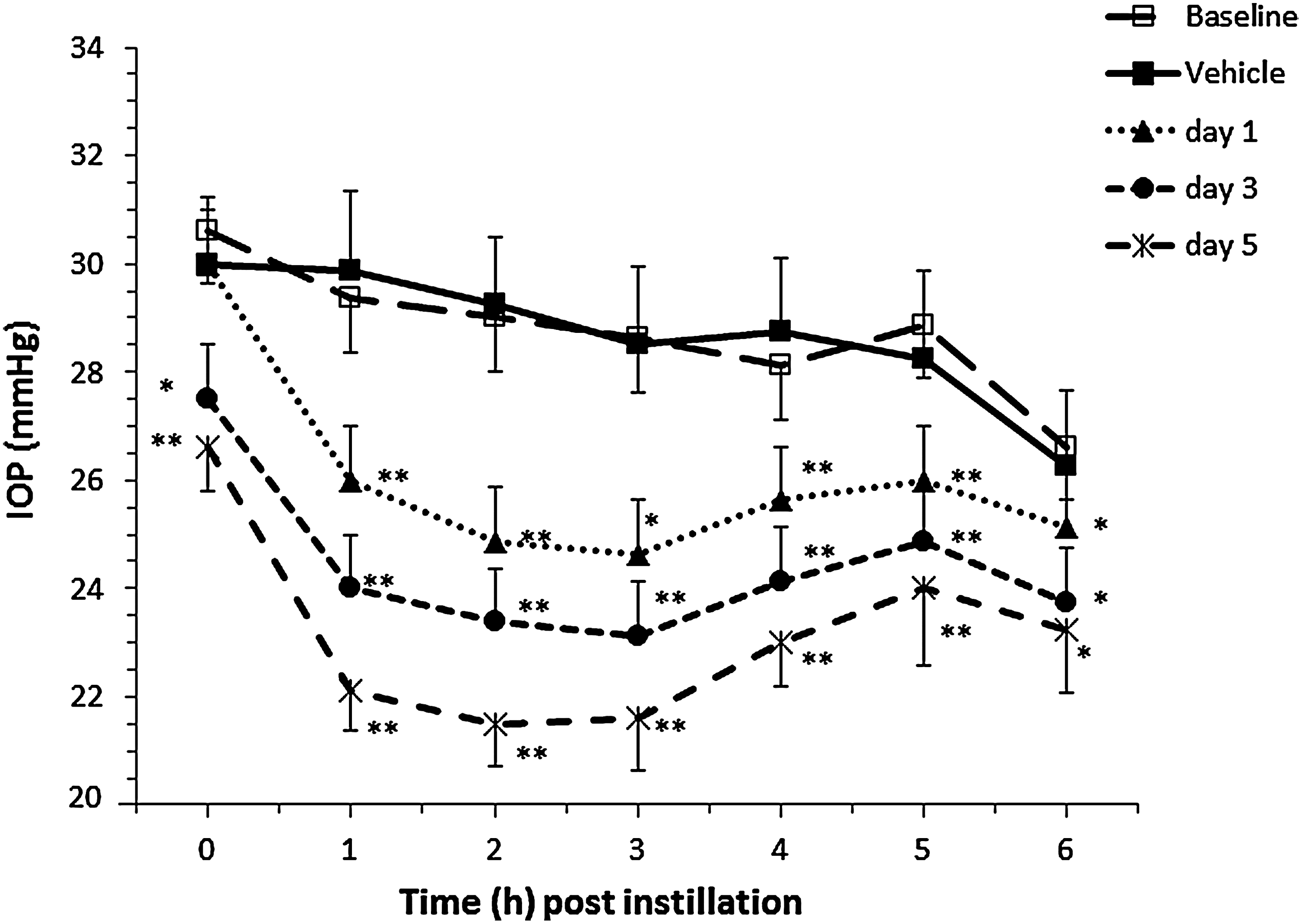
Effect on IOP at 1–6 h after morning dose of a 0.005% latanoprost cationic emulsion administered once daily for 5 consecutive days to 8 glaucomatous monkey eyes. Statistically significant reduction in mean IOP±SEM compared with vehicle treatment: *P<0.05; **P<0.001. Significant differences in IOP were not observed comparing baseline and vehicle-treated days for the latanoprost cationic emulsion (P>0.80). IOP, intraocular pressure; SEM, standard error of mean.
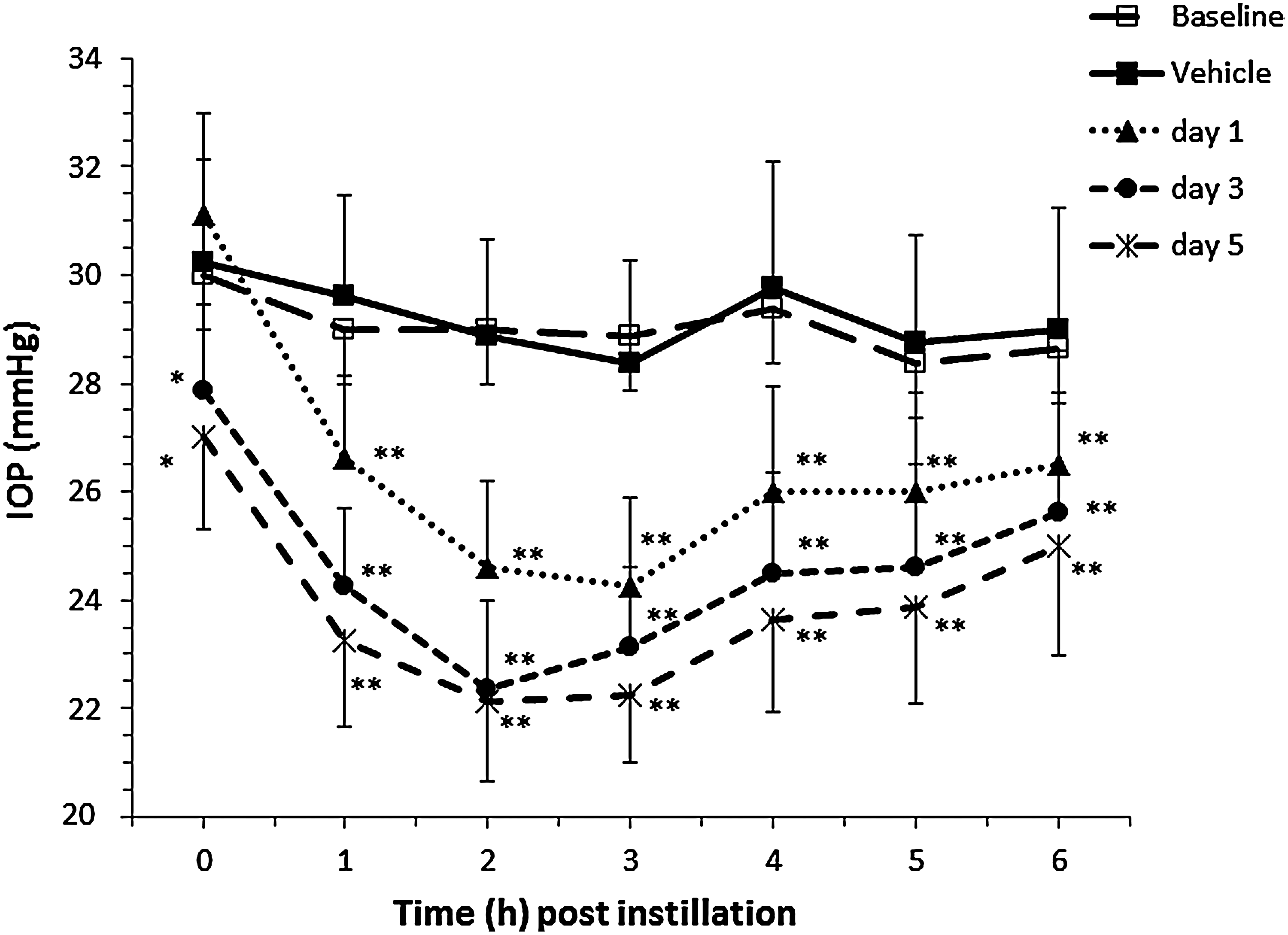
Effect on IOP at 1–6 h after morning dose of Xalatan® administered once daily for 5 consecutive days to 8 glaucomatous monkey eyes. Statistically significant reduction in mean IOP±SEM compared with vehicle treatment: *P<0.05; **P<0.001. Significant differences in IOP were not observed comparing baseline and vehicle-treated days for Xalatan® (P>0.80).

Comparison of the mean change in IOP in 8 glaucomatous monkey eyes after once daily administration of Xalatan® or 0.005% latanoprost cationic emulsion. Data show the mean change in IOP±SEM from vehicle baseline at day 1
Ocular and systemic PK profile following a single administration of a preservative-free latanoprost 0.005% cationic emulsion in the rabbit
Following the instillation of both latanoprost formulations, the prodrug latanoprost was rapidly hydrolyzed into latanoprost free acid (within minutes), and was not detectable in any evaluated tissues even at the shortest time point (0.25 h).
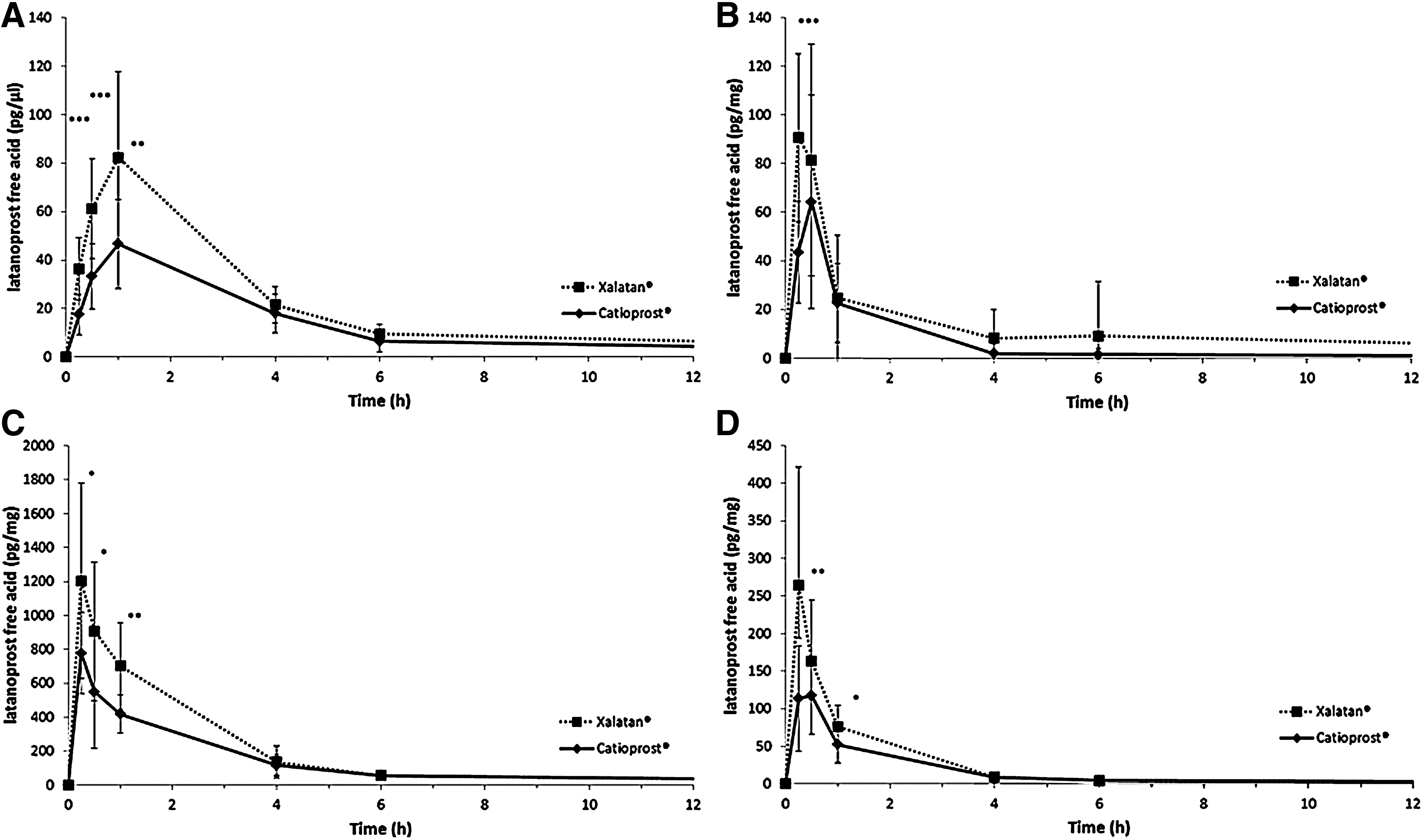
Ocular tissue latanoprost free acid levels demonstrated that the prodrug latanoprost is better absorbed after the instillation of Xalatan® than the latanoprost cationic emulsion (Fig. 4), as evidence by a shorter Tmax and better Cmax values (Table 3). It is well known that BAK (0.02% in Xalatan®) is not only a preservative, but also an effective permeation enhancer. Thus, the statistically (from P<0.05 to P<0.0001 depending on the tissue) better values observed for latanoprost free acid at the earlier time points (0.25, 0.5, and 1 h) after the instillation of Xalatan® were not surprising. It is noteworthy, however, that latanoprost free acid concentrations at the later 4 and 6 h postinstillation time points in both the cornea and ciliary body were not statistically different between the 2 latanoprost formulations (Fig. 4). For both formulations, latanoprost free acid was barely detectable 24 h postinstillation (data not shown).
Pharmacokinetic (PK) profile of latanoprost free acid in
AUC, area under the curve; Cmax, concentration maximum; Tmax, time at Cmax.
A comparison of the area under the curve (AUC) demonstrates that the latanoprost cationic emulsion yielded a lower overall exposure of latanoprost in the ocular tissues than Xalatan®. However, this difference was least in the cornea and ciliary body (Table 3), and from the 4 h time point to the end of the experiment both formulations had the same PK profile. Thus, except for the earliest time points, the PKs of the 2 latanoprost formulations were similar.
The systemic exposure of latanoprost following a single bilateral instillation was assessed by collecting blood samples 15, 30, and 60 min after the instillation (Table 4). The data demonstrated that the systemic exposure of latanoprost following either formulation was negligible as latanoprost plasma levels were below the LLOQ (30 pg/mL).
ILQ, inferior to the lower limit of quantification (LLOQ); LLOQ=30 pg/mL for both latanoprost and latanoprost free acid. In parentheses is the number of animals.
Local tolerance and safety of repeated instillations of a preservative-free latanoprost 0.005% cationic emulsion in the rabbit
Following twice a day instillations over 28 days, minor, transient conjunctival irritation (slight redness on palpebral and bulbar conjunctiva) was seen in 8% (0.9% NaCl, control group), 13% (latanoprost cationic emulsion), and 22% (Xalatan®) of treated eyes (Table 5). However, similar mild conjunctival irritation was observed in the untreated contralateral eyes of each group: 1.0% (0.9% NaCl), 3.0% (latanoprost cationic emulsion), and 0.5% (Xalatan®) of the observations.
N, normal; A, absent; +, less than a quarter of surface; /, not performed.
Observation at the end of the 28-day treatment period.
Number observation over the 28-day treatment period
All observations were of level 1 in the grading scale.
1=cornea ulceration (trauma); 2=cornea neovascularization; 3=conjunctivitis; in parentheses is the number of animals.
No significant findings were observed in the cornea and anterior chambers or during the ophthalmoscopic examination of any of the treated rabbits. Additionally, no significant treatment-related adverse findings were observed throughout the experiment on the basis of clinical signs and body weight with both test elements.
The microscopic examination of the treated eyes following sacrifice did not reveal any abnormal findings. Microscopic examination of the nasal mucosa from the animals treated with either latanoprost formulation revealed moderate irritation that was similar in the 2 groups with no difference between right (treated) and left (untreated) nasal cavities.
The systemic exposure (Table 4) of latanoprost and latanoprost free acid, as assayed in plasma samples collected 15 min after the last instillation of the 28th day of dosing, was negligible. Indeed, both latanoprost and latanoprost free acid plasma levels were below the LLOQ (30 pg/mL), or slightly above the LLOQ for latanoprost free acid in 1 animal (out of 8) treated with the latanoprost cationic emulsion (32.1 pg/mL) and in 1 animal (out of 8) treated with Xalatan® (33.9 pg/mL).
Thus, under these experimental conditions, that is, twice daily dosing for 28 consecutive days, the latanoprost cationic emulsion was as well tolerated as Xalatan® and appeared to induce less conjunctival irritation.
Discussion
Cationic emulsions are a new type of delivery vehicle designed to improve the bioavailability of topically applied lipophilic drugs for the treatment of ophthalmic diseases. As a result of the electrostatic interactions between the negatively charged cells of the ocular surface and the positive charge on the oily nanodroplets, cationic emulsions enhance the absorption of lipophilic drugs by prolonging their contact with the ocular surface. 18 In clinical trials, cationic emulsions with no active ingredient and containing cyclosporine, a lipophilic immunomodulator, have shown efficacy for the treatment of dry eye disease. In addition to improving cyclosporine delivery, the oil and aqueous phases of the cationic emulsion provide lubrication to the ocular surface while restoring and preventing evaporation of the tear film. 13 This beneficial effect of cationic emulsions underlies the rationale for a preservative-free latanoprost 0.005% cationic emulsion (Catioprost®) that was developed to improve the overall tolerability of latanoprost and address the emerging concern about ocular surface disease in patients with glaucoma and ocular hypertension requiring long-term, effective IOP-lowering therapy.
To investigate the potential benefit of a BAK-free latanoprost cationic emulsion, the formulation was compared with Xalatan®, a leading BAK-preserved prostaglandin analog, in nonclinical efficacy and safety models.
The ocular tissue absorption of both the latanoprost formulations was assessed following a single instillation in the rabbit. The data demonstrated that Xalatan® had a slightly greater ocular exposure than the latanoprost cationic emulsion, with AUC values in the conjunctiva, cornea, and ciliary body being, respectively, 38.6%, 31.2%, and 24.4% higher. This Xalatan® PK profile was in accordance with previously published results by Sjoquist et al. 19 However, it is interesting to note that this difference between the cationic emulsion of latanoprost and Xalatan® was at its lowest in the ciliary body, the main target tissue for glaucoma therapies. This difference between the 2 latanoprost formulations might be explained by the presence of 0.02% BAK in Xalatan®. BAK is a detergent preservative that at high concentration exerts toxic effects on the corneal and conjunctival epithelial cell membranes. Paradoxically, the potential advantage of the toxic effect of BAK on tight junction desmosomes is an improved ocular penetration of latanoprost. This is confirmed by the description and use of BAK as a permeation enhancer.
Compared with standard ophthalmic solutions, emulsions are known to have improved residence time in the precorneal area over standard solutions, 18 and cationic emulsions, through the electrostatic interactions with the negatively charged ocular surface, have an even better residence time when compared with negatively charged or neutral emulsions. Since the human ocular surface is more negatively charged than that of rabbits,20,21 the improved residence time of the cationic emulsion on the ocular surface may translate into greater ocular absorption of latanoprost cationic emulsion in patients than in rabbits.
The efficacy of the latanoprost cationic emulsion for reducing elevated IOP was confirmed in monkeys, whose eyes are anatomically and physiologically closer to human eyes than rabbit eyes. 22 In monkey eyes with elevated IOP, the latanoprost cationic emulsion was as effective as Xalatan® for reducing IOP (Figs. 1–3). It is noteworthy that 24 h after the second and fourth instillations (i.e., the first IOP measurement on days 3 and 5) IOP reductions achieved with the latanoprost cationic emulsion were identical to those obtained with Xalatan®. Thus, while some differences in the PK profile were observed, the pharmacodynamics of both formulations was identical. This suggests that there is no advantage of elevated peak concentrations reached immediately after the instillation of Xalatan® to obtain a maximal and sustained IOP reduction with latanoprost. On the other hand, lower latanoprost free acid concentrations in the conjunctiva and cornea following latanoprost cationic emulsion instillation might be expected to result in a lower incidence of ocular side effects, particularly conjunctival hyperemia, compared with that experienced with Xalatan®. This was confirmed by the 28-day ocular tolerance study (Table 5) that demonstrated that there was approximately a 42% decrease in the incidence of conjunctival redness with the latanoprost cationic emulsion compared with Xalatan®. Conjunctival hyperemia depends on the nature of the prostaglandin analog,3,4 that is, its concentration in the tissue, but may also be affected by the presence of BAK that is proinflammatory. The absence of BAK in the latanoprost cationic emulsion and its particular PK profile in conjunctiva (Fig. 4B) both advocate for the improved ocular tolerance profile of the cationic emulsion. A more favorable safety profile for the latanoprost cationic emulsion relative to Xalatan® was previously demonstrated in an acute in vivo rabbit toxicity model, 23 in which the latanoprost cationic emulsion did not induce any signs of toxicity on the rabbit ocular surface with results similar to those of PBS. Following multiple instillations of latanoprost cationic emulsion in this acute toxicity model, examination of the cornea, conjunctiva, and conjunctival-associated lymphoid tissue appeared normal, in contrast to Xalatan® instillations that induced ocular surface cytotoxicity and conjunctival inflammatory cell infiltrates attributed to the presence of 0.02% BAK. 23 The potential benefit of latanoprost cationic emulsion in eyes with ocular surface damage was also assessed in vivo in a rat model of de-epithelialization and in an in vitro wound healing model. 24 In rats, exposure of the damaged ocular surface to a 0.02% BAK solution and Xalatan® delayed the corneal healing process by inducing an inflammatory response, neovascularization, and corneal opacity. In contrast, the latanoprost cationic emulsion treatment seemed to accelerate the healing process (relative to the control). 24
Ocular surface disease, which manifests with signs and symptoms similar to dry eye disease in up to 60% of glaucoma patients, is an increasing concern in the long-term management of glaucoma and ocular hypertension.11,25 Ocular surface disease in glaucoma patients negatively influences quality of life and can compromise compliance with glaucoma therapy. 26 While the risk factors for ocular surface disease in glaucoma patients are also similar to those for dry eye disease, that is, increasing age, sex, menopausal status, environment, and systemic medications, iatrogenic toxicity as a result of the preservatives common in ophthalmic medications may largely explain the coincidence of glaucoma and ocular surface disease. This is supported by the higher rates of ocular surface disease in patients requiring multiple IOP-lowering medications. As the deleterious effects of BAK on the ocular surface have been clearly established, effective BAK-free glaucoma therapies could help to lower the risk of the ocular surface in patients with glaucoma and ocular hypertension.
In nonclinical efficacy and safety animal models, a preservative-free latanoprost 0.005% cationic emulsion was similar to Xalatan® for the reduction of IOP and appeared to have a more favorable ocular tolerance profile due to a lower incidence of induced conjunctival hyperemia. These findings suggest that the latanoprost cationic emulsion has the potential to be a very promising alternative glaucoma therapy for the long-term management of patients with glaucoma or ocular hypertension, particularly in patients already suffering from symptoms and/or signs of ocular surface disease.27–29
Footnotes
Disclosure Statement
P. Daull: Novagali employee; J.-S. Garrigue: Novagali employee; G. Lambert: Novagali employee; M.-O. Faure: Novagali employee; R. Buggage: Novagali employee; J. Serle: none; R.-F. Wang: none.